What is cardiography
The essence of cardiography is the study of electrical currents arising during the work of the heart muscle.
The advantage of this method is its relative simplicity and accessibility. Strictly speaking, a cardiogram is the result of measuring the electrical parameters of the heart, displayed in the form of a time graph. The creation of electrocardiography in its modern form is associated with the name of the Dutch physiologist of the early 20th century, Willem Einthoven, who developed the basic ECG methods and terminology used by doctors to this day.
Thanks to the cardiogram, it is possible to obtain the following information about the heart muscle:
- Heart rate,
- Physical condition of the heart
- The presence of arrhythmias,
- The presence of acute or chronic myocardial damage,
- The presence of metabolic disorders in the heart muscle,
- Presence of electrical conductivity disturbances,
- Position of the electrical axis of the heart.
Also, a cardiac electrocardiogram can be used to obtain information about certain vascular diseases not related to the heart.
An ECG is usually performed in the following cases:
- Feeling of abnormal heartbeat;
- Attacks of shortness of breath, sudden weakness, fainting;
- Heartache;
- Heart murmurs;
- Deterioration of the condition of patients with cardiovascular diseases;
- Passing medical examinations;
- Medical examination of people over 45 years of age;
- Examination before surgery.
An electrocardiogram is also recommended for:
- Pregnancy;
- Endocrine pathologies;
- Nervous diseases;
- Changes in blood counts, especially with an increase in cholesterol;
- Over 40 years of age (once a year).
Normal readings
One of the most common and first methods for identifying any abnormalities in the normal functioning of the cardiovascular system is an electrocardiogram (ECG). RV myocardial hypertrophy can be indicated by a number of indicators that are significantly deviated from the norm. To diagnose a disease, you need to know which indicators are considered normal and which are not.
When assessing the condition of the right ventricular chamber, all 12 taken leads are studied, paying special attention to the right thoracic leads (V1-V2). Physiological indicators:
- The location of the cardiac axis is at an angle of 40-70 degrees;
- The PQ interval takes from 0.12 to 0.20 s;
- The Q wave is absent in V3-V6;
- The R wave is smooth, straight and symmetrical;
- The T wave is negative in lead aVR;
- ST segment on isoline.
With normal functioning of the heart on the cardiogram, depolarization of the left and right ventricles should occur simultaneously.
The mass of the left ventricle differs from the mass of the right in the direction of increase, as evidenced by the electrical potentials, which are slightly greater in the left ventricle than in the right ventricle. The appearance of rS-type complexes in the right precordial leads is the result of the difference between the electrical potentials of the LV and RV.
When depolarization occurs to the right, qR-type complexes appear, as indicated by the R wave; if, on the contrary, this will be indicated by the P wave in the rS complexes.
There are some cardiographic abnormalities that reflect the structural features of the right ventricle in healthy people. Such deviations are observed in 15-25% of cases and are caused by the special structure of nerve fibers. In the absence of complaints and normal physical development, they do not cause concern and can be observed in:
- Athletes (physiological hypertrophy);
- Children (due to the non-simultaneous development of nerve and muscle fibers);
- Asthenikov (close proximity of the heart to the chest).
Deviations that are a variant of the norm:
- Delay of impulses in the right ventricle;
- Incomplete blockade of the right Purkinje fibers;
- Anterior displacement of the cardiac axis;
- Positive T combined with high R in V1;
- Reducing the voltage of contractions in the first lead to 28 mV.
From simple to complex
Structure of the heart
Before we begin to explain why such a phenomenon as the predominance of the potentials of the left ventricle (LV) or right ventricle (RV) is observed, let us dwell on a simple one. But what does this incomprehensible and frighteningly scientific conclusion of a functionalist doctor mean? This conclusion is a purely electrocardiographic recording. Similar conclusions can be drawn during the interpretation of the cardiogram. The entire muscle mass of both the left and right ventricles is individually represented by small cells - cardiomyocytes.
The peculiarity of these cardiomyocytes is that they are able to accept negative and positive charges. The electric charge, like a chain reaction, spreads from one fiber to another, exciting the entire mass of the ventricular myocardium. The greater the mass of the ventricle, the greater the total potential it will have. In an adult, due to the fact that the LV has to work with greater force, its myocardium is much thicker than that of the RV. And since the ECG records the total potential, the potential of the left ventricle should normally prevail.
Where can I get a cardiogram?
If you suspect that there is something wrong with your heart, you can contact a therapist or cardiologist so that he can give you a referral for an ECG. Also, for a fee, a cardiogram can be done in any clinic or hospital.
Let's look at some terms that an ECG transcript may contain. They do not always indicate serious pathologies, but in any case they require a visit to a doctor for advice, and sometimes additional examinations.
Signs of pancreatic hypertrophy on the ECG
Predominance of left ventricular potentials
The predominance of ventricular potentials or the predominance of its electrical activity is detected by the electrocardiographic method. ECG signs of the predominance of LV activity are changes in the leads responsible for the left parts of the heart. Since the R wave on the cardiogram is responsible for the excitation of the ventricles, the dominance of RV or LV activity will influence changes in this wave in the corresponding leads. If LV activity predominates in the left precordial leads (I, II, AVL, V5-V6), the R wave will be larger than normal - more than 25 mm.
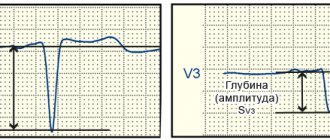
In the right leads, changes in the negative S wave will be observed. It will be more than 15 mm in depth in III, AVF, V1-V2. If the activity of the pancreas predominates, the opposite picture will occur. In the right leads, the height of the R wave will be greater than 7 mm. In the left chest leads, the negative S wave will be deeper than 7 mm. However, you should not draw conclusions only based on the R and S waves. It is necessary to evaluate other elements of the electrocardiogram, combining everything with clinical data.
Any deviations from the norm are considered a sign of pathology, which will be immediately noticed by an experienced specialist. But every person who has ever had an ECG examined with interest a long piece of paper folded several times with mysterious symbols and designations, trying to understand at least something.
The first sign of hypertrophy of the right ventricle of the heart when decoding data on the ECG is the predominance of its potentials over the left, which is why R waves appear in the right precordial leads, and depolarization occurs to the right.
Pathology may be indicated by a shift of the QRS complex vector to the right side, which in turn leads to the appearance of R-waves. Another indicator of the disease is the replacement of the rS complex in lead V1 with an R wave.
If normally the left ventricle gives more impulses, then if the right one is defective, it is the RV impulses that will prevail, shifting the vector to the right.
Cardiologists distinguish three degrees of development of the defect:
- Light (minor deviations from normal values);
- Average (signs of hypertrophy are already significant, but the indicators of the right pancreas are still slightly less than those of the left one);
- Severe (right ventricular impulses have already exceeded those of the LV and prevail in the ECG results).
On the cardiogram you can see special symbols that characterize one or another state of the heart. For example, a high positive R wave and a deep negative P wave are responsible for the frequency of contractions of the left and right atria, and the symbols Q, S, R characterize the contractions of the ventricles. The letter T indicates relaxation of the ventricles.
Signals of disease development based on cardiogram results can be:
- Quite high indicators of the RV1, V2 teeth in the absence of deviations in the V2, TV1 teeth in the STV1, V2 segments;
- Quite high fluctuations of RV1, V2 with a noticeable decrease in the pulsation of the STV1, V2 segment with a negative amplitude of the TV1, V2 tooth;
- The presence in the remaining leads of an increased R wave and a decreased ST segment.
According to the results of the cardiogram, the defect of the right ventricle is not as pronounced as the left, which is a good reason for a more thorough study and clarification of the diagnosis.
Cardiographic varieties identified on the basis of distinctive ECG changes are called hypertrophy types. They differ in the localization of pathological signs.
The detection rate is approximately 23% of patients. This type is caused by a downward displacement of the heart with the apex turning backwards. Such hypertrophy of the right ventricle develops with increased airiness of the lungs at the stage of cor pulmonale.
Signs:
- Low ventricular wave voltage in V leads;
- Deep S wave and positive T wave in V1-V6;
- Shift of the transition zone (V3-V4) towards V5.
Blockade (rSR')
It is detected in 18% of patients and is characteristic of heart block. Caused by non-simultaneous conduction of ventricular excitation, when the left chamber contracts first, then the right.
This type of right ventricular hypertrophy is characterized by:
- The appearance of the Q wave in V1-V2;
- Deep S in V1 combined with deep R in V6;
- The cardiac axis shifts first to the left, and at the end of the contraction - to the right.
The most common type (45% of cases), characteristic of high pulmonary hypertension, when the right ventricle becomes the largest chamber of the heart.
Signs:
- Widening of the QRS complex more than 12 ms;
- R wave voltage is more than 8 mm;
- Deep S wave, the amplitude of which gradually increases from V1 to V6.
- Dropping ST below the isoline;
- In standard and right leads, the T wave is negative.
Develops in 10-13% of patients with moderate overload of the right half of the heart, when the right ventricle becomes equal in size to the left.
Signs:
- Shift of the cardiac axis to the right up to 100 degrees;
- ST below isoline;
- Negative T in the right and standard leads;
- The ventricular complex looks like rSR';
- Voltage R' is more than 7 mm.
Dilation is a stretching of the chamber cavity, accompanied by thinning of its walls.
Both pathologies are externally represented by an enlarged ventricle, however, in the first case, the myocardium is thickened (the chamber may not be changed), in the second, the myocardium is stretched (the chamber is always enlarged).
The simultaneous development of right ventricular hypertrophy and dilatation is observed with:
- Pulmonary hypertension;
- Partition defects;
- Tricuspid defects;
- Pulmonary stenosis;
- Obstructive pulmonary diseases;
- Cardiomyopathies.
Electrocardiographic signs of RVH and dilatation together:
- Displacement of the cardiac axis to the right by 30 degrees or more;
- Deep Q and negative T in lead V3;
- Lengthening ST in V1-V6;
- Blockade of right Purkinje fibers.
The predominance and amplification of potentials is the dominance of electrical impulses from the right ventricle relative to the left. This cardiographic sign reflects the characteristics of electrical conduction to the surface of the chest. An increase in right ventricular electrical potentials is physiological for young children (up to 8-10 years), and is also detected in the following conditions:
- Vertical position of the heart;
- Emotional arousal at the time of examination;
- Incomplete blockade of the right Purkinje fibers.
In the absence of complaints, this sign should not be alarming. However, it can serve as a symptom of incipient hypertrophy when detected:
- Shortness of breath and cough for no apparent reason;
- Cyanosis;
- Delayed physical development;
- Tendency to pulmonary diseases.
The dominance of right-sided potentials is observed when:
- Atresia and stenosis of the pulmonary trunk;
- Tricuspid valve defects;
- Pulmonary hypertension;
- Cystic fibrosis and bronchial asthma.
When the predominance of potentials is normal
ECG of a newborn
The ECG of a full-term child up to one year old shows signs of predominant activity of the pancreas, since at the moment of the child’s birth the pulmonary circulation begins to function. But anatomically, the LV myocardium has not yet had time to “increase” its mass, so the thickness of the RV and LV are approximately the same at the time of birth. After one year and up to 6-8 years of age, as a rule, a restructuring of the cardiovascular system occurs. Due to the fact that the load on the ventricles changes, not only the anatomical location of the heart in the chest changes, but also its electrical axis.
After the age of six, RV dominance begins to wane and the ECG pattern begins to reflect increased LV activity. Therefore, if an ECG reveals dominance of RV potentials in a six-year-old child, this is not a reason to panic. Another question is if the child has some complaints and deviations in physical development. In an adult, a normal ECG should reflect a predominance of left ventricular potentials. The patient's body type may also have an impact. In people with an asthenic (thin) build, the heart occupies a vertical position in the chest, since the dome of the diaphragm is low.
This position leads to a change in the electrical axis of the heart. The largest R wave will be in lead I, and the smallest in lead III. In persons with a hypersthenic physique, the heart occupies a horizontal position due to the high position of the dome of the diaphragm. Therefore, the maximum R wave will be in III, and the smallest in I. In such situations, you should not look for pathology. Another situation where left ventricular activity dominates is physiological hypertrophy. Physiological hypertrophy can occur in athletes, as well as people whose work involves heavy physical activity.
Methodology of the procedure
ECG recording is usually performed in a supine position. To take a cardiogram, a stationary or portable device is used - an electrocardiograph. Stationary devices are installed in medical institutions, and portable ones are used by emergency teams. The device receives information about electrical potentials on the surface of the skin. For this purpose, electrodes are used that are attached to the chest area and limbs.
These electrodes are called leads. There are usually 6 leads installed on the chest and limbs. The chest leads are designated V1-V6, the leads on the limbs are called basic (I, II, III) and reinforced (aVL, aVR, aVF). All leads give a slightly different picture of oscillations, but by summing up the information from all electrodes, you can find out the details of the functioning of the heart as a whole. Sometimes additional leads are used (D, A, I).
Typically, the cardiogram is displayed in the form of a graph on paper containing millimeter markings. Each electrode lead has its own schedule. The standard speed of the belt is 5 cm/s; other speeds may be used. The cardiogram displayed on the tape can also indicate the main parameters, normal indicators and a conclusion generated automatically. Data can also be recorded in memory and on electronic media.
After the procedure, the cardiogram is usually deciphered by an experienced cardiologist.
Clinical symptoms
Symptoms are divided into pulmonary, cardiac and general. In the initial stages, right ventricular hypertrophy often has no manifestations.
General signs:
- Tendency to pneumonia;
- Fast fatiguability;
- Decreased exercise tolerance;
- Relief in a sitting position;
- Displacement of the liver from under the edge of the costal arch;
- Aching pain in the right hypochondrium.
Pulmonary signs:
- Shortness of breath of a mixed nature;
- Cough (dry or streaked with blood).
Cardiac signs:
- Feeling of palpitations, interruptions in heart function;
- Swelling of superficial veins;
- Blue skin;
- Swelling of the legs, increasing in the evening;
- Pressing pain behind the sternum;
- The “head of a jellyfish” symptom is an enlargement of the abdominal veins.
Symptoms and treatment of isolated systolic hypertension
As long as the right ventricle can cope with overload, myocardial hypertrophy does not manifest clinical signs. When the reserves of strength are exhausted, the muscle fibers weaken and their contractions are not enough to pump blood to the lungs. Right ventricular failure appears and increases with the following symptoms:
- difficulty breathing, first during exercise, and then at rest;
- attacks of suffocation;
- chest pain;
- rhythm disturbance;
- strong heartbeat;
- swelling in the legs;
- swelling of the neck veins;
- heaviness in the right hypochondrium due to an enlarged liver;
- congestion of blood in the lungs with cough and bloody sputum;
- accumulation of fluid in the pleural and abdominal cavity.
Diagnosis and probable causes
Considering the fact that based on ECG results alone, it may not be enough to make an accurate diagnosis, the cardiologist prescribes additional types of examination of the patient. These include:
- Electrocardiography (to detect rhythm disturbances);
- Medical examination (listening to heart murmurs, heartbeat rhythm);
- Echocardiography (determining the size of the ventricle using ultrasound, measuring thickness, detecting defects and their sizes);
- Research using a cardiovisor (dynamic observation of cardiac function);
- Identification of whether the patient belongs to one of the risk groups (overweight people, professional athletes, people with bad habits);
- Identification of genetic predisposition.
Why is hypertrophy of the walls of the right ventricle of the heart dangerous? Because this is only an indicator of the presence of a serious disease of the cardiovascular or pulmonary system. The consequences are determined precisely by what caused the hypertrophy.
Possible enlargement of the right ventricle is an indication for a thorough examination:
- Taking anamnesis;
- Examination of the cardiac region and the entire body;
- Palpation, percussion and auscultation of the lungs and heart;
- Studying the condition of the veins and liver;
- Conducting laboratory examinations (general and biochemical tests, determination of ASL-O), radiography and echocardiography.
Causes:
- Pulmonary hypertension in the initial stages;
- Bronchial asthma;
- First stage of emphysema;
- Congenital and acquired defects accompanied by pulmonary hypertension.
The main methods for confirming or excluding a possible disease are radiography and echocardiography.
Obvious hypertrophy indicates cardiopulmonary pathology, in 100% of cases it is combined with severe symptoms and requires:
- Immediate clarification of the diagnosis using radiography and ultrasound of the heart;
- Determination of the degree of pulmonary hypertension;
- Selection of method and means of therapy.
Causes:
- Mitral and tricuspid defects;
- Partition defects;
- Pulmonary trunk defects;
- Fallot's disease;
- Open aortic duct;
- Chronic obstructive pulmonary diseases.
Most often, pancreatic hypertrophy manifests itself in old age, very rarely in young people. But the exception is infants and newborns who are born with a heart defect.
Left ventricular hypertrophy of the heart: treatment, causes, symptoms
Have you been struggling with HYPERTENSION for many years without success?
Head of the Institute: “You will be amazed at how easy it is to cure hypertension by taking it every day.
Left ventricular hypertrophy is a syndrome characteristic of most diseases of the cardiovascular system, which consists of an increase in the muscle mass of the heart.
Unfortunately, today there are more and more cases of left ventricular hypertrophy in young people. The danger of this is complemented by a higher percentage of deaths than in older people. Men with left ventricular myocardial hypertrophy die 7 times more often than the fairer sex.
Our readers successfully use ReCardio to treat hypertension. Seeing how popular this product is, we decided to bring it to your attention. Read more here...
In a normal physiological state, the heart, pushing blood into the aorta, performs the function of a pump. From the aorta, blood flows to all organs. When the left ventricle relaxes, it receives a portion of blood from the left atrium. Its quantity is constant and sufficient to ensure optimal levels of gas exchange and other metabolic functions throughout the body.
As a consequence of the formation of pathological changes in the cardiovascular system, it becomes more difficult for the heart muscle to perform this function. To perform the same amount of work requires more energy expenditure. Then a natural compensatory mechanism is activated - an increase in load leads to an increase in the muscle mass of the heart. This can be compared to how increasing the load on the muscles in the gym results in an increase in muscle mass and volume.
The capillary network does not have time to develop after LV hypertrophy, so rapidly hypertrophied tissue may suffer from oxygen starvation. Which leads to ischemic changes in the myocardium. In addition, the conduction system of the heart remains the same, which leads to disruption of impulse conduction and various arrhythmias.
The tissue of the left ventricle, in particular the interventricular septum, is most susceptible to hypertrophy.
During intense physical activity, the heart has to pump more blood and work harder. Therefore, professional athletes may develop moderate left ventricular hypertrophy, which is physiological or compensatory.
In almost all long-term heart diseases, left ventricular hypertrophy is an obligatory consequence.
Left ventricular myocardial hypertrophy is observed with:
- hypertension;
- aortic valve stenosis;
- hypertrophic cardiomyopathy;
- intense long-term physical activity;
- obesity;
- smoking, drinking alcohol.
Thus, for any heart disease, left ventricular hypertrophy is a mandatory syndrome.
Excess weight is a risk factor for hypertension, which causes left ventricular hypertrophy. In addition, with obesity, blood supply to an enlarged body requires a lot of work to ensure blood supply to all tissues, which also leads to changes in the myocardium.
Of the congenital diseases, the main place is in heart defects with impaired blood outflow from the ventricle.
However, left ventricular hypertrophy will show the same symptoms for any etiology.
According to the degree of change in the shape of the left ventricle of the heart and its thickness, eccentric and concentric hypertrophy of the left ventricular myocardium is distinguished.
Concentric hypertrophy of the left ventricle is characterized by thickening of its walls. Its cavity in this case does not change. It is formed when the ventricle is overloaded with blood pressure. This form is typical for hypertension. This etiology accounts for at least 90% and has a high risk of life-threatening cardiovascular complications - more than 35%.
Eccentric left ventricular hypertrophy is characterized by relative preservation of the thickness of the walls of the ventricle, an increase in its mass and the size of the cavity. The risk of severe complications is about 25%. This type develops when there is excess blood volume.
For a long time, left ventricular hypertrophy of the heart has minor symptoms or the heart does not let you know that it is working through force. When compensatory capabilities are exhausted and a person begins to complain, the changes in the myocardium are already significant.
The following signs of left ventricular hypertrophy appear in varying degrees of severity:
- dyspnea;
- tachycardia;
- cardiac pain;
- feeling of weakness and fainting;
- fast fatiguability.
Timely early detection reduces the risk of developing severe complications. ECG signs of left ventricular hypertrophy are easily determined by any therapist. This method is cheap and informative.
Left ventricular hypertrophy on the ECG is manifested by an increase in the pulse transit time, ischemic changes on the ECG, impaired impulse conduction, deviation of the axis to the hypertrophied area, a shift in the electrical position of the heart, and the location of the transition zone.
If there is difficulty breathing, there is a desire to stop and catch your breath with the usual load, if there is pressure in the chest, or causeless weakness occurs, then you should consult a doctor.
The cardiologist will prescribe a complete clinical, biochemical and instrumental examination. Upon examination, specific heart murmurs and an increase in its boundaries may be detected. An X-ray examination will show how enlarged the heart is and in what parts. An echocardiogram will help determine the location of disorders and the degree of decrease in heart activity.
Once a diagnosis of left ventricular myocardial hypertrophy has been established, treatment depends on the degree of its severity and the severity of the patient’s general condition.
Changes in heart size are a consequence of other diseases. When treating a patient diagnosed with left ventricular hypertrophy, the causes that led to it are of primary importance.
Depending on the severity of the patient’s condition and how severe the left ventricular hypertrophy is, treatment can be carried out in a hospital or at home.
A prerequisite for successful treatment is a correct lifestyle. If this recommendation is ignored, any therapy is useless.
The diet reduces salt intake. Products that strengthen the heart muscle are recommended.
Constant monitoring of ECG and blood pressure levels and regular examination by a cardiologist are required.
If your condition is satisfactory, regular walks in the fresh air are good. Also, moderate left ventricular hypertrophy does not exclude race walking and swimming at a gentle pace. Excessive physical activity is avoided.
Medicines are taken throughout life. These are calcium channel blockers, beta blockers, antihypertensive drugs, metabolic cardiac medications.
In some cases, surgery may be recommended. During the operation, areas of thickened muscle are excised.
Complications are more than dangerous. This includes circulatory failure, rhythm disturbances, ischemic changes, and myocardial infarction.
Cardiovascular failure is the inability of the heart to perform its pumping function and provide the body with blood.
Rhythm disturbances occur as a result of the fact that the conduction system of the heart does not have the ability to hypertrophy. The time and quality of impulse conduction changes. Areas may appear where impulses do not pass through.
Ischemic manifestations (lack of oxygen in the tissue) occur due to the relatively slow development of the capillary network in the hypertrophied heart tissue. As a result, she does not receive enough oxygen. On the other hand, when working with increased load, the myocardial need for oxygen increases significantly.
For hypertrophy of the left ventricle of the heart, treatment continues for a long time. It has been proven that early treatment and the patient’s responsible attitude towards it can significantly improve the quality and length of life of patients.
Predominance of left ventricular potentials. Such a recording on the back of the electrocardiogram can not only confuse the patient, but also intimidate it. After all, just a day ago the person felt absolutely healthy and did not complain about anything.
Other types of procedures
There are several other methods for carrying out the procedure. For example, this is monitoring with physical activity. Abnormalities are usually more pronounced on the stress ECG. The most common way to provide the body with the necessary physical activity is a treadmill. This method is useful in cases where pathologies can only manifest themselves in the case of increased heart function, for example, if coronary artery disease is suspected.
During phonocardiography, not only the electrical potentials of the heart are recorded, but also the sounds that arise in the heart. The procedure is prescribed when it is necessary to clarify the occurrence of a heart murmur. This method is often used when heart defects are suspected.
Cases in newborns and children
Predominance of right ventricular potentials is often observed in newborns and young children. If such a sign is detected, the child is examined for additional symptoms and complaints. Their identification serves as an indication for in-depth research.
In most cases, the predominance of potentials is a variant of the norm and is not a cause for concern. Such a child is not registered.
Right ventricular hypertrophy in newborns and children is a symptom of heart defects, cystic fibrosis, bronchial asthma and prolonged pneumonia. Unlike the predominance of potentials, which can be congenital, hypertrophy develops gradually.
Its detection indicates a pre-existing disease, which requires confirmation by X-ray and ultrasound examinations. Children with this pathology are registered with a cardiologist.
Right ventricular hypertrophy in a child
Enlargement of the right ventricle of the heart is observed more in childhood. In infants, immediately after birth, the load on the right side of the heart is greater than on the left. Doctors call this reason for the change in the organ physiological. However, congenital right ventricular hypertrophy is much more common in children. Some symptoms of the disease do not appear immediately. Constant monitoring of the child's condition and a complete examination after birth help to make the correct diagnosis and choose accurate treatment methods.
Treatment tactics
Types of treatment:
- Conservative;
- Surgical;
- Palliative.
Since the pathology is secondary, the choice of how to treat right ventricular hypertrophy of the heart depends on the underlying disease. Timely therapy allows you to stop the progression of hypertrophy in time and improve the quality of life of patients.
For pulmonary diseases the following is performed:
- Inhalation of bronchodilators (adrenomimetics, anticholinergics, aminophylline);
- Taking mucolytics, cough suppressants;
- Antihistamines are used according to indications.
For heart diseases:
- Correction of blood pressure;
- Taking antiarrhythmic and diuretic drugs;
- Treatment with cardiac drugs (ACE inhibitors, nitroglycerin, calcium channel inhibitors).
Surgical treatment is performed when conservative therapy is ineffective - in the last stages of pulmonary diseases and in case of decompensation of defects. Valve replacement, balloon valvuloplasty, commissurotomy, lung transplantation are possible: it all depends on the disease-cause.
Palliative therapy is aimed at maintaining the life of patients with end-stage hypertrophy, when the underlying disease cannot be cured. It includes the use of diuretics, cardiotonics, oxygen inhalation and proper patient care.
The patient is required to categorically abstain from drinking alcohol and energy drinks, as well as from smoking. In addition to the main complex of therapy, physical therapy or swimming lessons can be added.
This pathology indicates more serious abnormalities in the functioning of the cardiopulmonary system, and if it is ignored and not treated, the consequences can be very sad.
If the disease is congenital, then timely therapy or surgery can stop the development of defects and stabilize the functioning of the heart.
In order to prevent the disease, it is necessary to lead a correct and healthy lifestyle, avoid hypothermia, harden the body, and do not ignore acute respiratory viral infections, which can lead to pneumonia and the development of hypertrophy. In other words, you need to be more attentive to your own health and promptly contact a specialist for qualified help.
Prevention of LVH
The main preventive measures include:
- elimination of bad habits (alcohol and nicotine addiction);
- a healthy diet (eliminating foods containing low-density lipoproteins, the so-called bad cholesterol, while increasing the intake of high-density lipoproteins, the “good cholesterol”);
- body weight control (obesity always negatively affects heart function);
- balanced physical activity appropriate for age;
- regular exposure to fresh air (active oxygen stimulates proper cardiac activity).
These recommendations will help not only avoid heart disease, but also improve your overall quality of life.
Source: diametod.ru
Types of teeth
First we should talk a little about how the heart works. It has 4 chambers - two atria and two ventricles (left and right). The electrical impulse, due to which it contracts, is formed, as a rule, in the upper part of the myocardium - in the sinus pacemaker - the sinoatrial (sinus) node.
The impulse spreads down the heart, first affecting the atria and causing them to contract, then passes through the atrioventricular nerve node and another nerve node, the bundle of His, and reaches the ventricles. The main burden of pumping blood is taken on by the ventricles, especially the left one, which is involved in the systemic circulation. This stage is called heart contraction or systole.
After contraction of all parts of the heart, the time comes for their relaxation - diastole. The cycle then repeats again and again - this process is called heartbeat.
The condition of the heart, in which there are no changes in the propagation of impulses, is reflected on the ECG in the form of a straight horizontal line, called an isoline. The deviation of the graph from the isoline is called a spike.
One heartbeat on the ECG contains six waves: P, Q, R, S, T, U. The waves can be directed both up and down. In the first case they are considered positive, in the second - negative. The Q and S waves are always positive, and the R wave is always negative.
What is “depolarization” and “repolarization”
The occurrence of an impulse (electric current or action potential) in heart cells goes through two main periods:
- Depolarization - sodium and calcium ions enter the cell and the charge changes to positive. At a certain speed, the depolarization wave is transmitted to neighboring cells and covers the entire muscle. Actin combines with myosin and the heart contracts. The speed of wave propagation depends on the presence of healthy or altered cells (ischemic or scar tissue) in the path of the impulse.
- Myocardial repolarization is a longer period, it is necessary to restore the negative intracellular charge, the flow of potassium ions must leave the cells. This phase determines the accumulation of energy in the heart muscle and preparation for the next contraction. Visible rest actually includes all the biochemical mechanisms of energy production, enzymes and oxygen from the blood are consumed. Until complete recovery is completed, the heart is not able to contract.
The most important mechanism ensuring sufficient action potential is the sodium-potassium pump.
Violation of myocardial repolarization can be detected during an electrocardiographic examination by determining the repolarization time.
Rhythm of contractions
Violation of the rhythm of contractions is called arrhythmia. The irregularity of the rhythm during arrhythmia is measured as a percentage. An irregular rhythm is indicated by a deviation in the distance between similar teeth by more than 10%. Sinus arrhythmia, that is, arrhythmia combined with sinus rhythm, may be normal for adolescents and young adults, but in most cases it indicates the onset of a pathological process.
A type of arrhythmia is extrasystole. They say it in the case when extraordinary contractions are observed. Single extrasystoles (no more than 200 per day with Holter monitoring) can also be observed in healthy people. Frequent extrasystoles that appear on the cardiogram in the amount of several pieces may indicate ischemia, myocarditis, or heart defects.
How to treat hypertrophy
To reduce the degree of hypertrophy of the heart muscle, identification and treatment of the underlying disease that led to this disorder is required. If heart defects are detected, reconstructive operations on the valves and their replacement with artificial ones are recommended.
If the cause of pathological changes in the myocardium is obstructive pulmonary diseases, then therapy is carried out with the following groups of drugs:
- bronchodilators (Salbutamol, Serevent);
- mucolytics (Lazolvan, Acetylcysteine);
- corticosteroids (Prednisolone, Dexamethasone, Beklofort).
In case of heart failure, the lack of oxygen and potassium is first corrected, and then cardiac glycosides are prescribed. To remove excess fluid, it is better to use potassium-sparing diuretics. Drugs from the group of prostaglandins (Alprostan, Vazaprostan) and endothelin receptor antagonists (Bozenex, Tracleer) have a powerful vasodilating and protective effect on myocardial cells.
To strengthen the heart muscle, patients are shown products containing potassium and magnesium salts (Panangin, Magnicum, Kalipoz), metabolic stimulants (Mexidol, Mildronate), oxygen therapy and hyperbaric oxygenation.
Heart Rate Types
This option is the simplest and most understandable. It determines the number of contractions in one minute. The number of contractions may be higher than normal (tachycardia) or lower than normal (bradycardia). The normal heart rate in adults can range from 60 to 80 beats. However, the norm in this case is a relative concept, so bradycardia and tachycardia may not always be evidence of pathology.
Heart rate norms for children of different ages
| Age | Heart rate, beats/min |
| Newborns | 140-160 |
| 6 months | 130-135 |
| 1 year | 120-125 |
| 2 years | 110-115 |
| 3 years | 105-110 |
| 5 years | 100-105 |
| 8 years | 90-100 |
| 10 years | 80-85 |
| 12 years and older | 70-75 |
There are several types of heart rhythm, depending on where the nerve impulse begins to spread, causing the heart to contract:
- Sinus,
- Atrial,
- Atrioventricular,
- Ventricular.
Normally, the rhythm is always sinus. In this case, sinus rhythm can be combined with both a heart rate above normal and a heart rate below normal. All other types of rhythms are evidence of problems with the heart muscle.
Atrial rhythm
Atrial rhythm also often appears on the cardiogram. Is atrial rhythm normal or is it a type of pathology? In most cases, the atrial rhythm on the ECG is not normal. However, this is a relatively mild degree of heart rhythm disturbance. It occurs when the sinus node is suppressed or disrupted.
Rhythm emanating from the atrioventricular node. With atrioventricular rhythm, the pulse rate usually drops to less than 60 beats per minute. Causes: weakness of the sinus node, atrioventricular block, taking certain medications. Atrioventricular rhythm, combined with tachycardia, can occur during heart surgery, rheumatism, and heart attack.
Ventricular rhythm
With ventricular rhythm, contractile impulses propagate from the ventricles. The contraction frequency drops to below 40 beats per minute. The most severe form of rhythm disturbance. Occurs in acute infarction, heart defects, cardiosclerosis, cardiac circulatory failure, and in a preagonal state.
Dangerous consequences
The left ventricle is responsible for oxygen saturation and movement of arterial blood into the aorta and further through all small vessels to nourish the organs. As the volume increases, the blood presses on the walls, the connective tissue displaces the muscle tissue, and the ventricle ceases to cope with its functional duties.
What such changes threaten is determined by the following diagnoses:
- coronary heart disease - a violation of the blood supply to the heart due to thickening of the walls of the gastric chamber;
- myocardial infarction – death (necrosis) of part of the heart muscle;
- ventricular extrasystole (arrhythmia) – failure of the heart rhythm;
- atrioventricular or ventricular block - cessation of the passage of electrical impulses between the atria and ventricles, leading to hemodynamics;
- heart failure is a low contractility of the heart muscle, often leading to death.
Timely detection of LVH will help prevent serious complications. The most informative in terms of diagnosing pathology is the electrocardiographic examination method.