Situations with GPP
Venous blood from the venae cava enters the right atrium. Overload of the right atrium occurs when blood enters from the vena cava in excess or with pulmonary hypertension, when blood from the right atrium to the right ventricle cannot pass immediately and completely. As a result, the atrium cavity begins to gradually expand and the wall thickens.
Another reason for overload of the right atrium is hypertension in the pulmonary circulation, which leads to hypertension in the right ventricle. For this reason, blood from the PP cannot immediately pass into the ventricle, which also leads to GPP. The load on the right side of the heart also increases with chronic lung diseases. The main reason is excess blood and pressure.
This condition occurs when there is stenosis of the tricuspid valve, which separates the atrium from the ventricle. In this case, some of the blood gets stuck in the atrium. Most often, this defect occurs after a rheumatic attack, with bacterial endocarditis.
Another defect is the insufficiency of the specified valve, in which its valves do not close completely and some of the blood returns. This condition occurs when the left ventricle dilates. Pressure load will occur with pulmonary pathologies: bronchitis, emphysema, asthma, genetic disease of the pulmonary artery. These diseases increase the volume of blood in the ventricle, and after this the atrium becomes overstrained. This is why overload of the right atrium and right ventricle are so often combined.
To restore normal blood flow, the atrium has to push blood out with greater force, and it hypertrophies. Overload of the right atrium develops gradually when the causative disease remains undiagnosed and untreated.
The time is individual for each patient, but the result is always depletion of the compensatory capabilities of the heart muscle and the onset of decompensated heart failure in a chronic course.
Changes in the atria
An ECG can diagnose most heart pathologies. The reasons for their appearance are due to concomitant diseases and lifestyle characteristics of the patient.
What does this mean if changes in the myocardium are detected on the ECG? In most cases, the patient requires conservative treatment and lifestyle modification.
Right atrium: description, normal performance, diagnosis and treatment of diseases
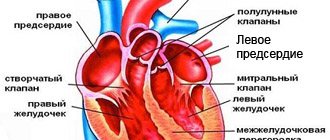
The human heart is represented by four chambers: atria and ventricles (right and left). The side walls of the cavities form the characteristic outlines of the organ on x-ray photographs.
The right atrium (RA) is the smallest chamber located at the base (top) of the heart. The RA cavity is connected to the right ventricle through the atrioventricular junction and the tricuspid valve.
The coronary groove serves as the boundary between the departments on the outer surface, which is poorly visualized due to the massiveness of the pericardium (the pericardial sac).
The atrium cavity is not designed for a large one-time volume of blood, so the thickness of the walls is 2-3 mm (five times less than that of the ventricle). A sufficient number of muscle fibers and the functionality of the valves avoid overload.
The anatomical structure of the right atrium is represented by a hexagonal cubic chamber. Characteristics of the main landmarks and elements of each of the walls are in the table:
- The openings of the upper and lower PV are at the boundaries with the front and rear walls.
- The Lover's mound is located between the points of confluence of blood vessels. In the prenatal period, the formation serves as a valve that regulates the direction of flow.
- Under the opening of the lower PV is the Eustachian valve (tissue protrusion), which extends to the edge of the fossa oval in the form of a Chiari network (plates with fenestrae - “holes”)
Vessels of the right atrium
Cardiomyocytes of the RA are supplied with blood by the right coronary artery, which starts from the aortic sinus and lies in the designated coronal sulcus. Along the way, the vessel gives off branches:
- to the sinoatrial node (the main pacemaker of the heart);
- atrial (2-6), which supply the ear and nearby tissues;
- intermediate branch (nourishes the bulk of the myocardium).
The outflow of venous blood from the myocardium of the right atrium occurs in two ways:
- Through the coronary veins, the fluid enters the coronary sinus of the left part of the diaphragmatic surface of the heart. The length of the sinus is 2-3 cm and opens into the cavity of the RA at the confluence of the inferior vena cava.
- Direct outflow from small-caliber vessels (the group of “right atrial veins” of Viessen-Tibizia) into the chamber cavity.
Source: https://med-perevozka.ru/simptomy/izmeneniya-v-predserdiyah.html
Other diseases leading to GPP
The development of right atrium overload can be provoked by:
- Myocardial remodeling - this phenomenon is considered part of post-infarction cardiosclerosis, when a scar develops at the site of necrosis. Healthy cardiomyocytes become more voluminous - they thicken, which outwardly looks like hypertrophied muscle. This is also a compensatory mechanism and most often involves the left ventricle. This creates another combination of right atrial overload and left ventricular diastolic overload.
- Postmyocardial cardiosclerosis - scar tissue is formed by the same mechanisms, but after inflammatory processes in the myocardium.
- Coronary heart disease - here we are talking about blockage of the coronary artery with a thrombus or plaque of atherosclerosis. This necessarily causes myocardial ischemia, and the contractile function of cardiomyocytes is impaired. Then the areas of the myocardium adjacent to the affected areas begin to thicken compensatoryly.
- Hypertrophic cardiomyopathy - occurs due to gene disorders in which uniform thickening of the myocardium of the entire heart muscle occurs. It is more often typical for children and involves the myocardium of the right atrium, then overload of the right atrium in the child is recorded.
Of the congenital pathological conditions of the heart muscle, heart overload is caused by:
- Defective septum between the atria. With such a deviation, the heart supplies blood to the right and left half of the heart under the same pressure, as a result of which the atrium receives an increased load.
- Ebstein's anomaly is a rare defect in which the atrioventricular valve leaflets are adjacent to the right ventricle rather than to the atriogastric ring. Then the right atrium merges with part of the right ventricle and also hypertrophies.
- Transposition of the great vessels - the main arteries of the cardiovascular system change their anatomical position - the main artery of the lungs is separated from the left parts of the heart, and the aorta is separated from the right. In these cases, GPP occurs in a child under 1 year of age. This is a very serious deviation.
- It is also possible to overload the right atrium in adolescents prone to fanatical sports. Regular physical activity is a common cause of HPP.
Right atrium overload: signs, causes, treatment methods, reviews
According to WHO statistics, more than 5 million people die every year from heart pathologies. Right atrium overload (RAO) or its hypertrophy is rare among cardiac pathologies, but its significance is great because it entails changes in other body systems.
A little physiology
The human heart includes 4 chambers, each of which, for certain reasons, can enlarge and hypertrophy. Typically, hypertrophy is an attempt by the body to overcome any organ failure with this compensation. Hypertrophy of the heart does not become an independent disease - it is a symptom of other pathologies.
The main function of the heart is to create blood flow to supply all tissues and organs with nutrients and oxygen.
Situations with GPP
Venous blood from the venae cava enters the right atrium. Overload of the right atrium occurs when blood enters from the vena cava in excess or with pulmonary hypertension, when blood from the right atrium to the right ventricle cannot pass immediately and completely. As a result, the atrium cavity begins to gradually expand and the wall thickens.
Another reason for overload of the right atrium is hypertension in the pulmonary circulation, which leads to hypertension in the right ventricle. For this reason, blood from the PP cannot immediately pass into the ventricle, which also leads to GPP. The load on the right side of the heart also increases with chronic lung diseases. The main reason is excess blood and pressure.
This condition occurs when there is stenosis of the tricuspid valve, which separates the atrium from the ventricle. In this case, some of the blood gets stuck in the atrium. Most often, this defect occurs after a rheumatic attack, with bacterial endocarditis.
Another defect is the insufficiency of the specified valve, in which its valves do not close completely and some of the blood returns. This condition occurs when the left ventricle dilates.
Pressure load will occur with pulmonary pathologies: bronchitis, emphysema, asthma, genetic disease of the pulmonary artery. These diseases increase the volume of blood in the ventricle, and after this the atrium becomes overstrained.
This is why overload of the right atrium and right ventricle are so often combined.
To restore normal blood flow, the atrium has to push blood out with greater force, and it hypertrophies. Overload of the right atrium develops gradually when the causative disease remains undiagnosed and untreated.
The time is individual for each patient, but the result is always depletion of the compensatory capabilities of the heart muscle and the onset of decompensated heart failure in a chronic course.
Other diseases leading to GPP
The development of right atrium overload can be provoked by:
- Myocardial remodeling - this phenomenon is considered part of post-infarction cardiosclerosis, when a scar develops at the site of necrosis. Healthy cardiomyocytes become more voluminous - they thicken, which outwardly looks like hypertrophied muscle. This is also a compensatory mechanism and most often involves the left ventricle. This creates another combination of right atrial overload and left ventricular diastolic overload.
- Postmyocardial cardiosclerosis - scar tissue is formed by the same mechanisms, but after inflammatory processes in the myocardium.
- Coronary heart disease - here we are talking about blockage of the coronary artery with a thrombus or plaque of atherosclerosis. This necessarily causes myocardial ischemia, and the contractile function of cardiomyocytes is impaired. Then the areas of the myocardium adjacent to the affected areas begin to thicken compensatoryly.
- Hypertrophic cardiomyopathy - occurs due to gene disorders in which uniform thickening of the myocardium of the entire heart muscle occurs. It is more often typical for children and involves the myocardium of the right atrium, then overload of the right atrium in the child is recorded.
Of the congenital pathological conditions of the heart muscle, heart overload is caused by:
- Defective septum between the atria. With such a deviation, the heart supplies blood to the right and left half of the heart under the same pressure, as a result of which the atrium receives an increased load.
- Ebstein's anomaly is a rare defect in which the atrioventricular valve leaflets are adjacent to the right ventricle rather than to the atriogastric ring. Then the right atrium merges with part of the right ventricle and also hypertrophies.
- Transposition of the great vessels - the main arteries of the cardiovascular system change their anatomical position - the main artery of the lungs is separated from the left parts of the heart, and the aorta is separated from the right. In these cases, GPP occurs in a child under 1 year of age. This is a very serious deviation.
- It is also possible to overload the right atrium in adolescents prone to fanatical sports. Regular physical activity is a common cause of HPP.
Symptomatic manifestations of pathology
GPP itself has no symptoms. Only symptoms associated with the underlying disease, which are complemented by venous stagnation, may be of concern.
Then we can say that signs of overload of the right atrium are shortness of breath even with minor exertion, pain behind the sternum.
Circulatory failure and cor pulmonale may develop. With cor pulmonale:
- shortness of breath in a horizontal position and with the slightest exertion;
- cough at night, sometimes mixed with blood.
Insufficient blood flow:
- heaviness in the right side of the chest;
- swelling in the legs;
- ascites;
- dilatation of veins
There may also be causeless fatigue, arrhythmias, tingling in the heart, and cyanosis. If these complaints arose only during infections and for the first time, you can count on their disappearance after treatment. For monitoring, a dynamic ECG is performed.
Diagnostics
There are no specific signs of pathology. It is only possible to assume the presence of overloads if a person suffers from chronic lung pathologies or has problems with valves.
In addition to palpation, percussion and auscultation, an ECG is used, which is used to determine some signs of right atrium overload on the ECG. However, even these indicators may be present only temporarily and disappear after the processes are normalized. In other cases, a similar picture may indicate the beginning of the process of atrial hypertrophy.
Ultrasound helps determine the increase in pressure and the volume of blood located in various parts of the heart. This method can detect disorders in all parts of the heart and blood vessels.
Pulmonary heart (P-pulmonale)
With it, pathological changes occur in the pulmonary circulation, and this is the main reason for overload of the right atrium.
On the ECG this is reflected by a modified P wave (atrial wave). It becomes tall and pointed in the form of a peak instead of the smooth apex of normal.
Functional overload of the right atrium on the ECG can also give an altered P - this is noted, for example, with overactivity of the thyroid gland, tachycardia, etc. Deviation of the heart axis to the right does not always occur only with HPP; it can also be normal in high asthenics. Therefore, other studies are used for differentiation.
If signs of right atrium overload are detected on the ECG, the patient is recommended to undergo echocardiography. It is considered safe for any category of patients and can be repeated many times over time. Modern devices can give answers about the thickness of the heart walls, the volume of the chambers, etc.
Together with echocardiography, the doctor may also prescribe Doppler ultrasound, then you can obtain information about hemodynamics and blood flow.
If there is a divergence of opinions, CT or radiography is prescribed. X-ray examination shows abnormalities of the right atrium and ventricle. Their contours merge with the contours of the vessels. In addition, an x-ray will show the condition of other structures of the chest, which is very valuable in case of pulmonary pathology as the root cause of HPP.
Consequences of GPP
In chronic diseases of the pulmonary system, the active alveoli are replaced by fibrous tissue, and the gas exchange area becomes smaller. Microcirculation is also disrupted, which leads to increased pressure in the pulmonary circulation. The atria have to actively contract, which ultimately causes their hypertrophy.
Thus, the complications and consequences of GPP are:
- expansion of the heart chambers;
- circulatory disorders, first in the small and then in the large circle;
- formation of the pulmonary heart;
- venous congestion and heart valve insufficiency.
If left untreated, pulse irregularities and attacks of heart failure may develop, which can lead to death.
Treatment
Normalizing the size of the atrium and improving the functioning of the heart muscle is only possible if the underlying disease – the cause of the pathology – is treated. Such treatment is always complex; monotherapy does not make sense.
In the presence of pulmonary pathology, these are bronchodilators (tablets and inhalers), antibacterial therapy for bacterial etiology of disorders, anti-inflammatory drugs.
For bronchiectasis, surgical treatment is used.
In case of heart defects, the best solution is corrective surgery. After heart attacks and myocarditis, it is necessary to prevent remodeling with the help of antihypoxic and cardioprotective drugs.
Antihypoxants are indicated: “Actovegin”, “Mildronate”, “Mexidol” and “Preductal”. Cardioprotectors: ACEs or angiotensin II receptor antagonists (ARA II). They can actually slow down the onset of chronic heart failure. More often than others, Enalapril, Quadropril, Perindopril, etc. are prescribed.
Nitrones, beta blockers (“Metoprolol”, “Bisoprolol”, “Nebivalol”, etc.), ACE inhibitors, antiplatelet agents that prevent the formation of blood clots, statins that normalize the amount of cholesterol are required.
Also used in treatment are glycosides (according to indications) and antiarrhythmics, agents that improve metabolic processes in the heart muscle. Judging by the reviews, good results were obtained when prescribing Riboxin.
Relapse Prevention
If drug therapy is the prerogative of the doctor, greater responsibility falls on the patient himself. Without his participation, the efforts of doctors will not produce results.
A person must definitely reconsider his lifestyle: give up smoking and alcohol, establish proper nutrition, eliminate physical inactivity, adhere to a daily routine, exercise moderate physical activity, and normalize body weight.
If pathologies of the cardiovascular and pulmonary systems become chronic, they cannot be completely cured.
The condition can only be improved by preventing exacerbations of these pathologies. Then the load on the cardiac system decreases.
GPP and pregnancy
During pregnancy, the body undergoes enormous changes not only in terms of hormonal balance, but also in the functioning of internal organs.
A difficult situation arises when diagnosing right atrium overload during pregnancy, which in this situation is considered an extragenital disease.
The diagnosis must not only be established, but also the woman’s ability to bear a fetus and give birth.
The best option, of course, is to diagnose heart pathologies before conception, but this does not always happen. Most often, pregnant women with heart pathologies are hospitalized three times during gestation; this is done to monitor the condition over time.
When first admitted to the hospital, the defect is examined, the activity of the process is determined and the work of the blood circulation is assessed, taking into account the question of a possible termination of pregnancy.
Repeated hospitalization is necessary because the physiological stress of the body to maintain the functioning of the heart muscle in a woman reaches its peak. The third hospitalization helps doctors choose the method of delivery.
Preventive actions
Prevention of right atrium hypertrophy begins with a review of the lifestyle, which involves proper balanced nutrition and a rational work and rest schedule.
If you are not a professional athlete and you do not necessarily need Olympic medals, do not show stubborn fanaticism in playing sports. This exhausts the body and exhausts the heart. The pressure in the circulatory system increases, and hypertrophy will not take long to occur.
Daily walks of an hour a day, swimming, and cycling are quite enough.
Another problem is eliminating stress. They also have a very negative impact on the functioning of the heart and the entire body as a whole. Yoga, meditation, and relaxation can help solve the problem.
Source: https://FB.ru/article/397136/peregruzka-pravogo-predserdiya-priznaki-prichinyi-metodyi-lecheniya-otzyivyi
Symptomatic manifestations of pathology
GPP itself has no symptoms. Only symptoms associated with the underlying disease, which are complemented by venous stagnation, may be of concern.
Then we can say that signs of overload of the right atrium are shortness of breath even with minor exertion, pain behind the sternum.
Circulatory failure and cor pulmonale may develop. With cor pulmonale:
- shortness of breath in a horizontal position and with the slightest exertion;
- cough at night, sometimes mixed with blood.
Insufficient blood flow:
- heaviness in the right side of the chest;
- swelling in the legs;
- ascites;
- dilatation of veins
There may also be causeless fatigue, arrhythmias, tingling in the heart, and cyanosis. If these complaints arose only during infections and for the first time, you can count on their disappearance after treatment. For monitoring, a dynamic ECG is performed.
Diffuse changes in the myocardium: what is it and what are the possible causes of the condition
Cardiovascular diseases top the list of causes of death in the world. Most deaths are due to coronary heart disease. To promptly recognize and prevent heart problems, various diagnostic methods are used, in particular an electrocardiogram (ECG) and ultrasound (echo-CG).
And for patients who have received an ECHO-CG or ECG result that says “diffuse changes in the myocardium,” the question arises: what is this?
The myocardium is the muscular middle layer of the heart containing contractile cells (cardiomyocytes). The coordinated contraction of cardiomyocytes causes the heart to contract and pump out blood. As a type of muscle tissue, the myocardium is unique among all other muscle tissues in the human body.
Diagnostics
There are no specific signs of pathology. It is only possible to assume the presence of overloads if a person suffers from chronic lung pathologies or has problems with valves.
In addition to palpation, percussion and auscultation, an ECG is used, which is used to determine some signs of right atrium overload on the ECG. However, even these indicators may be present only temporarily and disappear after the processes are normalized. In other cases, a similar picture may indicate the beginning of the process of atrial hypertrophy.
Ultrasound helps determine the increase in pressure and the volume of blood located in various parts of the heart. This method can detect disorders in all parts of the heart and blood vessels.
Pulmonary heart (P-pulmonale)
With it, pathological changes occur in the pulmonary circulation, and this is the main reason for overload of the right atrium.
On the ECG this is reflected by a modified P wave (atrial wave). It becomes tall and pointed in the form of a peak instead of the smooth apex of normal.
Functional overload of the right atrium on the ECG can also give an altered P - this is noted, for example, with overactivity of the thyroid gland, tachycardia, etc. Deviation of the heart axis to the right does not always occur only with HPP; it can also be normal in high asthenics. Therefore, other studies are used for differentiation.
If signs of right atrium overload are detected on the ECG, the patient is recommended to undergo echocardiography. It is considered safe for any category of patients and can be repeated many times over time. Modern devices can give answers about the thickness of the heart walls, the volume of the chambers, etc.
Together with echocardiography, the doctor may also prescribe Doppler ultrasound, then you can obtain information about hemodynamics and blood flow.
If there is a divergence of opinions, CT or radiography is prescribed. X-ray examination shows abnormalities of the right atrium and ventricle. Their contours merge with the contours of the vessels. In addition, an x-ray will show the condition of other structures of the chest, which is very valuable in case of pulmonary pathology as the root cause of HPP.
Signs on the ECG in comparison with the norm
Right atrium dysfunction most often develops against the background of combined myocardial damage (valvular defects, coronary artery disease). Clinical manifestations are nonspecific, so a complex of studies is required to make a diagnosis.
Typical malfunctions of the PP:
- hypertrophy;
- overvoltage;
- presence of a blood clot;
- dilatation;
- arrhythmias (if the sinoatrial node is involved in the process).
Symptoms of increased load
Increased stress on the chambers of the heart develops as resistance or fluid volume increases.
Characteristic deviations due to overload of the right atrium:
- increase in EDV (200-300 ml);
- thickening of the myocardial layer (more than 3-4 mm);
- increased pressure (systolic and diastolic) in the cavity.
If GPP is suspected, the following is examined on the cardiogram:
- the height and shape of the R, S waves in leads I-III and the P wave in any of leads II, III or aVF;
- direction (up/down) and width of the base of the teeth;
- repetition of a pattern (haphazardly or periodically).
Based on the results, conclusions are drawn about the presence or absence of the following signs of hypertrophy.
Shift of the cardiac EO to the right
In cases where HPP is caused or associated with right ventricular hypertrophy, a deviation of the electrical axis of the heart to the right may be observed on the ECG. The normal position of the EO is between 0◦ and 90◦; if the degree measure belongs to the interval 90◦-99◦, a slight deviation of the axis to the right is recorded. At values of 100◦ and above, a significant axis shift is indicated.
We will not give the formula for the angle value here, but we will show you how to “by eye” determine the right-sided displacement of the EO from the cardiogram. To do this, you need to check whether the following conditions are met:
- In lead I: the S wave is negative, the R wave is positive, but its height is less than the depth of S.
- In leads II and III: the height of the R wave is an order of magnitude higher than the same height in lead I. In addition, when comparing the R waves in leads II, III, the latter should be higher.
"Pulmonary heart" (P-pulmonale)
Pathological changes in the pulmonary (lat. pulmonale) circulation are a common cause of HPP. On the ECG they are reflected by modifications of the first (atrial) P wave.
With normal functioning of the atria, the P wave has a non-sharp, smoothed apex; but with HPP, a high, pointed “peak” is observed in leads II, III, aVF. The explanation for this fact is as follows: the P wave line represents the sum of two peaks - excitations of each of the atria.
- Normally, excitation of the RA precedes excitation of the LA; the extinction of excitations occurs in the same order. The P- and L-curves intersect, and the point of their intersection corresponds to the top of the “dome” of the P wave.
- With HPP, the excitation of the LA occurs after the excitation of the PP, but they attenuate almost simultaneously. The amplitude of the P-peak is greater, and it completely “absorbs” the L-peak - this is reflected in the shape of the total curve.
It should be understood that a set of P-pulmonale signs can be present on the cardiogram not only during hypertrophy, but also during functional overload of the PP - this happens, for example, against the background of hyperthyroidism, tachycardia, coronary heart disease, etc.
Consequences of GPP
In chronic diseases of the pulmonary system, the active alveoli are replaced by fibrous tissue, and the gas exchange area becomes smaller. Microcirculation is also disrupted, which leads to increased pressure in the pulmonary circulation. The atria have to actively contract, which ultimately causes their hypertrophy.
Thus, the complications and consequences of GPP are:
- expansion of the heart chambers;
- circulatory disorders, first in the small and then in the large circle;
- formation of the pulmonary heart;
- venous congestion and heart valve insufficiency.
If left untreated, pulse irregularities and attacks of heart failure may develop, which can lead to death.
Treatment
Normalizing the size of the atrium and improving the functioning of the heart muscle is only possible if the underlying disease – the cause of the pathology – is treated. Such treatment is always complex; monotherapy does not make sense.
In the presence of pulmonary pathology, these are bronchodilators (tablets and inhalers), antibacterial therapy for bacterial etiology of disorders, anti-inflammatory drugs.
For bronchiectasis, surgical treatment is used.
In case of heart defects, the best solution is corrective surgery. After heart attacks and myocarditis, it is necessary to prevent remodeling with the help of antihypoxic and cardioprotective drugs.
Antihypoxants are indicated: Actovegin, Mildronate, Mexidol and Preductal. Cardioprotectors: ACEs or angiotensin II receptor antagonists (ARA II). They can actually slow down the onset of chronic heart failure. The most commonly prescribed drugs are Enalapril, Quadropril, Perindopril, etc.
Nitrones, beta blockers (Metoprolol, Bisoprolol, Nebivalol, etc.), ACE inhibitors, antiplatelet agents that prevent the formation of blood clots, statins that normalize the amount of cholesterol are required.
Also used in treatment are glycosides (according to indications) and antiarrhythmics, agents that improve metabolic processes in the heart muscle. Judging by the reviews, good results were obtained when prescribing Riboxin.
Ventricular arrhythmia
- 1 Types of ventricular arrhythmia
- 2 Causes of pathology 2.1 Symptoms of ventricular arrhythmia
- 4.1 Prevention and prognosis
A pathology such as ventricular arrhythmia in severe cases can lead to serious consequences, including death. This disease has a certain classification, and the choice of therapy depends on the timeliness of diagnosis and the patient’s health condition. Timely measures provide a favorable prognosis for the patient’s future.
Types of ventricular arrhythmia
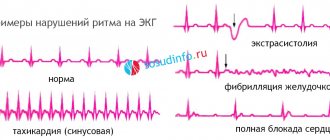
Arrhythmia is a pathology caused by disruptions in the frequency, rhythm, sequence of contractions and excitations of the heart muscle. In a healthy person, the heart contracts at regular intervals; the contraction frequency can range from 60 to 80 beats per minute. Deviation from these numbers is considered an arrhythmia. The disease can develop rapidly, sometimes even causing death. Therefore, it is imperative to treat this disease, otherwise the consequences will not keep you waiting.
| View | The essence of pathology | Subspecies |
| Extrasystole | Abnormally rapid heartbeat and premature contractions. |
|
| Ventricular tachycardia | Slow or abnormal heart rhythm as a result of the development of a ventricular ectolithic lesion. |
|
| Ventricular fibrillation (recurrent ventricular arrhythmia) | Arrhythmic, uncoordinated and ineffective contractions of the ventricles. Ventricular contraction occurs more than 300 beats per minute. |
|
Return to contents
Causes of pathology
Ventricular arrhythmia develops due to organic heart damage caused by the following diseases and conditions:
on
- hypertension;
- myocarditis of various origins;
- heart attack and recovery period;
- rheumatic heart disease;
- shock or severe heart failure;
- rheumatic heart defects;
- poisoning with drugs based on quinidine, adrenaline or chloroform;
- manipulations on the heart.
Bad habits, acid-base balance disorders, potassium deficiency, and hyperthyroidism accelerate the development of the disease. Heavy training and physical overexertion also cause attacks of arrhythmia.
Return to contents
Symptoms of ventricular arrhythmia
This cardiac pathology has characteristic symptoms:
- weakness, dizziness, darkening of the eyes;
- collapse, circulatory disorders, drop in pressure due to congestion and a reduced amount of blood;
- increased or slowed heart rate;
- lump in the throat;
- attack of fear, fainting;
- paleness of the skin;
- cerebral ischemia;
- depressed respiratory function, shortness of breath;
- recurrent or frequent heart pain;
- digestive disorders, the stomach cannot cope with stress, vomiting, nausea, and disorders develop;
- paresis, swelling, convulsions and other focal disorders.
Return to contents
Diagnostic measures
Identified features or pathology should be illustrated with ECG printouts for the corresponding monitoring period.
This disease is similar in symptoms to other heart diseases, so diagnosis includes standard procedures:
- ECG during the day;
- ECG under stress;
- blood test for biochemistry and electrolytes.
This type of disease is often a consequence of myocardial diseases, so sometimes the doctor prescribes additional tests:
- tomography;
- X-ray;
- Ultrasound of the heart;
- rhythmography.
Return to contents
Treatment of arrhythmia
If the development of the disease is not associated with concomitant pathologies, as a rule, treatment comes down to preventive measures. The doctor will recommend staying away from stress, getting rid of bad habits, and not taking medications without a doctor’s prescription. Treatment is prescribed if the symptoms are pronounced or the type of extrasystoles poses a threat to life.
The doctor prescribes beta-blockers if the patient has had a heart attack, and additional studies are performed to assess the risk of death. Medicines for arrhythmia are also prescribed, but under the supervision of a doctor, since together with the suppression of extrasystoles, the risk of complications increases. If the drugs are not effective, the doctor will prescribe radiofrequency catheter ablation.
Return to contents
Prevention and prognosis
Without treatment, the pathology can cause sudden death. Complications include atrial fibrillation, heart failure, and myocardial changes. Atrial fibrillation is fraught with complications: cardiogenic shock, cardiomyopathy, thrombus formation in the atria. For frequent attacks, a doctor's consultation is necessary. The patient's future prognosis depends on several factors:
- forms of the disease;
- presence of signs of problems with blood circulation;
- the presence of organic pathologies of the heart muscle.
Gastric arrhythmia is a type of heart rhythm disorder. When diagnosed, treatment is prescribed based on the patient’s condition on an individual basis. Despite the fact that a certain type of pathology does not require treatment, it is better to play it safe and undergo all the necessary examinations to avoid undesirable consequences in the future.
on
A comment
Nickname
Relapse Prevention
If drug therapy is the prerogative of the doctor, greater responsibility falls on the patient himself. Without his participation, the efforts of doctors will not produce results. A person must definitely reconsider his lifestyle: give up smoking and alcohol, establish proper nutrition, eliminate physical inactivity, adhere to a daily routine, exercise moderate physical activity, and normalize body weight. If pathologies of the cardiovascular and pulmonary systems become chronic, they cannot be completely cured.
The condition can only be improved by preventing exacerbations of these pathologies. Then the load on the cardiac system decreases.
GPP and pregnancy
During pregnancy, the body undergoes enormous changes not only in terms of hormonal balance, but also in the functioning of internal organs. A difficult situation arises when diagnosing right atrium overload during pregnancy, which in this situation is considered an extragenital disease. The diagnosis must not only be established, but also the woman’s ability to bear a fetus and give birth.
The best option, of course, is to diagnose heart pathologies before conception, but this does not always happen. Most often, pregnant women with heart pathologies are hospitalized three times during gestation; this is done to monitor the condition over time.
When first admitted to the hospital, the defect is examined, the activity of the process is determined and the work of the blood circulation is assessed, taking into account the question of a possible termination of pregnancy.
Repeated hospitalization is necessary because the physiological stress of the body to maintain the functioning of the heart muscle in a woman reaches its peak. The third hospitalization helps doctors choose the method of delivery.
Preventive actions
Prevention of right atrium hypertrophy begins with a review of the lifestyle, which involves proper balanced nutrition and a rational work and rest schedule. If you are not a professional athlete and you do not necessarily need Olympic medals, do not show stubborn fanaticism in playing sports. This exhausts the body and exhausts the heart. The pressure in the circulatory system increases, and hypertrophy will not take long to occur. Daily walks of an hour a day, swimming, and cycling are quite enough.
Another problem is eliminating stress. They also have a very negative impact on the functioning of the heart and the entire body as a whole. Yoga, meditation, and relaxation can help solve the problem.