0
Author of the article: Marina Dmitrievna
2017.07.07
141
Symptoms
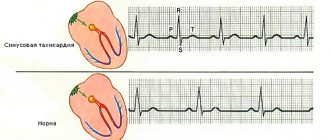
Atrial tachycardia (AT) is classified as a disease of the supraventricular zone of the heart. It often manifests itself as a rapid heartbeat of 100 to 130 beats per minute. Ectopic impulses that come from the atria cause rapid heartbeat. This change in the work of the heart is associated with increased automaticity of the centers of the II and III orders.
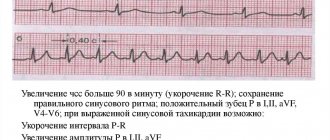
ECG PT
Pathological electrical impulses manifest themselves in one or more foci, which provoke the heart. Often 2 or more lesions are observed in elderly patients. If multiple foci are diagnosed, the atria are excited so often that this leads to heart flutter. The main sign of pathology that can be seen on the electrocardiogram is considered to be P waves. They are separated by an isoline that distinguishes atrial flutter from AT. In most cases, cardiologists diagnose right atrial tachycardia. Only 30% of patients have left atrial AT. The average rapid heart rate in this state can vary between 160-190 beats per minute. In advanced stages, the heartbeat can develop up to 240 beats per minute.
Signs and symptoms
Manifestations of atrial tachycardia include:
- Rapid pulse: In most cases of atrial tachycardia, the fast pulse is regular; it may be irregular in fast atrial tachycardias with variable AV conduction and in multifocal atrial tachycardia.
- Episodic or paroxysmal nature of occurrence;
- Sudden onset of palpitations;
- Continuous, prolonged or repeated tachycardia (if atrial tachycardia is caused by increased automaticity);
- Tachycardia gradually accelerates soon after onset;
- Shortness of breath, dizziness, fatigue or chest pressure: during tachycardic episodes accompanied by fluttering;
- Fainting with fast heart rate and severe hypotension;
- Symptoms of heart failure and decreased exercise capacity: early manifestations of tachycardia-induced cardiomyopathy in patients with recurrent tachycardias.
Patients who have multifocal tachycardia may have an underlying disease that is causing the tachycardia. Such diseases may include pulmonary, cardiac, metabolic and endocrinopathic disorders. Chronic obstructive pulmonary disease (COPD) is the most common underlying disease (60% of cases) in multifocal tachycardia.
Supraventricular atrial tachycardia is not uncommon in patients with a history of surgical repair of atrial septal defect. Connective tissue in the atrium can lead to the formation of a reentrant circuit.
When examining a patient, the most important abnormal symptom is a fast pulse. The heart rate is usually regular, but it may be irregular in rapid atrial tachycardia with variable AV conduction. Blood pressure may be low in patients who are tired, dizzy, or lightheaded.
Clinical picture
Atrial tachycardia, which occurs in young people who do not suffer from organic diseases, can be asymptomatic. In some cases, a poor clinical picture is observed - a rapid heartbeat is felt, slight shortness of breath and dizziness occur.
In people suffering from cardiovascular and pulmonary diseases, atrial tachycardia is more complicated. The severity of the clinical picture depends on the number of pathologies, the general condition of the person and the form of the rhythm disorder. In this case, symptoms of concomitant diseases are added to the signs of tachycardia.
Paroxysmal atrial tachycardia is accompanied by a clear clinical picture:
- Sudden onset of rapid heartbeat;
- Severe weakness;
- Dizziness;
- Darkening of the eyes, possible fainting;
- Cold clammy sweat;
- With the development of tachycardia against the background of pulmonary diseases, expiratory shortness of breath occurs;
- If paroxysmal tachycardia occurs due to heart disease, pain in the chest is possible.
During paroxysm, hemodynamic parameters change - the pulse increases to 150-250 beats/min while maintaining rhythm, and sometimes hypotension develops (decreased blood pressure).
Non-paroxysmal (chronic) atrial tachycardia is clinically milder. This is explained by the body’s adaptation to an almost constantly increased heart rate.
Classification methods
A number of methods are used to systematize atrial tachycardia. Classification in terms of origin may be based on endocardial activation mapping data, pathophysiological mechanisms and anatomy.
Based on endocardial activation, atrial tachycardia can be divided into the following two groups:
Focal atrial tachycardia : arises from a localized area in the atria, such as the ridge border, pulmonary veins, coronary sinus ostium, or intra-atrial septum.
Atrial reentry tachycardia : Recurrent atrial tachycardia most often occurs in patients with structural or complex heart disease, especially after atrial surgery.
Other classification methods include:
Pathophysiological mechanisms: Atrial tachycardia can be classified as the result of increased automaticity, triggered activity, or a re-entry mechanism.
Anatomical methods: Classification of atrial tachycardia can be based on the location of the arrhythmogenic focus.
Development mechanism
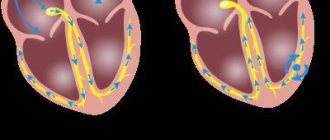
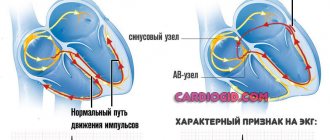
The basis of the development mechanism is the functional division of the AV node into two channels, which have their own electrophysiological properties.
Along the first of them, electrical impulses travel at a fast pace, while through the second, at a slow pace. The different speeds of their transmission provoke the formation of an additional pathway, the so-called re entry loop.
The following stages of formation of such a mechanism are distinguished:
- The occurrence of atrial extrasystole;
- Formation of a blockade of the passage of electrical impulses in the first (fast) channel;
- Transmission of electrical impulses through the second (slow channel) from the atria to the ventricles;
- Restoration of pulse transmission in the fast channel;
- Retrograde impulse transmission into the fast channel, then again into the slow one.
This formation of an additional wave of excitation is observed in a typical form of reciprocal tachycardia. Atypical forms are less common, when the mechanism starts in reverse or reverse electrical impulses pass through a slow channel.
Reciprocal tachycardia is provoked by atrial extrasystoles or a large time difference between the speed of transmission of electrical impulses.
Anatomy
Atrial tachycardia can be of right or left atrial origin. Individual atrial tachycardias actually occur outside the normal anatomical confines of the atria in areas such as the superior vena cava, pulmonary veins, and the vein of Marshall (the oblique vein of the left atrium), into which bundles of atrial myocardium extend. More rare locations, such as the noncoronary aortic valve and hepatic veins, have also been described.
Anisotropic conduction in the atria as a result of complex fiber orientation can create an area of slow conduction. Certain atrial tissues, such as the ridge border and pulmonary veins, are standard sites of automatic or triggered activity. In addition, disease processes or age-related atrial degeneration can lead to an arrhythmogenic process.
Abnormalities that have been noted at sites of atrial tachycardia may include the following:
- Extensive myocardial fibrosis
- Myocyte hypertrophy
- Endocardial fibrosis
- Mononuclear cell infiltration
- Mesenchymal cell proliferation
Prevention
First of all, prevention of atrial tachycardia comes down to lifestyle correction. To do this, you must follow the following recommendations:
- Eat rationally;
- Avoid excessive physical activity;
- Avoid stressful situations;
- Quit smoking, reduce alcohol consumption;
- Change your place of work if there is a high risk of occupational hazards.
Secondary prevention includes regular use of antiarrhythmic therapy, treatment of concomitant and background diseases, periodic visits to preventive medical examinations, as well as to the attending physician to correct the prescribed therapy.
Causes
Atrial tachycardia can occur in people with typical cardiovascular disease or in patients with organic heart disease. When it occurs in patients with congenital heart disease who have undergone corrective or palliative cardiac surgery, atrial tachycardia can have potentially life-threatening consequences.
Atrial tachycardia, resulting from exercise, catecholamine crisis, alcohol consumption, hypoxia, metabolic disorders, or use of stimulants or narcotics (eg, caffeine, albuterol, theophylline, cocaine), is due to increased automation or triggering activity.
Atrial re-entry tachycardia tends to occur in patients with structural heart diseases, in particular ischemic, congenital, postoperative and valvular disorders. Iatrogenic atrial tachycardia has become more common and is usually caused by ablative procedures in the left atrium. Several typical sites of origin for these tachycardias have been identified, including the mitral isthmus (between the left inferior pulmonary vein and the mitral valve), the superior left atrium, and, in a re-entry pattern, around the pulmonary veins.
MAT is often associated with underlying medical conditions, often occurring in patients suffering from exacerbation of chronic obstructive pulmonary disease, pulmonary thromboembolism, exacerbation of heart failure, or severe illness, especially when critically treated with inotropic infusions. MPT is often associated with hypoxia and sympathetic stimulation.
Other major conditions that are commonly associated with MMT are the following:
- Heart valve disease
- Diabetes
- Hypokalemia
- Hypermagnesemia (high magnesium content)
- Azotemia
- Postoperative condition
- Sepsis
- Toxicity of methylxanthine
- Myocardial infarction
- Pneumonia
Unnatural forms of atrial tachycardia can be observed in patients with an infiltrative process, including the pericardium and, as a continuation, the atrial wall.
Complications
In the absence of therapy or receiving it irregularly, the risk of various complications increases. Elderly people with cholesterol problems and not taking antiplatelet drugs are at high risk of developing thromboembolic complications.
The clinical picture depends on where the occlusion by the thrombus occurred. If a blood clot gets into the coronary arteries, symptoms of coronary artery disease (angina or myocardial infarction) occur:
- Pain syndrome behind the sternum of varying intensity;
- Irradiation of pain under the left shoulder blade, into the left half of the jaw or arm;
- Feeling of fear, cold sticky sweat, difficulty breathing.
When a blood clot enters the vessels of the brain, an acute cerebrovascular accident (stroke) develops:
- Aphasia, dysphagia;
- Smoothing of the nasolabial fold, facial asymmetry;
- Weakness or numbness in an arm and leg on one side;
- Impaired balance and orientation;
- Dizziness, nausea and vomiting.
If a blood clot blocks the pulmonary artery, a pulmonary embolism syndrome occurs:
- Pallor, cyanosis of the skin;
- Chest pain;
- Shortness of breath with the development of respiratory failure;
- Decreased blood pressure and increased heart rate.
Also, atrial tachycardia can lead to the development of arrhythmogenic shock - an extreme degree of circulatory disorder, accompanied by general weakness, impaired consciousness, decreased diuresis, a sharp drop in blood pressure and increased heart rate.
Diagnostics
The rhythm strip ECG is the primary diagnostic tool for identifying, locating, and differentiating atrial tachycardia. Laboratory tests may be ordered to rule out systemic diseases that may lead to tachycardia. An electrophysiological study may also be required. P-wave morphology provides important clues about the origin of tachycardia, and it is for this reason that the 12-lead ECG is essential.
When diagnosing atrial tachycardia, the following diagnostic methods can be used:
- Electrocardiography with rhythmic stripe. For identification, location and differentiation of atrial tachycardia;
- Holter monitor: to analyze the beginning and end of an episode of atrial tachycardia, identify AV conduction block during the episode, and correlate symptoms with atrial tachycardia;
- Endocardial mapping: to localize atrial tachycardia.
Exclusion of systemic disorders
When starting work on atrial tachycardia, appropriate laboratory testing should be performed to rule out systemic causes of sinus tachycardia (eg, fever, hyperthyroidism, anemia, dehydration, infection, hypoxemia, metabolic disease).
The following laboratory tests can help exclude systemic causes of sinus tachycardia:
- Determination of blood serum: exclude disturbances in electrolyte metabolism;
- Level of hemoglobin in blood and red blood cells: exclusion of anemia;
- Arterial blood gas analysis: to determine the condition of the lungs;
- Serum digoxin test: if digitalis toxicity is suspected.
The following tests may be helpful in diagnosing atrial tachycardia:
Chest X-ray : in patients with cardiomyopathy caused by tachycardia or complex congenital heart disease;
Computed tomography (CT) scan : excludes pulmonary embolism, assesses pulmonary vein anatomy and obtains images before the ablation procedure;
Echocardiography : exclusion of heart pathology and analysis of the size of the left atrium, determination of blood pressure in the pulmonary artery, left ventricular function and pericardial pathology.
Treatment
Primary treatment during an attack of atrial tachycardia is rate control using AV node blocking agents (eg, beta blockers, calcium channel blockers). Antiarrhythmic drugs can prevent relapse; A calcium channel blocker or beta blocker may also be needed in combination therapy.
Specific antiarrhythmic therapies include the following:
Overactive atrial tachycardia: Verapamil, beta blockers and adenosine;
Atrial tachycardia with increased automaticity: beta blockers, but overall rates of improvement with treatment are low;
Recurrent atrial tachycardia: class Ic antiarrhythmic drugs
Maintenance of sinus rhythm: Class III antiarrhythmic drugs
Non-pharmacological treatments for atrial tachycardia
Cardioversion : used for patients who do not have good hemodynamics of the heart rhythm or for whom drugs that control heart rate control are ineffective or contraindicated.
Radiofrequency catheter ablation : for patients refractory to treatment. Radiofrequency catheter ablation for atrial tachycardia has become a fairly successful and effective treatment option for symptomatic patients whose condition is refractory to medical therapy or who are unwilling to undergo long-term antiarrhythmic treatment. It can treat re-entry forms and focal forms of atrial tachycardia.
Surgical ablation : used for patients with complex congenital heart disease.
Multifocal atrial tachycardia
Treatment for multifocal atrial tachycardia (MAT) involves treating the underlying cause that causes the heart to beat faster.
Treatment may also include the following medications:
- Calcium channel blockers: used as first line of therapy;
- Magnesium sulfate: When administered to correct hypokalemia, most patients return to normal sinus rhythm;
- Beta blockers;
- Antiarrhythmic drugs.
In very rare cases where MPT is persistent and refractory, the use of AV-compatible radiofrequency ablation and permanent pacemaker implantation should be considered. This treatment may improve symptoms and hemodynamics and prevent the development of tachycardia-mediated cardiomyopathy. In general, brief and asymptomatic episodes of atrial tachycardia detected as incidental findings on ambulatory ECG do not require treatment.
In adults, tachycardia is generally defined as a heart rate greater than 100 beats per minute (bpm). In children, the definition of tachycardia varies because the normal heart rate depends on age:
- Age 1-2 days: 123-159 beats/min
- Age 3-6 days: 129-166 beats/min
- Age 1-3 weeks: 107-182 beats/min
- Age 1-2 months: 121-179 beats/min
- Age 3-5 months: 106-186 beats/min
- Age 6-11 months: 109-169 beats/min
- Age 1-2 years: 89-151 beats/min
- Age 3-4 years: 73-137 beats/min
- Age 5-7 years: 65-133 beats/min
- Age 8-11 years: 62-130 beats/min
- Age 12-15 years: 60-119 beats/min
As with most cases of supraventricular tachycardia, the electrocardiogram typically demonstrates a narrow QRS complex tachycardia (unless trochlear aberration occurs). Heart rate can vary greatly, ranging from 100-250 beats/min. The atrial rhythm is usually regular.
The accompanying ventricular rhythm is also usually regular. However, it can become irregular, especially at higher atrial rates, due to variable conduction across the AV node, thus creating conduction patterns such as 2:1, 4:1, a combination of these, or Wenckebach AV block.
The morphology of P-waves on the ECG allows us to determine the site of origin, as well as the mechanism of atrial tachycardia. In the presence of focal tachycardia, P-wave morphology and axis depend on the location in the atrium from which the tachycardia originates. In the presence of a macro-re-entry tachycardia pattern, P-wave morphology and axis depend on activation patterns.
Multifocal atrial tachycardia is an arrhythmia with an irregular atrial rate greater than 100 beats/min. Atrial activity is well organized, with at least three morphologically distinct P waves, irregular PP intervals, and an isoelectric base between waves. Multifocal atrial tachycardia was previously called chaotic atrial rhythm or tachycardia, chaotic atrial mechanism, and repetitive paroxysmal MPT.
Epidemiology
Atrial tachycardia can occur at any age, although it is more common in people with congenital heart defects. MPT is a relatively rare form of arrhythmia, with a prevalence of 0.05-0.32% in hospitalized patients. It is predominantly seen in men and older adults, particularly older patients with multiple medical problems. The average age of the disease is 72 years.
Forecast
In patients with normal heart structure, atrial tachycardia has a low mortality rate. However, tachycardia-induced cardiomyopathies develop in patients with sustained or frequent atrial tachycardia. Patients with underlying structural heart disease, congenital heart disease, or pulmonary disease are less likely to tolerate atrial tachycardia.
(No Ratings Yet)
Risk factors
In addition to the main causes, atrial tachycardia can develop in people at risk with the following pathologies:
- Increased blood levels of thyroid and adrenal hormones;
- Arterial hypertension;
- Frequent respiratory diseases;
- Obesity;
- Occupational hazards (chemical intoxication, radiation exposure);
- Burdened heredity.
Paroxysm of atrial tachycardia is usually provoked by a stressful situation, excessive physical activity, a sharp change in air temperature, and smoking.