ARTERIES
(Greek
arteria
, singular) - blood vessels that carry blood, enriched with oxygen in the lungs, from the heart to all parts and organs of the body.
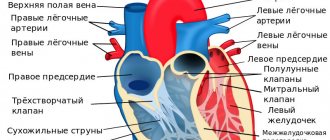
The exception is the pulmonary trunk (see), which carries venous blood from the heart to the lungs. Rice.
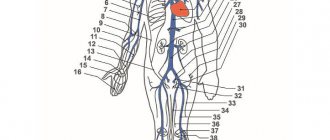
2. Arteries of the anterior surface of the leg and dorsum of the foot: 1 - a. genus descendens (ramus articularis); 2 - rami musculares; 3 - a. dorsalis pedis; 4 - a. arcuata; 5 - ramus plantaris profundus; 6 - aa. digitales dorsales; 7 - aa. metatarseae dorsales; 8 - r. perforans a. peroneae; 9 - a. tibialis ant.; 10 - a. recurrens tibialis ant.; 11 - rete patellae et rete articulare genus; 12 - a. genus superior lat. Rice. 3. Arteries of the popliteal fossa and posterior surface of the leg: 1 - a. poplitea; 2 - a. genus superior lat.; 3 - a. genus inferior lat.; 4 - a. peronea (fibularis); 5 - rr. malleolares lat.; 6 - rr. calcanei (lat.); 7 - rr. calcanei (med.); 8 - rr. malleolares med.; 9 - a. tibialis post.; 10 - a. genus inferior med.; 11 - a. genus superior med. In ancient times, the idea was created that air or air and blood circulated in the arteries, since when autopsies were made, the arteries were found to be empty in most cases. The ancient Greeks also used the term “artery” to designate the windpipe—the trachea.
The set of arteries: from the largest trunk - the aorta (see), originating from the left ventricle of the heart, to the smallest branches in the organs - precapillary arterioles - constitutes the arterial system (color. Fig. 2-6), representing part of the cardiovascular system ( cm.).
Arteries or their branches are named according to various characteristics: by topography (for example, a. subclavia, a. poplitea), by the name of the organ that they supply with blood (for example, a. renalis, a. uterina, a. testicularis), or part body (eg, a. dorsalis pedis, a. femoralis).
A number of arteries have several names (synonyms), which appeared as a result of the revision of anatomical nomenclatures. Some large arteries are called the trunk (truncus), small arterial vessels are called branches (rami), the smallest arteries are called arterioles (arteriola), arterioles that turn into capillaries (see) are called precapillary arterioles (arteriola precapillaris), or metarterioles (metarteriola) . Rice.
6. Arteries of the head, trunk and upper extremities: 1 - a. facialis; 2 - a. lingualis; 3 - a. thyroidea sup.; 4 - a. carotis communis sin.; 5 -a. subclavia sin.; 6 - a. axillaris; 7—arcus aortae; aorta ascendens; 9 - a. brachialis sin.; 10 - a. thoracica int.; 11—aorta thoracica; /2— aorta abdominalis; 13 -a. phrenica inf. sin.; 14 - truncus celiacus; 15 -a. mesenterica sup.; 16 - a. renalis sin.; 17 - a. testicularis sin.; 18 -a. mesenterica inf.; 19 -a. ulnaris; 20 -a. interossea communis; 21 - a. radialis; 22 -a. interossea ant.; 23—a. epigastrica inf.; 24—arcus palmaris superficialis; 25—arcus palmaris profundus; 26 - aa. digitales palmares communes; 27—aa. digitales palmares propriae; 28 -aa. digitales dorsales; 29 - aa. metacarpeae dorsales; 30 - ramus carpeus dorsalis; 31 - a. profunda femoris; 32—a. femoralis; 33 - a. interossea post.; 34 -a. iliaca externa dext.; 35 - a. iliaca int. dext.; 36 - a. sacralis mediana; 37 - a. iliaca communis dext.; 38 - aa. lumbales; 39 - a. renalis dext.; 40 - aa. intercostales post.; 41 - a. profunda brachii; 42 - a. brachialis dext.; 43 - truncus brachiocephalicus; 44 - a. subclavia dext.; 45 -a. carotis communis dext.; 46 - a. carotis ext.; 47 - a. carotis int.; 48 - a. vertebralis; 49 - a. occipitalis; 50 -a. temporalis superficialis. Rice. 1. Development of human arteries. A - D - development of the celiac trunk, superior and inferior mesenteric arteries in the embryo: A - 4th week; B - 5th week, C - 6th week; G - 7th week; D - arteries of the body wall in an embryo of the 7th week 1 - pharynx; 2 - pulmonary kidney; 3 - liver; 4 - a. omphalomesenterica; 5 - a. umbilicalis; 6 - hindgut; 7 - allantois; 8 - yolk sac; 9 - stomach; 10 - ventral segmental artery; and - a. vertebralis; 12 - a. subclavia; 13 - truncus celiacus; 14 - pancreas; 15 - a. mesenterica inf.; 16 - a. basilaris; 17 - large intestine; 18 - a. sacralis mediana; 19 - a. mesenterica sup.; 20 - a. carotis ext.; 21—a. intercostalis suprema; 22 - aorta; 23 - a. intercostalis post.; 24 - a. lumbalis; 25 - a. epigastrica inf.; 26 - a. ischiadica; 27 - a. iliaca ext.; 28 - a. thoracica int.; 29 - a. carotis int.
Functions of arteries
Considering the anatomy of the artery, it is easy to assess its morphological qualities. This is a hollow elastic tube whose main function is to transport blood from the heart to the capillary bed. But this task is not the only one, since these vessels also perform other important functions. Among them:
- participation in the hemostasis system, counteraction to intravascular thrombosis, closure of vascular damage by a thrombus;
- formation of a pulse wave and its transmission to vessels with a smaller caliber;
- maintaining blood pressure levels in the lumen of blood vessels at a great distance from the heart;
- formation of venous pulse.
Hemostasis is a term that characterizes the presence of a coagulation and anticoagulation mechanism within each blood vessel. That is, after a non-critical injury, the artery itself is able to restore blood flow and close the defect with a blood clot. The second component of the hemostatic system is the anticoagulant system. This is a complex of enzymes and receptor molecules that destroy the blood clot that forms without violating the integrity of the vascular wall.
If a blood clot has formed independently due to disorders not related to bleeding, the hemostasis system of arteries and veins will dissolve it independently in the most effective way available. However, this becomes impossible if the thrombus blocks the lumen of the artery, which is why thrombolytics of the anticoagulation system will not be able to reach its surface, as happens with myocardial infarction or PE.
Functions
Human arteries (their location diagram is presented in the article) are inherently transmission vessels. The largest of them branch off from the heart and lungs and follow along the spine to the main skeletal bones. Both oxygen-enriched and oxygen-depleted blood can move through the arteries.
The vessels that carry blood from the heart are resistant to stretching. Therefore, their anatomical structure changes over time. Namely: in large arteries the inner layer thickens, and in more distant arteries the outer and middle layers thicken.
Blood vessels leading biological fluid to organs and tissues have the following functional characteristics:
- transportation;
- protective;
- exchange;
- regulatory
Artery pulse wave
The anatomy of veins and arteries is also different due to the difference in hydrostatic pressure in their lumen. In arteries, the pressure is much higher than in veins, which is why their wall contains more muscle cells, and the collagen fibers of the outer membrane are better developed in them. Blood pressure is generated by the heart at the moment of left ventricular systole. Then a large portion of blood stretches the aorta, which, due to its elastic properties, quickly contracts back. This allows blood to be taken from the left ventricle first and then sent onward when the aortic valve closes.
As it moves away from the heart, the pulse wave will weaken, and it will not be enough to push blood through elastic stretching and compression alone. To maintain a constant level of blood pressure in the vascular arterial bed, muscle contraction will be required. To do this, there are muscle cells in the medial layer of the arteries, which, after nervous sympathetic stimulation, will generate a contraction and push the blood to the capillaries.
The pulsation of the arteries also allows blood to be pushed through the veins, which are located in close proximity to the pulsating vessel. That is, arteries in contact with nearby veins generate their pulsation and help return blood to the heart. Skeletal muscles perform a similar function during their contraction. Such assistance is necessary to push venous blood upward against gravity.
Peripheral artery diseases
2. Pain in the lower back
The arteries located in the lower back are the areas where plaque forms most quickly. This is the most dangerous area in the human body.
Lower back pain may be one of the first signs of clogged arteries.
The reason why you experience pain in the lower back is the result of clogged arteries. This situation occurs due to a lack of blood on the intervertebral discs, which are the natural lubricant for your vertebrae.
Lack of normal blood functioning in these places can lead to hernia and pinched nerves.
3. Calf pain
Pain in the calf area may be the result of arteriosclerosis. Thickening or hardening of arterial walls that block blood flow to the legs can lead to serious problems.
If something similar happens to you, and you often experience pain in the calf area, be sure to consult a specialist. One of the common symptoms of this problem is lameness.
Experts say people who smoke at least a few cigarettes a day are at higher risk of arteriosclerosis, which can ultimately lead to the development of claudication. Be sure to pay attention to this symptom.
Source
Types of arterial vessels
The anatomy of an artery varies depending on its diameter and distance from the heart. More precisely, the general plan of the structure remains the same, but the expression of elastic fibers and muscle cells changes, as well as the development of the connective tissue of the outer layer. The artery consists of a multilayer wall and cavity. The inner layer is the endothelium, located on the basement membrane and subendothelial connective tissue base. The latter is also called the internal elastic membrane.
Structure of arteries
The walls of all arteries consist of three layers:
- inner layer or endothelium
- middle layer consisting of strong and elastic fibers and muscle cells
- the superficial layer or adventitia is a dense and durable membrane
The inner layer of arteries is the endothelium
The endothelium is a single layer of flat cells. These cells serve as a barrier between the blood and the rest of the world. It is impossible to enumerate all the functions that this thin microscopic layer of cells performs. I will list just a few of them:
- Barrier - keeps all substances, including water and oxygen, in the blood, preventing their leakage.
- Filtration - regulates (filters) the flow of substances from the blood into the tissues and vice versa. That is, it decides which substances, in what quantity and in what place should leave the blood or, conversely, come from the outside.
- Regulatory - takes part in the regulation of vascular tone, pressure inside blood vessels, and heart rate.
- Hemostatic - actively participates in the formation of blood clots.
Middle layer
This layer is designed to strengthen the walls of the arteries. After all, they have to withstand high pressure. The highest pressure in the entire circulatory system. After all, the heart, as we have already agreed, forcefully pushes blood into the arteries. And they must withstand this shock wave, not break or fail.
Elastic fibers give them hardness, stability and elasticity. But muscle cells allow you to narrow and expand the lumen of the arteries, thereby regulating the pressure and speed of blood flow.
Superficial layer - adventitia
This is a dense layer of connective tissue that covers the outside of the arteries and also strengthens the vessel wall.
Differences in Artery Types
The middle layer is where the greatest differences exist between types of arteries. It contains elastic fibers and muscle cells. On top of it is an outer elastic membrane, completely covered on top with loose connective tissue, allowing the smallest arteries and nerves to penetrate into the middle shell. And depending on the caliber, as well as the structure of the middle shell, there are 4 types of arteries: elastic, transitional and muscular, as well as arterioles.
Arterioles are the smallest arteries with the thinnest connective tissue membrane and absent elastic fibers in the middle membrane. These are one of the most common arterial vessels directly adjacent to the capillary bed. In these areas, the main blood supply changes to regional and capillary. It flows in the interstitial fluid directly near the group of cells to which the vessel approaches.
Arteries
Arteries are blood vessels that carry arterial blood rich in oxygen and nutrients from the heart to all parts of the body. The exception is the arteries of the pulmonary circulation, through which venous blood moves from the heart to the lungs. The totality of all arteries forms the arterial system, which is part of the cardiovascular system.
The largest artery is the aorta. Arteries branch off from it, which branch and become smaller as they move away from the heart. The thinnest arteries are called arterioles. In the thickness of the organs, the arteries branch up to the capillaries (see). Nearby arteries are often connected by anastomoses through which collateral blood flow occurs. Typically, arterial plexuses and networks are formed from anastomosing arteries. The artery that supplies blood to a section of an organ (segment of the lung, kidney, liver) is called segmental.
The artery wall consists of three layers: the inner - endothelial, or intima, the middle - muscular, or media, with a certain amount of collagen and elastic fibers and the outer - connective tissue, or adventitia; the wall of the artery is richly supplied with vessels and nerves, located mainly in the outer and middle layers. Based on the structural features of the wall, arteries are divided into three types: muscular, muscular-elastic (for example, carotid arteries) and elastic (for example, the aorta). Muscular arteries include small and medium-sized arteries (for example, radial, brachial, femoral). The elastic frame of the artery wall prevents its collapse, ensuring the continuity of blood flow in it.
Usually the arteries lie for a long distance deep between the muscles and near the bones, to which the artery can be pressed during bleeding. A pulse is felt in a superficial artery (for example, the radial artery).
The walls of the arteries have their own blood vessels (“vasa vasa”) supplying them. Motor and sensory innervation of the arteries is carried out by sympathetic, parasympathetic nerves and branches of the cranial or spinal nerves. The nerves of the artery penetrate the middle layer (vasomotors - vasomotor nerves) and contract the muscle fibers of the vascular wall and change the lumen of the artery.
Pathology of the artery - see Aneurysm, Arteritis, Atherosclerosis, Endarteritis. See also Blood vessels.
Rice. 1. Arteries of the head, trunk and upper extremities: 1 - a. facialis; 2 - a. lingualis; 3 - a. thyroidea sup.; 4 - a. carotis communis sin.; 5 -a. subclavia sin.; 6 - a. axillaris; 7 - arcus aortae; £ - aorta ascendens; 9 -a. brachialis sin.; 10 - a. thoracica int.; 11 - aorta thoracica; 12 - aorta abdominalis; 13 - a. phrenica sin.; 14 - truncus coeliacus; 15 - a. mesenterica sup.; 16 - a. renalis sin.; 17 - a. testicular sin.; 18 - a. mesenterica inf.; 19 - a. ulnaris; 20 -a. interossea communis; 21 - a. radialis; 22 - a. interossea ant.; 23 - a. epigastrica inf.; 24 - arcus palmaris superficialis; 25 - arcus palmaris profundus; 26 - aa. digitales palmares communes; 27 - aa. digitales palmares propriae; 28 - aa. digitales dorsales; 29 - aa. metacarpeae dorsales; 30 - ramus carpeus dorsalis; 31 -a, profunda femoris; 32 - a. femoralis; 33 - a. interossea post.; 34 - a. iliaca externa dextra; 35 - a. iliaca interna dextra; 36 - a. sacraiis mediana; 37 - a. iliaca communis dextra; 38 - aa. lumbales; 39— a. renalis dextra; 40 - aa. intercostales post.; 41 -a. profunda brachii; 42 -a. brachialis dextra; 43 - truncus brachio-cephalicus; 44 - a. subciavia dextra; 45 - a. carotis communis dextra; 46 - a. carotis externa; 47 -a. carotis interna; 48 -a. vertebralis; 49 - a. occipitalis; 50 - a. temporalis superficialis.
Rice. 2. Arteries of the anterior surface of the leg and dorsum of the foot: 1 - a, genu descendens (ramus articularis); 2 - ram! musculares; 3 - a. dorsalis pedis; 4 - a. arcuata; 5 - ramus plantaris profundus; 5 -aa. digitales dorsales; 7 -aa. metatarseae dorsales; 8 - ramus perforans a. peroneae; 9 - a. tibialis ant.; 10 -a. recurrens tibialis ant.; 11 - rete patellae et rete articulare genu; 12 - a. genu sup. lateralis.
Rice. 3. Arteries of the popliteal fossa and posterior surface of the leg: 1 - a. poplitea; 2 - a. genu sup. lateralis; 3 - a. genu inf. lateralis; 4 - a. peronea (fibularis); 5 - rami malleolares tat.; 6 - rami calcanei (lat.); 7 - rami calcanei (med.); 8 - rami malleolares mediales; 9 - a. tibialis post.; 10 - a. genu inf. medialis; 11 - a. genu sup. medialis.
Rice. 4. Arteries of the plantar surface of the foot: 1 - a. tibialis post.; 2 - rete calcaneum; 3 - a. plantaris lat.; 4 - a. digitalis plantaris (V); 5 - arcus plantaris; 6 - aa. metatarseae plantares; 7 -aa. digitales propriae; 8 - a. digitalis plantaris (hallucis); 9 - a. plantaris medialis.
Rice. 5. Arteries of the abdominal cavity: 1 - a. phrenica sin.; 2 - a. gastrica sin.; 3 - truncus coeliacus; 4 -a. lienalis; 5 -a. mesenterica sup.; 6 - a. hepatica communis; 7 -a. gastroepiploica sin.; 8 - aa. jejunales; 9 -aa. ilei; 10 -a. colica sin.; 11 -a. mesenterica inf.; 12 -a. iliaca communis sin.; 13 -aa, sigmoideae; 14 - a. rectalis sup.; 15 - a. appendicis vermiformis; 16 -a. ileocolica; 17 -a. iliaca communis dextra; 18— a. colica. dext.; 19— a. pancreaticoduodenal inf.; 20— a. colica media; 21 - a. gastroepiploica dextra; 22 - a. gastroduodenalis; 23 - a. gastrica dextra; 24 - a. hepatica propria; 25 - a, cystica; 26 - aorta abdominalis.
Arteries (Greek arteria) are a system of blood vessels extending from the heart to all parts of the body and containing blood enriched with oxygen (the exception is a. pulmonalis, which carries venous blood from the heart to the lungs). The arterial system includes the aorta and all its branches down to the smallest arterioles (Fig. 1-5). Arteries are usually designated by topographical characteristics (a. facialis, a. poplitea) or by the name of the organ they supply (a. renalis, aa. cerebri). Arteries are cylindrical elastic tubes of various diameters and are divided into large, medium and small. The division of arteries into smaller branches occurs according to three main types (V.N. Shevkunenko).
With the main type of division, the main trunk is well defined, gradually decreasing in diameter as secondary branches move away from it. The loose type is characterized by a short main trunk that quickly breaks up into a mass of secondary branches. The transitional, or mixed, type occupies an intermediate position. The branches of the arteries often connect with each other, forming anastomoses. There are intrasystemic anastomoses (between the branches of one artery) and intersystemic anastomoses (between the branches of different arteries) (B. A. Dolgo-Saburov). Most anastomoses exist continuously as roundabout (collateral) blood circulation pathways. In some cases, collaterals may reappear. Small arteries can be directly connected to veins using arteriovenous anastomoses (see).
Arteries are derivatives of mesenchyme. During embryonic development, muscle, elastic elements and adventitia, also of mesenchymal origin, are added to the initial thin endothelial tubes. Histologically, three main membranes are distinguished in the artery wall: internal (tunica intima, s. interna), middle (tunica media, s. muscularis) and external (tunica adventitia, s. externa) (Fig. 1). According to their structural features, arteries are distinguished into muscular, muscular-elastic and elastic types.
Muscle-type arteries include small and medium-sized arteries, as well as most arteries of internal organs. The inner lining of the artery includes the endothelium, subendothelial layers and internal elastic membrane. The endothelium lines the lumen of the artery and consists of flat cells elongated along the axis of the vessel with an oval nucleus. The boundaries between cells have the appearance of a wavy or finely jagged line. According to electron microscopy, a very narrow (about 100 A) gap is constantly maintained between cells. Endothelial cells are characterized by the presence of a significant number of vesicle-like structures in the cytoplasm. The subendothelial layer consists of connective tissue with very thin elastic and collagen fibers and poorly differentiated stellate cells. The subendothelial layer is well developed in large and medium-sized arteries. The internal elastic, or fenestrated, membrane (membrana elastica interna, s.membrana fenestrata) has a lamellar-fibrillar structure with holes of various shapes and sizes and is closely connected with the elastic fibers of the subendothelial layer.
The tunica media consists mainly of smooth muscle cells, which are arranged in a spiral. Between the muscle cells there is a small amount of elastic and collagen fibers. In medium-sized arteries, at the border between the middle and outer membranes, elastic fibers can thicken, forming an outer elastic membrane (membrana elastica externa). The complex muscular-elastic framework of muscular-type arteries not only protects the vascular wall from overstretching and rupture and ensures its elastic properties, but also allows the arteries to actively change their lumen.
Arteries of the muscular-elastic, or mixed, type (for example, the carotid and subclavian arteries) have thicker walls with an increased content of elastic elements. Fenestrated elastic membranes appear in the middle shell. The thickness of the internal elastic membrane also increases. An additional internal layer appears in the adventitia, containing individual bundles of smooth muscle cells.
The arteries of the elastic type include the vessels of the largest caliber - the aorta (see) and the pulmonary artery (see). In them, the thickness of the vascular wall increases even more, especially the middle shell, where elastic elements predominate in the form of 40-50 powerfully developed fenestrated elastic membranes connected by elastic fibers (Fig. 2). The thickness of the subendothelial layer also increases, and in it, in addition to loose connective tissue rich in stellate cells (Langhans layer), individual smooth muscle cells appear. The structural features of elastic arteries correspond to their main functional purpose - predominantly passively resisting a strong push of blood ejected from the heart under high pressure. Different sections of the aorta, differing in their functional load, contain different amounts of elastic fibers. The arteriole wall retains a highly reduced three-layer structure. The arteries that supply blood to internal organs have specific structural features and intraorgan distribution of branches. The branches of the arteries of hollow organs (stomach, intestines) form a network in the wall of the organ. Arteries in parenchymal organs have a characteristic topography and a number of other features.
Histochemically, a significant amount of mucopolysaccharides is found in the ground substance of all arterial membranes and especially in the inner membrane. The walls of the arteries have their own blood vessels supplying them (a. and v. vasorum, s. vasa vasorum). Vasa vasorum are located in the adventitia. Nutrition of the inner membrane and the part of the middle membrane bordering it is carried out from blood plasma through the endothelium by pinocytosis. Using electron microscopy, it was established that numerous processes extending from the basal surface of endothelial cells reach muscle cells through holes in the internal elastic membrane. When the artery contracts, many small and medium-sized windows in the internal elastic membrane are partially or completely closed, which makes it difficult for nutrients to flow through the processes of endothelial cells to muscle cells. Great importance in the nutrition of areas of the vascular wall lacking vasa vasorum is attached to the ground substance.
Motor and sensory innervation of the arteries is carried out by sympathetic, parasympathetic nerves and branches of the cranial or spinal nerves. The nerves of the arteries, forming plexuses in the adventitia, penetrate the tunica media and are designated as vasomotor nerves (vasomotors), which contract the muscle fibers of the vascular wall and narrow the lumen of the artery. The walls of the artery are equipped with numerous sensitive nerve endings - angioreceptors. In certain areas of the vascular system there are especially many of them and they form reflexogenic zones, for example, at the site of division of the common carotid artery in the area of the carotid sinus. The thickness of the artery walls and their structure are subject to significant individual and age-related changes. And arteries have a high ability to regenerate.
Pathology of the arteries - see Aneurysm, Aortitis, Arteritis, Atherosclerosis, Coronary artery disease, Coronary sclerosis, Endarteritis.
See also Blood vessels.
Carotid artery
Rice. 1. Arcus aortae and its branches: 1 - mm. stylohyoldeus, sternohyoideus et omohyoideus; 2 and 22 - a. carotis int.; 3 and 23 - a. carotis ext.; 4 - m. cricothyreoldeus; 5 and 24 - aa. thyreoideae superiores sin. et dext.; 6 - glandula thyreoidea; 7 - truncus thyreocervicalis; 8 - trachea; 9 - a. thyreoidea ima; 10 and 18 - a. subclavia sin. et dext.; 11 and 21 - a. carotis communis sin. et dext.; 12 - truncus pulmonaiis; 13 - auricula dext.; 14 — pulmo dext.; 15 - arcus aortae; 16 - v. cava sup.; 17 - truncus brachiocephalicus; 19 – m. scalenus ant.; 20 - plexus brachialis; 25 - glandula submandibularis.
Rice. 2. Arteria carotis communis dextra and its branches; 1 - a. facialis; 2 - a. occipitalis; 3 - a. lingualis; 4 - a. thyroidea sup.; 5 - a. thyreoidea inf.; 6 -a. carotis communis; 7 - truncus thyreocervicalis; 8 and 10 - a. subclavia; 9 - a. thoracica int.; 11 - plexus brachialis; 12 - a. transversa colli; 13 - a. cervicalis superficialis; 14 - a. cervicalis ascendens; 15 -a. carotis ext.; 16 - a. carotis int.; 17 - a. vagus; 18 - n. hypoglossus; 19 - a. auricularis post.; 20 - a. temporalis superficialis; 21 - a. zygomaticoorbitalis.
Rice. 1. Transverse section of the artery: 1 - outer membrane with longitudinal bundles of muscle fibers 2, 3 - middle membrane; 4 - endothelium; 5 - internal elastic membrane.
Rice. 2. Transverse section of the thoracic aorta. The elastic membranes of the middle shell are contracted (o) and relaxed (b). 1 - endothelium; 2 - intima; 3 - internal elastic membrane; 4 - elastic membranes of the middle shell.
Main arteries
The great vessels are those human arteries whose anatomy is of critical importance for surgery. These include large vessels of elastic and transitional type: aorta, iliac, renal arteries, subclavian and carotid. They are called trunk for the reason that they deliver blood not to the organs, but to areas of the body. For example, the aorta, as the largest vessel, carries blood to all parts of the body.
The carotid arteries, the anatomy of which will be discussed below, deliver nutrients and oxygen to the head and brain. The great vessels also include the femoral, brachial arteries, celiac trunk, mesenteric vessels and many others. This concept not only defines the context for studying the anatomy of arteries, but is intended to clarify the regions of blood supply. This makes it possible to understand that blood is delivered from the heart through large to small arteries and in the huge area where the great vessels are present, neither gas exchange nor exchange of metabolites is possible. They perform only a transport function and participate in hemostasis.
Arteries of the neck and head
The arteries of the head and neck, the anatomy of which allows us to understand the nature of vascular lesions of the brain, originate from the aortic arch and subclavian vessels. The most significant is the pool of the carotid arteries (right and left), through which the largest amount of oxygenated blood enters the tissues of the head.
The right common carotid (carotid) artery branches from the brachiocephalic trunk, which originates on the aortic arch. To the left is a branch of the left common carotid and left subclavian arteries.
Arteries in children
The fetal circulatory system is placental, that is, the child receives oxygen and nutrients not through the lungs (pulmonary circulation), but through the mother’s arterial blood, which reaches him through the umbilical vein.
At birth, the baby’s lungs open, and the cardiovascular system switches to pulmonary circulation - a small circle starts. In this case, the umbilical arteries are completely overgrown during the first days of life.
Also, immediately after birth, changes occur in the heart; the fetus has an oval window - an opening that connects the right and left atria and allows blood to flow bypassing the lungs. After the first inhalation, the hole normally closes with a valve, and within the first 1-2 years it closes completely.
If the oval window does not close, it can cause diseases, since it will interfere with the functioning of the pulmonary circulation and contribute to the mixing of arterial and venous blood. However, in most cases, even those people who live with an open oval window all their lives do not experience any special health problems.
Serious pathologies of vascular development can also appear in childhood. Among them:
- Aneurysms (weakening of the walls of a vessel, as a result of which it locally increases in diameter).
- Arterial stenosis (narrowing of the diameter of the artery).
- Arterial hypoplasia (underdevelopment of the vessel tube).
Blood supply to the brain
Both carotid arteries are divided into two large branches - the external and internal carotid arteries. The anatomy of these vessels is notable for the multiple anastomoses between the branches of these basins in the area of the facial skull.
The external carotid arteries are responsible for supplying blood to the muscles and skin of the face, tongue, and larynx, while the internal ones are responsible for supplying blood to the brain. Inside the skull there is an additional source of blood supply - the basin of the vertebral arteries (anatomy has thus provided a reserve source of blood supply). They originate from the subclavian vessels, after which they head upward and enter the cranial cavity.
Then they merge and form an anastomosis between the arteries of the internal carotid artery, creating the Willis circle of blood circulation in the brain. After the vertebral and internal carotid territories of the carotid arteries are united, the anatomy of the blood supply to the brain becomes more complicated. This is a backup mechanism that protects the main organ of the nervous system from most ischemic episodes.
Arteries of the upper limbs
The upper limb girdle is fed by a group of arteries that originate from the aorta. To the right of it the brachiocephalic trunk branches off, giving rise to the right subclavian artery. The anatomy of the blood supply to the left limb is slightly different: the subclavian artery on the left is separated directly from the aorta, and not from the trunk common with the carotid arteries. Because of this feature, a special symptom may be observed: with significant hypertrophy of the left atrium or severe stretching, it presses on the subclavian artery, causing its pulsation to weaken.
From the subclavian arteries, after originating from the aorta or the right brachiocephalic trunk, a group of vessels later branches off to the free upper limb and the shoulder joint.
The largest arteries in the arm are the brachial and ulnar arteries, which for a long time run together with the nerves and veins in the same channel. True, this description is very inaccurate, and the location varies from person to person. Therefore, the course of blood vessels should be studied on a macroscopic specimen, using diagrams or anatomical atlases.
Pathological anatomy of heart valves
A wide range of pathologies that can change the normal anatomy of the two atrioventricular and vascular valves is headed by acute rheumatic fever:
- connective tissue diseases;
- injuries;
- infective endocarditis;
- congenital malformations;
- pathology of other organs and systems.
View of an open and closed normal and modified valve.
| Valve pathology | Hemodynamic changes | Images characterizing pathology |
| Mitral stenosis | The narrowing of the bicuspid valve area makes it impossible to completely empty the left atrium during diastole. Excessive stretching of its cavity, a significant decrease in the stroke volume of the left ventricle and stagnation in the pulmonary circulation, in addition to a number of characteristic clinics, also ensures the development of concomitant pathology, for example, atrial fibrillation. |
|
| Mitral regurgitation | The reverse flow of blood from the ventricle into the atrium entails an increase in the volume circulating in the left chambers of the heart. The explanation for this is simple: in diastole, in addition to oxygenated blood returning from the pulmonary veins, the ventricle also receives the volume of blood that returned through the mitral valve to the left atrium in the previous systole. |
|
| Left atrioventricular valve stenosis | Due to the similarity in the structure of the two atrioventricular valves, the pathophysiology accompanying their stenosis will be similar to one another, with the exception of the affected side of the heart, and accordingly, the circulatory system. In this case, the right atrium is susceptible to overstretching of the cavity, and stagnation is observed in a large circle. The small circle suffers from depletion of blood flow through it. |
|
| Tricuspid valve insufficiency | The right ventricle receives a volume of blood that exceeds the norm, since in diastole it is replenished with a portion coming from the vena cava, as well as with a portion of regurgitation. |
|
| Stenosis of the aortic and pulmonary valves | An increase in afterload due to a narrowing of the lumen of the aortic and pulmonary valves leads to an increase in the force of contraction necessary to “push” the stroke volume of blood into the pulmonary and systemic circulation. The long course of this pathology, in addition to the depletion of the corresponding affected circle, leads to the development and increase of heart failure. |
|
| Aortic and pulmonary valve insufficiency | Reversed blood flow due to insufficient closure of the semilunar valves or dilatation of the aortic orifice or pulmonary trunk leads to an increase in the stroke volume of the right or left ventricle, as well as reduced perfusion of the pulmonary or systemic circulation (depending on the affected valve). |
|
In conclusion, it is important to note that regular optimal physical activity allows you to train the heart muscle, which plays an important role in preventing the development of a large list of pathologies. Thus, the price of a healthy lifestyle in youth is equal to its quality in old age.
Arterial bed of the abdominal cavity
In the abdominal cavity, the blood supply is also of the main type. The celiac trunk and several mesenteric arteries branch off from the aorta. From the celiac trunk branches go to the stomach, pancreas, and liver. To the spleen, the artery sometimes branches off from the left gastric, and sometimes from the right gastroduodenal. These features of blood supply are individual and variable.
In the retroperitoneal space there are two kidneys, to each of which two short renal vessels are directed. The left renal artery is much shorter and less often affected by atherosclerosis. Both of these vessels are capable of withstanding high pressure, and a quarter of each systolic ejection of the left ventricle flows through them. This proves the fundamental importance of the kidneys as organs regulating blood pressure.
Pelvic arteries
The pelvic cavity includes the aorta, which is divided into two large branches - the common iliac arteries. The right and left external and internal iliac vessels depart from them, each of which is responsible for the blood circulation of its parts of the body. The external iliac artery gives off a number of small branches and goes to the lower limb. From now on, its continuation will be called the femoral artery.
The internal iliac arteries give many branches to the genitals and bladder, the muscles of the perineum and rectum, as well as the sacrum.
Embryology
Rice.
4. Arteries of the plantar surface of the foot: 1 - a. tibialis post.; 2 - rete calcaneum; 3 - a. plantaris lat.; 4 - a. digitalis plantaris (V); 5 - arcus plantaris; 6 - aa. metatarseae plantares; 7 - aa. digitales propriae; 8 - a. digitalis plantaris (hallucis); 9 - a. plantaris medialis. Rice. 5. Arteries of the abdominal cavity: 1 - a. phrenica inferior sin.; 2 - a. gastrica sin.; 3 - truncus celiacus; 4 - a. lienalis; 5 - a. mesenterica sup.; 6 - a. hepatica communis; 7 - a. gastroepiploica sin.; 8 - aa. jejunales; 9 - aa. ilei; 10 - a. colica sin.; 11 - a. mesenterica inf.; 12 a.m. iliaca communis sin.; 13 - sigmoideae; 14_a. rectalis sup.; 15 - a. appendicularis; 16 - a. ileocolica; 17 - a. iliaca communis dext.; 18 - a. colica dext.; 19 - a. pancreaticoduodenalis inf.; 20—n. colica media; 21 - a. gastroepiploica dext.; 22 - a. gastroduodenalis; 23 - a. gastrica dext.; 24 - a. hepatica propria; 25 - a. cystica; 26 - aorta abdominalis. Arteries develop from mesenchyme. In vertebrate and human embryos, an arterial trunk departs from the heart, which, heading to the head section of the embryo, soon divides into two ventral aortas. The last six arterial branchial arches are connected with the dorsal aortas (see Aorta, comparative anatomy). A series of paired arterial vessels depart from the dorsal aortas, running along the sides of the neural tube in the dorsal direction between the somites (dorsal intersegmental arteries). In addition to them, two other types of paired arteries depart from the aorta of the embryo: the lateral segmental arteries and the ventral segmental arteries. From the arterial trunk the ascending aorta (aorta ascendens) and pulmonary trunk (truncus pulmonalis) develop; the initial sections of the ventral and dorsal aortas, connected by 6 arterial branchial arches, give rise to the internal, external and common carotid arteries (aa. carotis interna, externa et communis), on the right the brachiocephalic trunk and the subclavian artery (tra arteries uncus brachiocephalicus and a. subclavia dext .), on the left - the aortic arch (arcus aortae), pulmonary arteries (aa. pulmonales) and the ductus arteriosus (ductus arteriosus). From the dorsal intersegmental arteries the vertebral arteries (aa. vertebrales) are formed, and more cranially - the basilar artery (a. basilaris) and its branches. Caudal to the level of emergence of the vertebral arteries, intercostal and lumbar arteries (aa. intercostales post, et aa. lumbales) are formed from the dorsal intersegmental arteries. Numerous anastomoses of these vessels form the internal thoracic artery (a. thoracica int.) and the upper and lower epigastric arteries (aa. epigastricae sup. et inf). The lateral segmental arteries are associated with the developing genitourinary organs. In embryos at early stages of development, the branches of the lateral segmental arteries form the glomeruli of the primary kidney tubules (mesonephros). From the lateral segmental arteries, the renal, adrenal arteries and arteries of the gonads develop (aa. renales, aa. suprarenales et aa. testiculares, s. ovaricae). The ventral segmental arteries are associated with the yolk sac and intestinal tract. In embryos of early stages of development, they are directed laterally along the dorsal wall of the primary intestine, and from here into the walls of the yolk sac, constituting the arterial part of the yolk circulation of the embryo. Later, when the intestine separates from the yolk sac and the mesentery appears, the paired ventral segmental arteries unite and form arteries located in the mesentery (color Fig. 1): the celiac trunk (truncus celiacus), the superior and inferior mesenteric arteries (aa. mesentericae sup. et inf.). In the caudal section, the umbilical arteries (aa. umbilicales) develop from the ventral segmental arteries. During the development of the upper extremities, the axial artery grows into them as a continuation of the subclavian artery, the remainder of which in the forearm region is the interosseous artery (a. interossea communis). The vessels of the developing hand are connected to the axial artery. In later stages of development, the connection with this artery disappears and the median artery develops parallel to it. The radial and ulnar arteries (aa. radialis et ulnaris) develop as branches of the axial artery. The primary artery of the leg, like that of the arm, is axial, arises from the initial section of the umbilical artery and is called the sciatic artery. At later stages of development, it loses its importance, and only the peroneal artery (a. peronea) and a number of small arteries of the lower limb remain from it, and the external iliac artery (a. iliaca externa) receives significant development, and its continuation is the femoral, popliteal and the posterior tibial artery (a. femoralis, a. poplitea et tibialis post.) constitute the main arterial trunk of the leg. After birth, with the cessation of placental blood circulation, the proximal parts of the umbilical arteries form the internal iliac arteries (aa. iliacae int.), and the umbilical artery itself is reduced and turns into the medial umbilical ligament (lig. umbilicale mediale).
Arteries of the lower extremities
The arteries of the lower extremities have a simpler anatomy than the pelvic vessels, due to a more pronounced blood supply. In particular, the femoral artery, branching from the external iliac, descends and gives off many branches to supply blood to the muscles, bones and skin of the lower extremities.
On its way, it gives off a large descending branch, the popliteal, anterior and posterior tibial, and fibular branches. On the foot, branches already extend from the tibial and peroneal arteries to the ankles and ankle joints, heel bones, foot muscles and toes.
The blood circulation pattern of the lower extremities is symmetrical - the vessels are the same on both sides.
Arterial diseases
Arterial diseases can be divided into congenital and acquired. Congenital defects are often diagnosed at an early age (before 3-5 years) or immediately after birth.
Acquired ones develop over the years and can be the result of diseases, heredity or lifestyle. For example, arterial blood flow may be impaired due to diabetes mellitus, which worsens the composition of arterial blood, or may occur after vascular injury.
Other reasons for the development of diseases may be bad habits and poor lifestyle:
- Smoking increases the risk of atherosclerosis.
- Excess salt in the diet disrupts the water-salt balance and affects blood pressure.
- Too much fatty food increases the level of “bad” cholesterol in the blood and contributes to the formation of atherosclerotic plaques.
- Excess body weight can affect the condition of the arteries of the limbs and other vessels.
Arterial hypoplasia
Arterial hypoplasia is a congenital malformation of blood vessels, which is characterized by underdevelopment of a certain area of the artery, resulting in a narrowing of the lumen and deterioration of blood flow. The severity of the symptoms of the disease depends on which vessel is affected. For example, hypoplasia of the aortic artery manifests itself already in the first day of life, as soon as the ductus arteriosus begins to overgrow. The baby has:
- Tachycardia with weak pulse.
- Paleness of the skin.
- Dyspnea.
- Breathing problems, in particular, may include sleep apnea.
Hypoplasia of the vertebral artery may not appear for a long time. This defect is characterized by signs of oxygen starvation of the brain:
- Weakness.
- Drowsiness.
- Irritability.
- Deterioration of vision.
- Darkening of the eyes, dizziness.
- Infants may experience delayed mental development.
Arterial hypoplasia is a risk factor for the development of organ infarctions, because a narrow area can easily be blocked by a blood clot.
Pathology most often develops for the following reasons:
- Drinking and smoking during pregnancy.
- Bruise during pregnancy.
- Infectious diseases. Flu, rubella, and acute toxoplasmosis are especially dangerous.
To completely eliminate the pathology, surgical treatment is performed.
Artery aneurysm
An aneurysm is a stretching of the vessel wall, most often found in arteries. It is formed due to congenital or acquired defects in the middle part of the artery wall. As a result, the pulsating blood puts pressure on the weak area and stretches it.
The severity of the symptoms of an aneurysm and its danger depend on the site of the lesion.
With pathology of the arteries of the brain, the aneurysm may not make itself felt until the weakened area bursts and causes a hemorrhagic stroke (hemorrhage). If the aneurysm grows but does not burst, its symptoms are similar to a brain tumor - headaches, blurred vision, nausea, etc.
A coronary artery aneurysm can occur after a myocardial infarction and is manifested by heart failure: weakness, edema, etc.
Dilatation of the walls of the aorta may be asymptomatic until the diameter of the artery exceeds 7 cm. In other cases, a person may feel pain, pulsation in the abdomen, coldness in the toes and hands. Aortic rupture causes massive bleeding and is fatal in most cases.
Arterial stenosis
Arterial stenosis is a dangerous condition characterized by a decrease in the lumen of the vessel, with subsequent disruption of blood flow. It occurs as a consequence of other diseases - diabetes, atherosclerosis, arterial hypertension. The main reason is the accumulation of cholesterol plaques on the walls of blood vessels. However, the condition can also be a congenital pathology. Unlike arterial hypoplasia, which is characterized by underdevelopment of the wall, a vessel affected by stenosis may appear normal in appearance.
Arterial stenosis can appear in any part of the arterial system.
- Damage to cerebral vessels.
It is characterized by a gradual deterioration in blood circulation, which manifests itself in memory impairment, changes in the emotional sphere, and movement disorders may occur. The most dangerous consequence is ischemic stroke.
- Stenosis of the arteries of the lower extremities.
Impaired blood flow in the legs can lead to dangerous consequences, including the development of trophic ulcers and gangrene. The so-called “diabetic foot” is typical for patients with type 2 diabetes mellitus.
- Stenosis of the coronary arteries.
The main symptom of coronary heart disease, the risk of developing heart failure and myocardial infarction.
- Pulmonary stenosis
A congenital pathology in which there is a decrease in the diameter of the pulmonary duct or the vessels themselves. Very often combined with other heart defects.
Arterial hypertension and blood pressure
Blood moves through the arteries under a certain pressure. There are two types of it:
- Systolic (upper) occurs when the heart muscle contracts.
- Diastolic (lower) occurs when the heart relaxes.
Normally, in an adult, these indicators should be 120/80 mm Hg. Art. However, during physical activity or emotional experiences, blood pressure can increase - this is facilitated by the release of hormones into the blood, an increase in muscle needs for oxygen and other factors. In a healthy person, blood pressure should return to normal a short time after the cause is eliminated.
If blood pressure readings are constantly above normal, often observed in a calm state, the person is diagnosed with arterial hypertension (hypertension). This is a common CVD disease, occurring in 50-65% of people over 65 years of age and in 20-30% of the adult population.
There are several degrees of hypertension:
- 1st degree – 140-159/90-99 mmHg. Art.
- 2nd degree – 169-179/100-109 mm Hg. Art.
- 3rd degree – 180 and above/110 and above mmHg. Art.
Increased arterial blood flow affects the functioning of the cardiovascular system, even if the patient is accustomed to high blood pressure values. Hypertension increases the risk of developing the following diseases and conditions:
- Myocardial infarction.
- Stroke.
- Heart failure.
- Visual impairment.
- Kidney failure.
Atherosclerosis of the arteries
Atherosclerosis of the arteries is one of the most common diseases of the cardiovascular system; its varying degrees are recorded in every second person over 50 years of age. With age, the metabolism of fats and proteins is disrupted, as a result of which plaques - cholesterol deposits - begin to form on the walls of the arteries.
Atherosclerosis of the arteries is a chronic disease, and it does not manifest any symptoms for a long time. And this is its main danger, since in advanced stages, when the lumen of blood vessels is severely blocked, the disease causes serious consequences. Atherosclerosis of the arteries can be localized in a specific area of the body, but, as a rule, affects the entire arterial system.
Since plaques make the vessels less elastic, in atherosclerosis the danger is not only the deposits themselves, but also the blood clots that form in areas of microdamage to the walls. Most often, it is the combination of a cholesterol plaque and a blood clot that leads to organ infarctions.
Cardiac ischemia
Coronary heart disease is a special case of atherosclerosis, which affects the coronary arteries. The disease develops over years and does not make itself felt in the early stages. The asymptomatic, or “silent” form of IHD can last up to 5 years or more. Afterwards, the patient exhibits heart rhythm disturbances, angina pectoris, signs of insufficient oxygen supply to the heart muscle: fatigue, shortness of breath, etc.
IHD is a chronic diagnosis, a disease that gradually progresses. The best results in stopping atherosclerotic degeneration of the coronary arteries are obtained by treatment in the early stages. But since at this time the disease does not make itself felt, preventive appointments with a cardiologist are key in its diagnosis. They are recommended for men every year starting at age 40, and for women no later than age 50.
Myocardial infarction
The final stage of coronary artery disease is myocardial infarction, in which an atherosclerotic plaque, often with an attached thrombus, completely blocks the artery. Depending on how large a section of the coronary vessel cannot deliver arterial blood, a different section of the heart muscle dies.
A heart attack is manifested by characteristic severe pain, which:
- It cannot be relieved by taking nitroglycerin tablets (three tablets in a row with five-minute intervals).
- Does not go away with rest or in the fresh air.
- It can radiate to the arm, back, shoulder, neck, jaw.
Myocardial infarction requires immediate medical attention, preferably from a specialized cardiac team that can carry out the first manipulations on the way to the hospital. It must be remembered that this is a potentially fatal condition, so an ambulance should be called even if an attack is suspected. If the patient survives, a scar forms on the affected area of the myocardium, which leads to disability.
Thromboembolism of arteries
Arterial thromboembolism is a blockage of a vessel by a thrombus, as a result of which blood flow stops and ischemia develops. Special cases are myocardial infarction, renal infarction, ischemic stroke.
Separately, cardiologists distinguish pulmonary embolism (PE). In this condition, blood clots block the vessel itself or its branches. Since the diameter of the pulmonary artery is quite large (up to 2.5 cm), the condition is most often caused by large blood clots that form in the veins of the lower extremities, from there they enter the heart and then clog the lumen.
This type of arterial thromboembolism is a fairly common acute condition, occurring on average in 1 in 1000 patients. Older people are most often affected; among men, pulmonary embolism is 20-30% more common than among women. In some cases, blockage of the pulmonary artery is caused not by blood clots, but by air or fat bubbles, tumor cells, and foreign bodies. However, among all the possible causes, blood clots are the main ones.