Topography of the inferior and superior vena cava
The superior vena cava (SVC) is a short trunk located in the chest to the right of the ascending aorta. It is 5-8 cm long, 21-28 mm in diameter. This is a thin-walled vessel that has no valves and is located in the upper part of the anterior mediastinum. It is formed from the confluence of two brachiocephalic veins behind the first sternocostal joint on the right.
Further, descending, at the level of the cartilage of the third rib, the vein flows into the right atrium. Topographically, the pleural layer with the phrenic nerve is adjacent to the superior vena cava on the right, the ascending aorta is on the left, the thymus is in front, and the root of the right lung is behind. The lower part of the SVC is located in the pericardial cavity. The only tributary vessel is the azygos vein.
Tributaries of the ERW:
- brachiocephalic veins;
- steam room and nameless;
- intercostal;
- veins of the spinal column;
- internal jugular;
- plexuses of the head and neck;
- sinuses of the dura mater of the brain;
- emissary vessels;
- veins of the brain.
The SVC system collects blood from the head, neck, upper extremities, organs, and chest walls.
The inferior vena cava (IVC) is the largest venous vessel in the human body (18-20 cm long and 2-3.3 cm in diameter), which collects blood from the lower extremities, pelvic organs and abdominal cavity. It also does not have a valve system and is located extraperitoneally.
The IVC begins at the level of the IV-V lumbar vertebrae and is formed by the confluence of the left and right common iliac veins. Then it follows upward, frontally in relation to the right psoas major muscle, the lateral part of the vertebral bodies, and above, in front of the right leg of the diaphragm, it lies next to the abdominal aorta. The vessel enters the chest cavity through the tendon opening of the diaphragm into the posterior, then upper mediastinum and flows into the right atrium.
The IVC system is one of the most powerful collectors in the human body (it provides 70% of the total venous blood flow).
Tributaries of the inferior vena cava:
- Parietal: Lumbar veins.
- Lower diaphragmatic.
- Two ovarian veins.
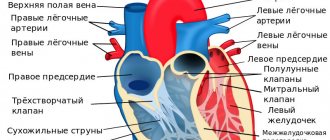
Anatomy of the venous apparatus of the heart: how does it all work?
Veins carry blood from organs to the right atrium (the exception is the pulmonary veins, which transport it to the left atrium).
Histological structure of the wall of a venous vessel:
- internal (intima) with venous valves;
- elastic membrane (media), which consists of circular bundles of smooth muscle fibers;
- external (adventitia).
The IVC refers to veins of the muscular type, in which the outer membrane contains well-developed bundles of longitudinally arranged smooth muscle cells.
In the SVC, the degree of development of muscular elements is moderate (sparse groups of longitudinally located fibers in the adventitia).
Veins have many anastomoses and form plexuses in organs, which ensures their greater capacity compared to arteries. They have high stretchability and relatively low elasticity. The blood moves through them against the force of gravity. Most veins have valves on their inner surfaces that prevent backflow.
The movement of blood through the vena cava into the heart is ensured by:
- negative pressure in the chest cavity and its fluctuation during breathing;
- suction ability of the heart;
- the work of the diaphragmatic pump (its pressure on the internal organs during inhalation pushes blood into the portal vein);
- peristaltic contractions of their walls (with a frequency of 2-3 per minute).
How does the syndrome manifest?
Symptoms of the syndrome can occur suddenly, without any provoking factors or precursors. This can occur at a time when the superior vena cava is tightly blocked by an atherosclerotic thrombus.
In most cases, the syndrome is characterized by the following symptoms:
- cough with increasing shortness of breath;
- attacks of headache and dizziness;
- pain localized in the chest area;
- dysphagia and nausea;
- changes in facial expressions and features;
- fainting conditions;
- noticeable swelling of veins in the cervical area and within the chest;
- swelling and puffiness of the face;
- cyanosis of the facial area or chest.
For the most accurate diagnosis of superior vena cava syndrome, it is necessary to undergo a series of procedures aimed at examining the condition of the venous channels. Such examinations include topography, radiography and Doppler ultrasound. By resorting to their help, it is quite possible to differentiate diagnoses and prescribe the most effective surgical treatment.
If your general health worsens or the above symptoms are detected, you should immediately contact a medical institution for qualified advice. Only an experienced specialist will be able to most accurately and quickly establish a diagnosis, as well as suggest suitable treatment measures.
If thrombosis of the superior vena cava is not detected in time, deplorable health conditions can occur.
Vessels
Brachiocephalic Vein (Left): From Which Veins Is Formed?
Feb 06, 2020 Kokh V. A.
7196
Vessels
Arteries of the Head and Neck: Anatomy, Diagram, Atherosclerosis
Feb 06, 2020 Kokh V. A.
16582
Vessels
Vascular function
Veins, together with arteries, capillaries and the heart, form a single circulatory system. Unidirectional continuous movement through the vessels is ensured by the pressure difference in each segment of the channel.
Main functions of veins:
- deposition (reserve) of circulating blood (2/3 of the total volume);
- return of oxygen-depleted blood to the heart;
- saturation of tissues with carbon dioxide;
- regulation of peripheral circulation (arteriovenous anastomoses).
Syndrome and pregnancy
During the period of gestation, all the woman’s organs experience a heavy load, the volume of circulating blood increases and, as a result, stagnation appears. The uterus enlarges and compresses not only surrounding organs, but also blood vessels. In case of inferior vena cava syndrome in pregnant women, treatment should be carried out with extreme caution.
Problems begin with the fact that it is very difficult for a woman to lie on her back; usually this condition begins from the 25th week of gestation. There is slight dizziness, weakness, periodically lack of air. Blood pressure usually decreases. Very rarely, a pregnant woman may lose consciousness.
Naturally, we are not talking about drastic therapeutic measures during pregnancy, but some rules will still help to tolerate the syndrome easier:
- you will have to give up all exercises that are performed in a supine position, on your back;
— you should also not sleep on your back;
- nutrition should be adjusted towards reducing salt consumption;
- it is necessary to reduce the amount of fluid consumed;
- to improve the condition, it is better to walk more, in this case the muscles on the lower leg contract, and this process stimulates the upward movement of venous blood;
— a visit to the pool is recommended; the water helps squeeze blood out of the veins of the lower extremities.
What symptoms bother the patient when blood flow through the vena cava is disrupted?
The main pathology of the caval veins is their complete or partial obstruction (occlusion). Violation of the outflow of blood through these vessels leads to an increase in pressure in the vessels, then in the organs from which adequate outflow is not produced, their expansion, transudation (release) of fluid into the surrounding tissues and a decrease in the return of blood to the heart.
The main signs of impaired outflow through the vena cava:
- swelling;
- change in skin color;
- expansion of subcutaneous anastomoses;
- decreased blood pressure;
- dysfunction of organs from which there is no outflow.
Superior vena cava syndrome in men
This pathology is more common between the ages of 30 and 60 years (3-4 times more often in men).
Factors that provoke the formation of cava syndrome:
- extravasal compression (squeezing from the outside);
- tumor growth;
- thrombosis.
Causes of impaired patency of the SVC:
- Oncological diseases (lymphoma, lung cancer, breast cancer with metastasis, melanoma, sarcoma, lymphogranulomatosis).
- Aortic aneurysm.
- Enlarged thyroid gland.
- Infectious lesions of the vessel - syphilis, tuberculosis, histioplasmosis.
- Idiopathic fibrous mediastinitis.
- Constrictive endocarditis.
- Complication of radiation therapy (adhesions).
- Silicosis.
- Iatrogenic damage - blockage due to prolonged catheterization or a pacemaker.
Symptoms of SVC occlusion:
- severe shortness of breath;
- chest pain;
- cough;
- attacks of suffocation;
- hoarseness of voice;
- swelling of the veins of the chest, upper limbs and neck;
- puffiness, pastiness of the face, swelling of the upper extremities;
- cyanosis or congestion of the upper half of the chest and face;
- difficulty swallowing, swelling of the larynx;
- nosebleeds;
- headache, tinnitus;
- decreased vision, exophthalmos, increased intraocular pressure, drowsiness, convulsions.
Inferior vena cava syndrome in pregnant women
During the period of bearing a child, the constantly enlarging uterus in the supine position puts pressure on the inferior vena cava and abdominal aorta, which can lead to a number of unpleasant symptoms and complications.
The situation is further aggravated by an increase in the volume of circulating blood necessary to nourish the fetus.
Hidden manifestations of IVC syndrome are observed in more than 50% of pregnant women, and clinically in every tenth (severe cases occur with a frequency of 1:100).
As a result of compression of blood vessels, the following is observed:
- decreased venous return of blood to the heart;
- deterioration of blood oxygen saturation;
- decreased cardiac output;
- venous congestion in the veins of the lower extremities;
- high risk of thrombosis, embolism.
Symptoms of aortocaval compression (occur in the supine position, more often in the third trimester):
- dizziness, general weakness and fainting (due to a drop in blood pressure below 80 mm Hg);
- feeling of lack of oxygen, darkening of the eyes, tinnitus;
- severe pallor;
- heartbeat;
- nausea;
- cold clammy sweat;
- swelling of the lower extremities, manifestation of the vascular network;
- haemorrhoids.
This condition does not require drug treatment. A pregnant woman must follow a number of rules:
- do not lie on your back after 25 weeks of pregnancy;
- do not perform exercises in a lying position;
- rest on your left side or half-sitting;
- use special pillows for pregnant women during sleep;
- walk, swim in the pool;
- during childbirth, choose a position on your side or squatting.
Thrombosis
Blockage of the superior vena cava by a thrombus is often a secondary process caused by tumor growth in the lungs and mediastinum, a consequence of mastectomy, catheterization of the subclavian or jugular veins (with the exception of Paget-Schrötter syndrome).
In the case of complete occlusion of the lumen, the following rapidly occurs:
- cyanosis and swelling of the upper body, head and neck;
- inability to assume a horizontal position;
- severe headache and chest pain, aggravated by bending the body forward.
Causes of thrombosis of the inferior vena cava:
- Primary: Tumor process.
- Birth defects.
- Mechanical damage.
- Invasion of the vessel wall by a tumor.
Clinically, the following types of IVC thrombosis are distinguished:
- Distal segment (most common location). Symptoms are less pronounced due to the good compensatory capabilities of collateral blood flow. The patient develops signs of ileofemoral thrombosis - increasing swelling of the ankles, spreading to the entire limb, lower abdomen and lower back, cyanosis, bursting sensations in the legs.
- Renal segment. It is severe, has a high mortality rate and requires surgical correction. Clinically manifested as severe pain in the lower back, oliguria, the presence of protein in the urine, microhematuria, vomiting, and increasing renal failure.
- Liver segment. The clinic of suprahepatic portal hypertension is developing: an increase in the size of the organ, jaundice, ascites, the manifestation of venous plexuses on the anterior surface of the abdomen, varicose veins of the lower third of the esophagus (with the risk of gastrointestinal bleeding), splenomegaly.
Deep vein thrombosis. Treatment tactics in special cases
Surgical treatment The objectives of surgical intervention for DVT are to prevent pulmonary embolism and/or restore the patency of the venous bed. The choice of the scope of surgical treatment should be based on the localization of thrombosis, its prevalence, duration of the disease, the presence of concomitant pathology, the severity of the patient’s condition, and the technical and instrumental support available to the surgeon. Implantation of a vena cava filter.
Indications for implantation of a vena cava filter are:
• inability to provide appropriate anticoagulant therapy; • ineffectiveness of adequate anticoagulant therapy, against the background of which thrombosis increases with the formation of an embolic thrombus; • widespread embolic thrombosis; • recurrent pulmonary embolism with high (>50 mmHg) pulmonary hypertension. In young patients with removable risk factors and causes of DVT, it is necessary to implant only removable models, which should be removed when the threat of pulmonary embolism is eliminated. Endovascular catheter thrombectomy of the inferior vena cava and iliac veins. Indicated for embolic thrombi in the intra- and suprarenal sections of the inferior vena cava. Plication of the inferior vena cava.
Indications for plication of the inferior vena cava may include: • embolic thrombus of the suprarenal portion of the inferior vena cava in the absence of the ability to perform endovascular thrombectomy (plication is performed after direct thrombectomy); • INCORRECT POSITION of a previously INSTALLED vena cava filter (for example, its location in the renal vein), excluding the possibility of re-implantation (plication is performed after removal of the vena cava filter); • combination of embolic thrombosis with an operable tumor of the abdominal cavity or retroperitoneal space. In the long-term period, the patency of the inferior vena cava is completely restored in more than 2/3 of patients within 2-3 years after surgery. Palliative thrombectomy is indicated for embolic floating thrombosis of the femoral or iliac veins when it is inappropriate or impossible to install a vena cava filter. As a rule, it is supplemented by ligation or plication of the main vein. Radical thrombectomy. May be considered in cases of early diagnosed segmental venous thrombosis during the first 5 days of the disease. Given the difficulty of establishing the exact time period that has passed since the development of thrombosis (clinical signs are delayed by several days), the selection of patients for radical thrombectomy must be extremely careful. Regional thrombolytic therapy. Preferred is regional administration directly into thrombotic masses using a pre-installed catheter. Streptokinase, urokinase, and alteplase are used as thrombolytic drugs. The effectiveness of catheter thrombolysis for DVT is currently the subject of active study, and therefore the method can be recommended only in cases where the potential benefits of thrombolysis are obvious and the risks are minimal. Its implementation can only be considered in patients without severe somatic pathology, with a low risk of bleeding, with a disease duration of no more than 14 days and occlusion of 1-2 anatomical segments.
Therapeutic tactics for deep vein thrombosis in patients from traumatology and orthopedics departments. Algorithm for identifying VTEC. A daily clinical examination of the patient should include active identification of symptoms of acute thrombosis of the deep and superficial veins of both lower extremities. During delayed surgical treatment of patients with injuries or diseases of the musculoskeletal system accompanied by immobilization, especially if adequate drug prophylaxis was not carried out, it is advisable to perform ultrasound compression ultrasonography of the veins of the inferior vena cava system before surgery to identify asymptomatic veins. -nosal thrombosis with the study as close as possible to the time of intervention. In some cases, when preventive measures were not carried out in full or there is a particularly high risk of developing VTEC, performing ultrasound compression ultrasonography is advisable even before activating the patient. Tactics of a traumatologist-orthopedist in identifying VTEC. Identification of signs of acute thrombosis of superficial, deep veins and/or pulmonary embolism, as well as reasonable suspicion of them, is the basis for consultation with a vascular surgeon. Surgeries on the musculoskeletal system should be postponed until the risk of embolism has been eliminated. The plaster cast should be cut and its edges separated. If intervention is necessary for vital reasons, the installation of a cava filter or plication of the inferior vena cava should be considered, after which surgery is possible while administering prophylactic doses of direct anticoagulants. Before instrumental examination, patients with DVT and/or PE should be prescribed strict bed rest to reduce the risk of PE. After examination, patients with non-embolic forms of venous thrombosis can be activated. The basis of treatment for patients with VTEC (including asymptomatic ones) is adequate anticoagulant therapy. Further treatment of a patient with VTEC is carried out jointly by a vascular surgeon and a traumatologist-orthopedist. After eliminating the threat of pulmonary embolism and selecting adequate anticoagulant therapy, it is possible to treat the patient in the trauma department. Features of treatment tactics in different categories of patients With venous thrombosis, treatment tactics depend on the location, embolic danger of the thrombus and at what stage of treatment of patients with injuries and diseases of the musculoskeletal system (MSA) this complication was identified. 1. Venous thrombosis identified during preoperative examination A. The patient does not require emergency or urgent surgical intervention
— Thrombosis of superficial veins. When thrombosis is localized in the basin of the great saphenous vein proximal to the level of the knee joint, crossectomy is indicated, after which intervention on the musculoskeletal system (MSA) can be performed. Further treatment of superficial vein thrombosis is carried out depending on the severity and extent of the pathological process. — Deep vein thrombosis. Patients with non-embolic forms of thrombosis are recommended to undergo anticoagulant therapy (LMWH or UFH) with dynamic ultrasonic monitoring of the state of the thrombus and venous bed. After the thrombotic process has stabilized, confirmed by ultrasound angioscanning data, and the clinical manifestations of thrombosis have subsided (after 3-5 days), it is possible to perform surgical intervention on the musculoskeletal system. 12 hours before surgery, the therapeutic dosage of anticoagulants is replaced with a prophylactic dose of LMWH. After surgery (24 hours after the previous injection), provided that hemostasis is stable, LMWH is re-administered in a prophylactic dose. From the second day of the postoperative period, therapeutic doses of anticoagulants are used. Further treatment tactics for DVT are carried out depending on the severity and extent of the pathological process. In the postoperative period, dynamic ultrasound monitoring of the condition of the thrombus and venous bed is carried out (every 3-5 days). For patients with an embolic (floating) thrombus, implantation of a removable model of a vena cava filter is indicated, after which surgical intervention on the musculoskeletal system is possible within a time frame determined by an orthopedic traumatologist. The tactics of anticoagulant therapy are similar to those used for non-embolic thrombosis. B. The patient needs emergency or urgent surgical intervention - Superficial vein thrombosis. If thrombosis is localized in the basin of the great saphenous vein proximal to the level of the knee joint, a crossectomy is indicated, after which intervention on the musculoskeletal system can be performed. Further treatment of superficial vein thrombosis is carried out depending on the severity and extent of the pathological process. — Deep vein thrombosis A. Iliocaval segment In the postoperative period, there is a high probability of progression of the thrombotic process, and therefore patients with any form of thrombosis are advised to undergo implantation of a removable model of a vena cava filter, followed by the proposed surgical intervention on the musculoskeletal system. B. Femoropopliteal segment and veins of the leg In case of an embolic thrombus, implantation of a removable model of a vena cava filter is indicated. As an alternative, ligation of the superficial femoral vein with an absorbable ligature is possible. In patients with a floating thrombus of the common femoral vein, the first stage is thrombectomy from the common femoral vein. Performing an intervention on the deep venous system is indicated as the first stage in one operating session with intervention on the musculoskeletal system. For tactics for non-embolic thrombus, see above. In the postoperative period, patients are administered a prophylactic or intermediate dose of heparin 6-8 hours after surgery, subject to stable hemostasis. From the second day of the postoperative period, patients receive standard therapy with therapeutic doses of anticoagulants. 2. Venous thrombosis detected in the postoperative period and in a patient for whom surgical treatment is not planned. Standard tactics for treating superficial and deep vein thrombosis are used. Therapeutic tactics for DVT during pregnancy, at the stage of delivery and in the postpartum period During pregnancy, it is recommended to use LMWH in therapeutic doses for the treatment of VTEC. Together with a vascular surgeon, the issue of the need to install a vena cava filter or another method of surgical treatment and prevention is decided. For VTEC occurring during pregnancy, LMWH or UFH should be used throughout pregnancy; LMWH are the drug of choice. The optimal dose of LMWH for long-term use has not been determined. After initial use of standard therapeutic doses of LMWH for at least 1 month, the dose can be reduced to 75% of the therapeutic dose. After delivery, heparin can be replaced with NOAC or ABK. It should be remembered that the use of NOACs is contraindicated during pregnancy and breastfeeding. In such cases, the use of VKA with a target INR of 2.0-3.0 is justified, subject to conditions that ensure safe change of drugs during treatment (see Appendix 1). Experts believe that if VTEC occurs during pregnancy, anticoagulants should be used for at least 1.5 months after birth, and the total duration of treatment should be at least 3 months. Subcutaneous administration of HMH or UFH should be discontinued 24-36 hours before labor or cesarean section. In pregnant women with a particularly high risk of recurrent VTE during this period, it is advisable to switch to intravenous infusion of UFH, which should be interrupted 4-6 hours before delivery or cesarean section; in some cases, consider the advisability of installing a temporary vena cava filter. In case of unplanned onset of labor, neuraxial anesthesia is contraindicated; if bleeding occurs, a marked increase in aPTT (in cases when UFH was used) or a high level of anti-Xa activity in the blood (in cases when LMWH was used), administration of protamine sulfate may be required to neutralize the effect of these drugs. Therapeutic tactics at the stage of delivery The method of delivery is determined by the specific obstetric situation. • If external bleeding occurs, including vaginal bleeding, or at the onset of labor, stop using LMWH and UFH. • If signs of threatening preterm labor appear in pregnancy up to 35-36 weeks in patients who have previously used LMWH in therapeutic doses, continue their use or switch to UFH as a drug with a shorter half-life. • In the presence of massive blood loss or blood transfusion, begin or resume drug prophylaxis of VTE immediately after the risk of bleeding has decreased. • If there is a high risk of bleeding, use UFH, recommend wearing compression stockings and/or perform pneumocompression. • In the case of using LMWH, induction of labor, cesarean section, regional anesthesia and analgesia techniques should be postponed for at least 24 hours after administration of the last therapeutic dose of LMWH. • If UFH is used, induction of labor, caesarean section, regional anesthesia and analgesia techniques should be postponed for at least 4-6 hours after the administration of UFH. • Anticoagulant therapy should be resumed 12-24 hours after birth in the absence of hemorrhagic complications. • Removal of the epidural catheter should be carried out no earlier than 12 hours after the administration of prophylactic doses of LMWH or 4 hours after the administration of prophylactic doses of UFH. • Resume the administration of LMWH and UFH no earlier than 4-6 hours after the use of spinal anesthesia or after removal of the epidural catheter.
• If it is impossible to stop the administration of LMWH or UFH during labor (for example, in women with spontaneous labor within 24 hours after the last dose of LMWH), do not prescribe regional analgesia techniques, but use alternative methods of analgesia, for example, controlled intravenous opiate-based analgesia, and for caesarean section - general anesthesia. Therapeutic tactics in the postpartum period • Early activation (within 2-4 hours after childbirth or cesarean section), if impossible, use of compression stockings and/or pneumocompression. • Anticoagulant therapy after childbirth continues for at least 6 weeks (with a total duration of treatment with anticoagulants of at least 3 months). • Possible use of LMWH, UFH and warfarin
Diagnostics and clarification
To establish the cause of obstruction of blood flow through the vena cava system and select further tactics, a number of diagnostic procedures are shown:
- History taking and physical examination.
- General blood test, biochemistry, coagulogram.
- Doppler ultrasound and duplex scanning of veins.
- Plain radiography of the chest and abdominal organs.
- CT, MRI with contrast.
- Magnetic resonance phlebography.
- Measurement of central venous pressure (CVP).
Treatment methods
The choice of patient management tactics depends on the cause of blood flow disturbance in the portal veins.
Today, almost all cases of thrombosis are treated conservatively. Studies have shown that after thrombectomy, clot fragments remain on the vessel wall, which subsequently serve as a source of re-occlusion or the development of a dangerous complication of the BODY (pulmonary embolism).
Compression of a vessel by a space-occupying lesion or tumor invasion of the vein walls requires surgical intervention. The prognosis for conservative management of the disease is unfavorable.
Surgical methods
Types of surgical interventions for vena cava thrombosis:
- endovascular thrombectomy with Fogarty catheter;
- open clot removal;
- palliative plication of the vena cava (artificial formation of the lumen with U-shaped staples);
- installation of a vena cava filter.
In case of external compression of the vessel or metastatic lesion, palliative interventions are performed:
- stenting the narrowing area;
- radical decompression (removal or excision of tumor formation);
- resection of the affected area and replacement with a venous homograft;
- shunting of the obliterated area.
Drug treatment
The most effective method of conservative treatment for blockage of deep veins by a clot is thrombolytic therapy (Alteplase, Streptokinase, Actilyse).
Criteria for choosing this treatment method:
- age of thrombotic masses up to 7 days;
- no history of acute cerebral blood flow disorders in the last 3 months;
- the patient did not undergo surgical procedures for 14 days.
Additional drug support regimen:
- Anticoagulant therapy: “Heparin”, “Fraxiparin” intravenous drip with further transition to subcutaneous administration.
- Improving the rheological qualities of blood: “Reosorbilact”, “Nicotinic acid”, “Trental”, “Curantil”.
- Venotonics: Detralex, Troxevasin.
- Nonsteroidal anti-inflammatory drugs: Indomethacin, Ibuprofen.
Diagnostic methods
To confirm the diagnosis of acute thrombosis, a study of blood coagulation activity is prescribed, the most informative indicator of which is the determination of plasma D-dimer. Excess of it means the beginning of the formation of blood clots in the vessels. The technique has high reliability, but lacks specificity, since in case of tumor, inflammation, infection, pregnancy and after surgery, the level of this substance is initially increased.
In order to find a blood clot in the body, fibrinogen labeled with radionuclides is used. This pharmaceutical reveals hidden blood clots and, during scanning, signals their location. However, the type of blood clot and its danger cannot be determined.
Duplex ultrasound examination of blood vessels
Vascular ultrasound is one of the most optimal methods for diagnosing venous and cardiac thrombosis . The most complete information can be obtained by duplex scanning with Doppler color mapping. In this case, the following properties of the blood clot can be assessed:
- density (the longer the process, the coarser the structure of the clot);
- diameter of the vessel or size of the cardiac cavity;
- degree of blockage;
- mobility.
The angiographic research method is used when the data obtained at the previous stages of the examination is insufficient. It can be combined with the installation of a vena cava filter and removal of a blood clot.
Signs of a floating thrombus:
- the large vein from which the head of the thrombus “grows” is poorly contrasted;
- the filling defect has the shape of a leech or tongue;
- the base of the clot is larger than the moving part.
Watch the video about what a floating blood clot looks like on ultrasound:
conclusions
Impaired blood flow through the vena cava system is a pathological condition that is difficult to treat and has a high mortality rate. Also, in 70% of cases, re-occlusion or rethrombosis of the affected segment is observed within a year. The most common fatal complications are: BODY, major ischemic stroke, acute renal failure, bleeding from esophageal varices and cerebral hemorrhage.
In the case of tumor damage to blood vessels, the prognosis is unfavorable. Treatment is palliative in nature and is aimed only at alleviating existing symptoms and some continuation of the patient’s life.