Among the various forms of cardiomyopathy, restrictive cardiomyopathy is the most common in children. The development of pathology is associated with fibrosis of the heart muscle, due to which the heart begins to contract less efficiently. In the absence of treatment or an unfavorable course of the disease, complications in the form of heart failure may occur.
Restrictive cardiomyopathy (RCM) is a rare myocardial disease and the least common of the other two clinically recognized and described cardiomyopathies. Characterized by diastolic dysfunction with limited capacity. Atrial enlargement occurs due to disruption of ventricular filling during diastole, but the volume and thickness of the walls of the ventricular chambers usually remain within normal limits.
Restrictive cardiomyopathy accounts for approximately 5% of all diagnosed cardiomyopathies. [1 - Huby AC; Mendsaikhan U; Takagi K; Martherus R; Wansapura J; Gong N; Osinska H; James JF; Kramer K; Saito K; Robbins J; Khuchua Z; Towbin JA; Purevjav E. Disturbance in Z-disk mechanosensitive proteins induced by a persistent mutant myopalladin causes familial restrictive cardiomyopathy. J Am Coll Cardiol. 2014; 64(25):2765-76]
RCM may be idiopathic or secondary to other diseases, particularly amyloidosis and endomyocardial disease with or without hypereosinophilia. The prognosis for RCM depends on the clinic and treatment. The disease has been found to be a significant cause of heart failure with preserved ejection fraction. Due to the difficulties associated with diagnosing RCM, several methods should be used during the examination of patients.
Video: Restrictive cardiomyopathy: causes, symptoms, diagnosis, treatment and pathology
Description
Restrictive cardiomyopathy can be either hereditary or acquired. In both cases, it is equally common among males and females. Increased myocardial stiffness causes ventricular pressure to increase sharply even with a small increase in blood volume. Thus, the highest measure of filling occurs in the early phase of diastole and ends abruptly at the end of rapid filling.
Decreased left ventricular filling volume results in decreased cardiac output. Early in the disease process, systolic function usually remains normal. Wall thickness may be increased in cases of infiltrative processes such as amyloidosis, but the change is usually not as pronounced as in hypertrophic cardiomyopathy.
As the disease progresses, there is a variable decline in systolic function and the development of symptoms of decreased cardiac output. Increased filling pressures can manifest as pulmonary and systemic overload. RCM affects both ventricles and can therefore cause signs and symptoms of both left- and right-sided heart failure.
In some cases, complete blockage of the heart occurs as a result of developed fibrosis involving the sinoatrial or atrioventricular nodes.
Classification of restrictive cardiomyopathy by type (Kushwaha P. et al., 1997)
- Restrictive myocardial cardiomyopathies:
1. Non-infiltrative:
1.1 Idiopathic cardiomyopathy; 1.2 Familial cardiomyopathy; 1.3 Hypertrophic cardiomyopathy; 1.4 Scleroderma; 1.5 Pseudoxanthoma elastica; 1.6 Diabetic cardiomyopathy
2. Infiltrative:
2.1 Amyloidosis; 2.2 Sarcoidosis; 2.3 Gaucher disease; 2.4 Hurler's disease; 2.5 Fatty infiltration
3. Storage diseases:
3.1 Hemochromatosis; 3.2 Fabry disease; 3.3 Glycogen storage disease
- Restrictive endomyocardial cardiomyopathies:
- Endomyocardial fibrosis
- Hypereosinophilic syndrome
- Carcinoid heart disease
- Metastatic cancer lesion
- Radiation damage to the heart
- Toxic effects of anthracyclines
- Drug-induced fibrous endocarditis
Endocardial fibrosis can extend to the atrioventricular valves and cause regurgitation. There are two forms of endomyocardial fibrosis (EMF)—active eosinophilic EMF and chronic EMF.
Prevalence of restrictive cardiomyopathy:
- Idiopathic RCM is seen primarily in the United States.
- Loeffler's endocarditis is common in temperate climates.
- Chronic endomyocardial fibrosis is observed exclusively in tropical and subtropical countries in Africa, Asia and South America.
- EMF is most common in children and young people living in Uganda and Nigeria, often accounting for up to one quarter of deaths due to heart failure in these areas.
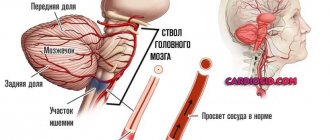
What happens to the heart?
Restrictive cardiomyopathy is a rare, dangerous disease. Its symptoms must be treated carefully in order to prescribe timely treatment. What happens to the heart?
The main functions of the heart are disrupted - both pumping and diastolic. The development of the disease goes through three stages.
- Infiltration of the myocardium, as a consequence, progression of coronaritis (inflammation of the walls of the arteries of the heart) - necrotic stage.
- Endocardial hypertrophy, development of vascular thrombosis - thrombotic stage.
- Myocardial fibrosis and nonspecific obliterating endarteritis of the coronary arteries - fibrous stage.
Changes in the heart with restrictive cardiomyopathy
The main symptom characterizing restrictive cardiomyopathy manifests itself in the form of insufficient blood circulation. This in turn leads to:
- severe shortness of breath;
- weakness with simple movements;
- swelling;
- swelling of the veins in the neck;
- development of ascites (dropsy in the abdominal cavity);
- hepatomegaly (severe enlargement of the liver).
However, the heart is not enlarged or slightly enlarged, and the ECG shows atrial fibrillation and arrhythmia. On the ECG, the ST segment is reduced, and T wave inversion is also visible. X-ray studies show venous congestion in both lungs - these are the symptoms. A blood test shows eosinophilia (increased white blood cells).
Causes
Restrictive cardiomyopathy can be caused by a variety of local and systemic disorders; many of them are quite rare.
According to World Health Organization (WHO) guidelines, the term “cardiomyopathy” refers to myocardial diseases that are idiopathic (ie, primary cardiomyopathies). However, secondary infiltrative myocardial diseases, which are actually cardiac manifestations of systemic diseases, are often grouped together with cardiomyopathies.
The causes of RCM can be divided into two large groups as follows:
- Primary/idiopathic RCM. These include endomyocardial fibrosis (ECF), eosinophilic endomyocardial Loeffler's disease.
- Secondary RCM. The group includes causes such as amyloidosis, sarcoidosis, hemochromatosis, progressive systemic sclerosis (scleroderma), carcinoid heart disease, hemogenic heart disease, radiation/treatment induced, metastatic malignancy, anthracycline toxicity.
Prognosis of restrictive cardiomyopathy
The prognosis, as with dilated cardiomyopathy, is unfavorable. This is due to the fact that this diagnosis is usually not established immediately, but in later stages. In such cases, only symptomatic treatment is indicated.
About 65% of patients live with this diagnosis for about 5 years. 50% of patients survive 10 years after diagnosis of restrictive cardiomyopathy. Almost all patients suffer from heart failure of varying degrees.
Thus, restrictive cardiomyopathy is a disease accompanied by impaired compliance of the heart walls. Usually one of the ventricles of the heart is affected. The main symptoms that bother patients are fatigue and shortness of breath. The diagnosis is made using several instrumental research methods. The main one is echocardiography. Therapy is symptomatic, often ineffective. In severe cases, surgical treatment is indicated
Kinds
Primary (idiopathic) RCM
Both genetic and sporadic cases of primary (idiopathic) RCM have been described. It is a rare disease that can affect children and adults, while men and women are equally affected. The prognosis for children is worse than for adults. Genetic cases are most often based on autosomal dominant inheritance with incomplete penetrance. The mutation appears to occur in genes encoding sarcomeric proteins, including troponin I, troponin T, alpha-cardiac actin, and beta-myosin heavy chain. The presence of a positive history of familial RCM is determined in approximately 30% of cases. [2 - Huby AC; Mendsaikhan U; Takagi K; Martherus R; Wansapura J; Gong N; Osinska H; James JF; Kramer K; Saito K; Robbins J; Khuchua Z; Towbin JA; Purevjav E. Disturbance in Z-disk mechanosensitive proteins induced by a persistent mutant myopalladin causes familial restrictive cardiomyopathy. J Am Coll Cardiol. 2014; 64(25):2765-76]
In many cases, cardiac muscle disease has no known cause and presents with heart failure and restrictive hemodynamics but without significant ventricular hypertrophy. Endocardial thickening or fibrosis associated with eosinophilia or other histopathological changes may be present.
In addition to symptoms of right or left heart failure, thromboembolic complications may be present in one third of patients with idiopathic RCM. Pathologically, these patients have greatly enlarged atria, which is clearly visible on a chest x-ray. Echocardiography in such cases shows bilateral atrial dilatation with normal ventricular size, as well as significant diffuse left ventricular hypertrophy, especially in the presence of amyloidosis. The histologic features of idiopathic RCM include interstitial fibrosis that is minimal in some patients and quite extensive in others.
Eosinophilic cardiomyopathy (Loeffler's endocarditis) and ECP are the most common global causes of RCM, affecting approximately 12 million people worldwide. This condition is observed in equatorial Africa and, less commonly, in tropical and subtropical Asia and South America.
Severe long-term eosinophilia from any cause (eg, allergic, autoimmune, parasitic, leukemic, or idiopathic) can lead to eosinophilic infiltration of the myocardium.
Eosinophilic cardiomyopathy, also known as Loeffler's endocarditis, begins with an acute inflammatory phase characterized by fever. Disruption of the structure of the left and right ventricles occurs in the intermediate phase, and then the final stage, which includes the development of endocardial fibrosis, lasts from several months to several years.
The prognosis is poor for patients with diffuse cardiac damage. Localized lesions associated with the valves are amenable to surgical reconstruction or removal and replacement.
Secondary RCM
Infiltrative RCM
Infiltrative cardiomyopathies are characterized by the deposition of abnormal substances (amyloid proteins, noncaseating granulomas, iron) within the cardiac tissue. Infiltration leads to thickening of the ventricular walls, which contributes to the development of diastolic dysfunction. The disease occurs in a variety of age groups and, given the systemic nature of the underlying pathology, is characterized by extracardiac manifestations.
Restrictive disorders predominate early in the disease, causing conduction abnormalities and diastolic heart failure. Unfavorable remodeling can lead to systolic dysfunction and ventricular arrhythmias.
Amyloidosis is the most common cause of RCM in the United States. Studies have shown that there may be a higher prevalence of amyloidosis among older patients with heart failure and preserved ejection fraction.
Amyloidosis is characterized by multisystem protein deposition known as amyloid fibrils. It usually presents as a systemic disorder with infiltration of the liver, kidneys, intestines, nerves, skin and tongue. Cardiac involvement is also quite common and is a major source of disease-related mortality.
In amyloidosis, the myocardium thickens and becomes hard, rubbery, and unable to contract as amyloid accumulates in the heart tissue. These changes lead to abnormalities in contractility, conduction, and disruption of coronary blood flow. Biventricular diastolic dysfunction causes increased intracardiac pressure and may progress to systolic dysfunction.
Amyloid can be deposited in any part of the heart, including the myocardium, blood vessels, endocardium, valves, epicardium, and parietal pericardium. The ventricular walls usually thicken, sometimes with disproportionate enlargement of the septum, and may mimic the appearance of hypertrophic cardiomyopathy. Atrial dilatation develops as a consequence of increased pressure and filling of the ventricles.
Classic two-dimensional echocardiographic findings include increased left ventricular and right ventricular wall thickness, normal or small left ventricular cavity size, and preserved ejection fraction. One third of patients may have normal left ventricular wall size. Typically there is effusion and thickening of both the valves and the papillary muscles.
Other less common forms of infiltrative RCM include:
- Sarcoidosis: characterized by the presence of non-caseating granulomas (cardiac involvement is 25-30%).
- Hemochromatosis and cardiomyopathy with excessive amounts of iron.
- Danon disease: deficiency associated with membrane protein 2 (LAMP2).
- Friedreich's ataxia: mutation of the frataxin gene (FXN).
Video: Amyloidosis Awareness (narrated by Michael York) — Available in 14 Languages
Drug-induced RCM
Post-radiation fibrosis . Radiation-induced myocardial and endocardial fibrosis is the cause of non-infiltrative RCM. Fibrosis causes endothelial cell damage and subsequent microvascular dysfunction. An increase in the total concentration of collagen leads to a decrease in the distensibility of ventricular tissue. Radiation affects the coronary vessels, valves and pericardium. This complication of radiation therapy, as with pericardial tamponade, appears several years after treatment. It is quite difficult to diagnose. Echocardiography may demonstrate normal left ventricular wall thickness with abnormal left ventricular filling, valvular calcification, and pericarditis.
Drug-induced RCM is a rare disease that has been described after long-term use of antimalarial drugs (chloroquinone and hydroxychloroquinone).
Common heart disorders include conduction abnormalities and thickening of the valves.
Cardiomyopathy in children: causes, symptoms, treatment, diet
Cardiomyopathy refers to a whole group of diseases (non-inflammatory) of the heart sac with a predominance of myocardial damage. In this case, neither valve damage nor hypertension (pulmonary or arterial) occurs. These serious diseases are characterized by an increase in heart size and heart failure.
The course of the disease can be acute (develops over several weeks), subacute or chronic (over several months).
Causes
Many viral or bacterial infections suffered by a child can trigger the development of cardiomyopathy.
The exact cause of these diseases has not been established. Most scientists support the assumption that infectious factors and genetic predisposition are important for the occurrence of cardiomyopathy.
It is believed that the following infections at the stage of intrauterine development are important for the development of cardiomyopathy in newborns and children after one year:
- toxoplasmosis;
- herpetic infection;
- staphylococcal;
- cytomegalovirus;
- adenoviral;
- rubella, etc.
Bacterial or viral infections can provoke cardiac pathology at any age of the child.
The following factors cannot be excluded:
- intrauterine hypoxia;
- asphyxia during childbirth;
- sepsis;
- birth trauma of the central nervous system.
Genetic aspects also play a significant role, since the family nature of the pathology is often revealed. Moreover, not only the child’s parents get sick, but also close relatives. Many experts are of the opinion that heredity plays the leading role for newborns.
In adolescents, a provoking factor for the occurrence of cardiomyopathy can be excessive psycho-emotional or physical stress or even rapid growth.
Regardless of the age of children, the basis of cardiomyopathy is a violation of all metabolic processes in the tissues of the heart sac. The result of metabolic and mineral disorders are dystrophic changes that most often occur in the myocardium, less often in the outer (pericardium) or inner (endocardium) membranes of the heart sac.
The consequence of these irreversible changes is the expansion of the cavities of the heart, a decrease in the elasticity of the bursa, and increasing heart failure.
Depending on the state of intracardiac circulation, the following types or forms of cardiomyopathy are distinguished:
- hypertrophic;
- dilatational;
- arrhythmogenic;
- restrictive.
The type of disease suggests a possible cause of the developed process. In many children, there may be several reasons for the development of cardiomyopathy. If the cause is unknown, the idiopathic form is diagnosed.
Symptoms
Clinical manifestations of various types of cardiomyopathy:
- Hypertrophic cardiomyopathy can occur in children of any age, even newborns. The main symptom of the disease is an increase in the cavity of the left ventricle and a gradual deterioration in the contractile function of the heart. Rhythm disturbances, frequent dizziness, and fainting may also occur. Shortness of breath is caused by physical exertion, and increased fatigue is noted.
In young children, heart failure may develop due to congestion. The prognosis for this form is more favorable than for others. A rapid course with a fatal outcome rarely develops.
However, this form of cardiomyopathy may have a long asymptomatic period, and sudden fainting and subsequent death of the child may be the only manifestation of the disease.
- Dilated cardiomyopathy is the most common form of the disease. Occurs in children at any age. It happens less often in girls than in boys. With this form, all the cavities of the heart expand, the contractility of the heart muscle decreases, and eventually heart failure develops.
The cause of the disease in most children cannot be determined. It has a gradual course. Babies do not gain weight well; when feeding, the child often stops sucking due to lack of air.
In older children, signs of heart failure prevail:
- increased fatigue even with light load;
- constant weakness;
- swelling of the lower extremities or even ascites (sweating of fluid into the abdominal cavity);
- shortness of breath and wet cough (especially at night).
With this form of the disease, blood clots may form in the heart cavity. If a blood clot breaks away from the wall, it can cause blockage of a blood vessel in various organs and, as a result, a kidney infarction, cerebral stroke, or pulmonary infarction. Ischemia can also develop in the myocardium itself as a consequence of irreversible metabolic disorders and changes in the vascular wall.
- Restrictive cardiomyopathy is one of the rarest forms of the disease. Its share is 5% of the total number of cardiomyopathies. It is characterized by a pronounced decrease in the elasticity of the myocardium and its contractility, a gradual course.
The disease may be primary (idiopathic) or secondary (due to a systemic or autoimmune disease), and may be familial (but the specific defective gene has not yet been identified). Some cases may be caused by viral or bacterial infections.
It may be asymptomatic for a long time. Clinical manifestations are dominated by symptoms of congestion in the systemic circulation. The symptoms of heart failure progress slowly. Children are lagging behind in development, and there is increasing weakness and lethargy of the child. At the slightest stress (for example, when crying), acrocyanosis (cyanosis) appears on the face and fingers.
Older children are inactive and do not participate in outdoor games. Shortness of breath and acrocyanosis occur during physical exertion. Teenagers are worried about a cough, a feeling of lack of air, palpitations, heart pain, and constant weakness.
- Arrhythmogenic cardiomyopathy is rare in childhood, but according to research, it is the cause of death in 25% of children with cardiomyopathy.
- Experts identify another form - dysmetabolic cardiomyopathy, but it is not an independent disease, but one of the manifestations of systemic diseases. Dystrophic metabolic changes in the myocardium occur against the background of:
In these diseases, symptoms of the underlying process predominate, and cardiac damage is nonspecific.
Diagnostics
Additional research methods, in particular ECG, will help the doctor make a diagnosis.
In the absence of pronounced manifestations in the initial stage, cardiomyopathy can be detected accidentally during an ECG or Echo-CG during examination for any reason.
An ECG reveals significant metabolic disorders (the main sign of myocardial dystrophy), and an Echo-CG reveals an increased size of the heart.
The diagnosis of “cardiomyopathy” can be made under the basic condition of excluding congenital anomalies of the heart, valvular defects, pericarditis, and damage to the conduction system in the heart.
In cardiology departments, to verify the diagnosis, in addition to ECG and Echo-CG (ultrasound of the heart), the following diagnostic methods are used:
- Dopplerography;
- scintigraphy;
- chest x-ray;
- puncture biopsy of the cardiac sac;
- CT and MRI.
These methods make it possible to assess the condition of large vessels and the degree of dystrophic changes in the myocardium. But the main instrumental and most informative method for diagnosing this pathology is ultrasound of the heart.
Laboratory tests are used to determine water and electrolyte balance and monitor the effectiveness of treatment.
Treatment
The goal of treatment for all forms of cardiomyopathy is to eliminate (or reduce) the manifestations of heart failure and prevent complications.
Conservative therapy is aimed at:
- normalization of blood pressure (under the influence of inhibitors);
- improvement of metabolic processes (vitamins and anabolic steroids are prescribed);
- reducing the load on the heart during symptoms of heart failure (use of cardiac glycosides, diuretics for edema).
All drugs and their dosages, duration of use are prescribed by a pediatric cardiologist, taking into account the patient’s age, body weight and severity of the disease.
Conservative therapy can only be effective in the early stages of the disease and proper treatment. With significant changes, in advanced cases, a heart transplant is necessary.
Donor heart transplantation is more indicated for children suffering from dilated cardiomyopathy. And with the restrictive form, there is a high risk of relapse in the transplanted donor heart.
In the hypertrophic form of the disease, in some cases, implantation of an electrical pacemaker is indicated.
Diet
One of the components of treatment for cardiomyopathy is diet. Children should be fed 5-6 rubles. per day in small portions. It is recommended to include in the diet foods that improve blood circulation and normalize metabolic processes in the body.
Products containing magnesium and potassium (apricots, raisins, dried apricots, prunes, carrots, etc.) will be especially useful. You should pay attention to the amount of salt - it should be limited to 6 g per day. This requirement is explained by the property of salt to retain water in the body and contribute to the occurrence of edema.
In agreement with the cardiologist, the volume of fluid consumed per day is also determined, since a larger volume of circulating blood will increase the load on the heart and increase blood pressure, which is undesirable for this pathology.
Including steamed or boiled fish (low-fat varieties) in your diet will provide the body with essential fatty acids (omega-3). They will help lower blood pressure and prevent blood clots, which is very important for cardiomyopathy.
Recommended Products:
- As a first course - vegetarian soups (vegetable, with vegetable oil) or dairy.
- Meat and fish (low-fat varieties), seafood.
- Porridge and pasta (from durum wheat).
- Vegetables (boiled, baked, stewed); Eating vegetables raw should be avoided.
- White dietary bread without salt and crackers made from it.
- Low-fat fermented milk products (kefir, yogurt, cottage cheese).
- Chicken eggs (1 piece per day), soft-boiled, or steamed omelet.
- Berries and fruits, including dried fruits.
- Juices (preferably freshly squeezed) vegetable and fruit.
- Honey (if there is no allergy).
- Tea, loosely brewed (preferably white or green).
You should exclude from your diet:
- broths;
- sausages;
- fatty and fried foods;
- seasonings and sauces;
- legumes;
- smoked meats, pickles;
- canned food;
- baked goods and confectionery products;
- carbonated drinks;
- margarine, cream, full-fat sour cream.
Forecast
The most suitable first course for a child with cardiomyopathy is vegetarian soup.
The prognosis for dilated (the most common form) cardiomyopathy is very serious, most cases have an unfavorable outcome. Annual mortality is 10-20% of children; only 50% of sick children survive for 5 years.
With the hypertrophic form, the prognosis is somewhat more favorable. The annual mortality rate is from 2 to 6%. Children at an early age die from heart failure, and older children die suddenly from severe arrhythmia (ventricular fibrillation).
Restrictive cardiomyopathy also often has an unfavorable outcome. The cause of infant mortality is thromboembolism, chronic heart failure or other complications.
Children with congenital cardiomyopathy survive the first year, according to various sources, in 45-80% of cases. Death is possible within the first 3 months after birth.
In 25-30% of surviving infants, functional left ventricular heart failure develops. The successful outcome is influenced by the timing of detection of the disease and initiation of treatment. The highest survival rate is observed in early childhood.
Summary for parents
Cardiomyopathy in any form is a very severe damage to the heart, often leading to irreversible changes in the tissues of the heart sac and severe impairment of heart function. Only careful attention to the behavior and condition of the child on the part of the parents can help diagnose the disease in the early stages, which can somewhat optimize the prognosis during treatment.
Lecture by a specialist on the topic “Cardiomyopathies: general characteristics”:
Source: https://babyfoodtips.ru/20203622-kardiomiopatiya-u-detej-prichiny-simptomy-lechenie-dieticheskoe-pitanie/
Clinic
Symptoms of restrictive cardiomyopathy may include the following:
- Orthopnea
- Fatigue
- Heartbeat
- Gradual onset of shortness of breath
- Weight loss (cardiac cachexia)
- Paroxysmal nocturnal dyspnea
- Intolerance to strenuous exercise
- Abdominal discomfort or tenderness in the liver area
- Chest pain, especially in patients with amyloidosis or angina pectoris
Manifestations and symptoms of restrictive cardiomyopathy
Symptoms of the disease directly depend on the degree and nature of damage to the cardiac elements. Thus, it is possible to have both an asymptomatic and an extremely severe course of the disease with a rapid fatal outcome.
In the early stages it is possible:
- fast fatiguability;
- causeless weakness;
- attacks of shortness of breath at night;
- chest pain (only in some forms of amyloidosis).
Manifestations and symptoms of the disease in later stages:
- the development of congestive heart failure, the appearance of signs of liver enlargement and the appearance of edema in the body, the appearance of shortness of breath during physical activity;
- impaired cardiac conduction and the occurrence of thrombosis;
- the appearance of arrhythmia such as atrial fibrillation (atrial fibrillation);
- in rare cases - angina and fainting.
Diagnostics
Physical examination
Extracardiac manifestations of a systemic disorder may include the following:
- Increased jugular venous pressure
- Reducing impulse volume
- The appearance of ascites and acute edema of the lower extremities
- Hepatomegaly due to fluid or amyloid infiltration
- Light bruises, periorbital purpura, macroglossia (severely enlarged tongue), etc.
A cardiovascular examination may provide the following results:
- Normal heart sounds
- Loud sound of early diastolic filling
- Heart murmur due to mitral and tricuspid valve effacement (usually not hemodynamically significant)
Respiratory examination results:
- Breathing may be less audible on auscultation due to pleural effusions, often bilateral and extensive in amyloidosis
- Creeps or crackles are rarely heard
Establishing a diagnosis of RCM and excluding constrictive pericarditis is, as a rule, mandatory.
If restrictive cardiomyopathy is suspected, the following tests may be performed:
- Detailed blood test
- Blood gas analysis
- Serum electrolytes, nitrogen, urea, creatinine
- Liver markers
- Serum iron concentration and other possible indicators of hemochromatosis
- Serum brain natriuretic peptide level
The following instrumental diagnostic methods are selected:
- Radiography
- Angiography
- Echocardiography
- Cardiac catheterization
- Electrocardiography
- Radionuclide diagnostics
- Cardiovascular magnetic resonance imaging
- CT scan
- Ventricular biopsy
- Liver biopsy to diagnose hemochromatosis
Pathogenesis of restrictive cardiomyopathy
The mechanism of development of restrictive cardiomyopathy often leads to changes in other tissues and organs.
For example, amyloidosis affects only the heart muscle, but also the heart arteries. A similar process is observed in hemochromatosis. Farby's disease and sarcoidosis often affect the conduction system of the heart, causing blockages and contributing to the development of various rhythm disorders.
Loeffler's syndrome begins its manifestation in the form of inflammation of the arteries (arteritis) of eosinophilic origin. Then blood clots form on the endocardium, valves and chords of the heart. All this progresses to fibrosis.
The consequence of all of the above is myocardial infiltration and/or endocardial thickening. These changes prevent the ventricles from stretching properly, resulting in gradual development of diastolic dysfunction. As a result, venous pressure in the pulmonary circulation increases, lung function and gas exchange are disrupted. In parallel, parietal thrombi form inside the cardiac cavities. The danger is that these blood clots can migrate to various organs at any time, causing arterial thrombosis. This often leads to heart attacks and strokes.
Treatment
There is no specific treatment for restrictive cardiomyopathy. However, therapy aimed at specific causes of RCM is effective in some cases.
Pharmacological therapy may include:
- Beta blockers
- Amiodarone
- Cardioselective calcium channel blockers
- Diuretics
- Anticoagulants for patients with atrial fibrillation
- Digoxin (should be used with caution)
- Melphalan (for the treatment of antiplasma disorders in systemic amyloidosis)
- Chemotherapy (for amyloidosis)
- Corticosteroids, cytotoxic agents (eg, hydroxyurea), and interferon (for Loeffler's endocarditis)
- Therapeutic phlebotomy (for hemochromatosis)
Other types of treatment:
- Pacemaker implantation
- Endomyocardectomy
- Heart transplant
- New treatments (for example, RNA interference or freezing genes that are involved in the development of the abnormal protein in familial amyloidosis)
Video: Modern aspects of diagnosis and treatment of cardiomyopathies in childhood
Possible complications
- Stroke. Acute cerebrovascular accident. The ischemic variety is less lethal compared to the hemorrhagic one.
- Heart attack. Similar process. Accompanied by myocardial nutritional disturbances. Aggravates the course of cardiopathy.
- IBS. A harbinger of cardiac tissue necrosis.
- Discirculatory processes. Deviations from the nervous system.
- Vascular dementia is also possible. In the absence of timely assistance. This is a potentially reversible condition.
- The risk of Alzheimer's and Parkinson's disease increases significantly. And regardless of age.
- Heart failure.
- Cardiogenic shock.
All phenomena are potentially lethal. Some in the social sense, but more often we are talking about the biological cessation of existence.
Dilation type
It is considered the most common in clinical practice. It is characterized by uncontrolled growth of heart tissue, without the possibility of radical help.
Appears as a result of a long course of the rheumatoid process and other inflammatory pathologies. Stretching of the myocardial ventricles is observed.
Manifestations at an early stage are minimal. Diagnostics is not a problem. Echocardiography shows pronounced deviations in the anatomical development of the organ.
Otherwise the processes are identical. When working with children, diagnosis is simpler, since many factors: alcohol, smoking, nutritional factors, etc. are excluded.
Restrictive cardiomyopathy is the least common form of cardiomyopathy. It implies the presence of practically inextensible walls of the ventricles, which, due to lesions, cannot adequately fill the heart chamber with blood. The left side of the heart, in particular the left ventricle, is most often affected. This cardiomyopathy can be obliterating or non-obliterating. The first includes fibrosis of the subendocardium and endocardium (the inner layer of the heart). The second is infiltration of the myocardial layer by a pathological substance.
Forecast
Restrictive cardiomyopathy has the poorest prognosis of all types of cardiovascular disease. In particular, the mortality rate from 2 to 5 years is 50% and 70%, respectively, and RCM has the highest rate of sudden cardiac death. Due to the severe progression of the disease, patients with RCM often eventually suffer from heart failure and pulmonary hypertension.
The prognostic conclusion mainly depends on the pathology clinic, while treatment is often unsatisfactory. The prognosis is usually unfavorable for adults, since the pathology is often associated with progressive deterioration.
Patients whose condition is refractory to supportive care usually die from low-output heart failure. A radical transplant can help solve the problem.
The following complications most often develop with RCM:
- Pulmonary hypertension
- Thromboembolism
- Arrhythmia
- Cardiac or cardiac cirrhosis of the liver
- Progressive deterioration of cardiac function
4.80 avg. rating ( 94 % score) – 5 votes – ratings
Signs of illness
There are several symptoms of this disease. First of all, it is shortness of breath. The person begins to breathe frequently, but he cannot fully inhale the air. First, shortness of breath begins after physical exertion, and then in a calm state. It is rapid breathing at rest that is an alarming sign; it often indicates heart pathology.
In addition to shortness of breath, patients note that:
- they get tired quickly even with minor loads;
- feel heaviness in the upper abdomen (this is explained by the increased size of the liver);
- their legs swell;
- the heart beats irregularly.
In this state, a person may lose consciousness.
This occurs when heart block develops (no electrical impulse is sent to the muscle). Also read: Calcification and calcium index of the coronary arteries A disease such as restrictive cardiomyopathy can be asymptomatic (subclinical) in a child for a long time. Over time, the symptoms increase, and then adults take the children to the doctor. The severity of heart failure affects the severity of symptoms. The doctor determines the disease based on the brightness of the clinical picture.
Complaints in children are the same as in adults. But they still have a cough and an increase in the size of the abdomen.
This disease can develop in pregnant women in the last, third, trimester of pregnancy or shortly after the birth of the baby. The mechanism of its development is not uniform, so it is impossible to predict how the disease will progress.
Dysfunction of the heart muscle during pregnancy is caused by changes in the movement of blood through the vessels. Blood volume increases and blood pressure also changes. Hormonal levels are unstable. The emotional component also plays a role in the development of heart pathologies.
All of these factors can lead to cardiomyopathy. According to statistics, pregnant women more often suffer from dilated or hypertrophic forms of the disease. Their bodies are weakened and they often get tired. And such a pathology can pose a threat to the life of the expectant mother.