Anatomy
The communication between the left ventricle and the left atrium is carried out through the left atrioventricular orifice; the ventriculus sinister is completely isolated from the right ventricle by the interventricular septum. The aorta emerges from this chamber of the heart, through which blood, enriched with oxygen, passes through smaller arteries to the internal organs.
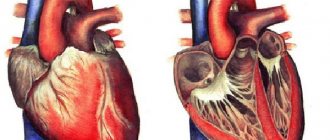
The left ventricle looks like an inverted cone, and is the only one of all the chambers that takes part in the formation of the apex of the heart. Due to its larger size than the right ventricle, it is believed that the heart is located on the left, although in fact it occupies almost the center of the chest.
The walls of the left ventricle are ten to fifteen millimeters thick, which is several times greater than that of the wall of the right ventricle. This is due to the more developed myocardium on the left side due to higher loads. That is, the higher the amount of work performed, the thicker the heart wall. The left ventricle pumps blood into the systemic circulation, while the right ventricle supplies the pulmonary circulation. That is why, under normal conditions, the latter is less developed, and its thickness is correspondingly smaller.
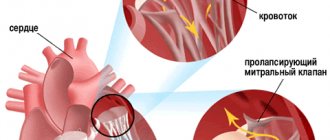
The atrioventricular communication (orifice) on the left side is closed by the mitral valve, consisting of a posterior and anterior leaflet. In this case, the anterior one is located in close proximity to the interventricular septum, and the posterior one is located outside of it.
Chords extend from both valves - tendon threads that attach the valves to the papillary muscles. Due to these muscles, the valve performs its functions, that is, during systole, blood does not return back to the atrium.
The papillary muscles are attached to special myocardial protrusions (fleshy trabeculae), which are located on the inner plane of the ventricle. Such trabeculae are especially developed in the area of the interventricular septum and the apex of the heart, but their number in the ventricle on the left is less than on the right.
The length and number of chords of the left ventricle are individual.
With age, their length gradually increases, being inversely related to the length of the papillary muscles. Most often, the chords that come from one muscle are attached to one valve. In addition, chordae are found that connect the papillary muscles with the trabeculae.
At the exit of the aorta there is a semilunar valve, which prevents blood from returning from the aorta to the heart.
The nerve impulse to the left ventricular myocardium enters through the Hiss bundle (its left leg). It is worth noting that only to the left ventricle the impulse is sent through two branches - anterior and posterior.
Pathologies
Pathological changes in the papillary muscles can occur either primarily or as a result of diseases of other parts of the heart.
Primary lesion of the SM in the form of hypoplasia or aplasia occurs when:
- congenital regurgitation of the mitral valve;
- trisomy 18 syndrome (Edwards);
- Ebstein's anomaly - the formation of valves from the muscle tissue of the ventricles.
Congenital defects of the mitral valve (MV), which serve as the basis for a defect in the papillary muscles:
- Additional MK - there is an additional element with an atypical fastening.
- Arcade mitral valve - SM have an abnormal structure, often fused into one and hypertrophied.
- Additional valves (three-, four-leaf MV) - additional groups of papillary muscles are detected.
- Parachute-shaped MV - echocardiography reveals an enlarged papillary muscle, which “connects” two MV leaflets at the same time.
In all of the above cases, defective papillary muscles aggravate the clinical manifestations of valvular insufficiency.
SM tissues can be affected by a tumor process (most often lymphoma). Also, papillary muscles are often damaged due to infectious diseases (endocarditis, rheumatism).
After suffering from an ulcerative variant of infective endocarditis, fusion of adjacent papillary muscles is observed with the formation of a valve defect with a predominance of insufficiency.
Changes in papillary muscles with tricuspid valve defects:
- blunting of the apexes of the spinal cord (especially the anterior ones);
- fusion of the anterior papillary muscles with the marginal zone of the tricuspid valve leaflets;
- marginal fusion of the spinal mass with the wall of the right ventricle.
Changes in the structure of the papillary muscles in acquired mitral valve stenosis:
- thickening and elongation of the SC;
- fusion of papillary muscles into a single conglomerate;
- soldering the edges of the CM to the surface of the left ventricle;
- the tops of the muscles are soldered to the leaflets of the mitral valve.
An increase in the size of the SM is observed in hypertrophic cardiomyopathy, since the papillary muscles are a continuation of the inner layer of the ventricular myocardium. Enlarged SM reduces the useful volume of the left sections, which reduces the ejection fraction and aggravates hemodynamic disorders.
In the last 70 years, the term “cirrhotic cardiomyopathy” has appeared - a change in the structure and functioning of the myocardium due to metabolic and hemodynamic disorders caused by liver cirrhosis. Impaired contractile function of the papillary muscles in such patients leads to the formation of mitral and tricuspid insufficiency with intact (undamaged) valve tissue.
Rupture of the papillary muscles
Rupture of the papillary muscle is a serious condition caused by injury or myocardial infarction with subsequent “dissolution” of the fibers. This complication causes the patient’s death in 5% of cases.
More often, the posterior papillary muscle undergoes necrosis, which is explained by a poorer blood supply compared to the anterior one.
Due to rupture of the SM during ventricular systole, one of the leaflets of the mitral valve (MV) falls into the cavity of the left atrium. Failure of the MV allows blood to move in the opposite direction, which causes severe failure. Impaired fluid outflow leads to increased pressure in the pulmonary veins (cardiogenic edema) and a decrease in systemic hemodynamics.
Main symptoms and paraclinical signs of rupture:
- sudden onset – chest pain, rapid heartbeat, severe shortness of breath, foamy sputum;
- Auscultation: soft noise in the fourth intercostal space on the left, intensifying during systole and carried to the axillary region;
- weakening of the first sound at the apex of the heart;
- EchoCG - M-shaped flapping leaflet of the mitral valve, which opens into the atrium cavity when the ventricles contract;
- Dopplerography - varying degrees of regurgitation with turbulent blood flow.
Treatment of ruptures of the papillary muscles is exclusively surgical, after preliminary drug stabilization of the parameters. The essence of the intervention is the installation of an artificial MV or the removal of part of the leaflet with plastic surgery of the atrioventricular orifice. Early mortality reaches 50% after urgent cardiac surgery.
Also, with Q-myocardial infarction, most patients by the end of the first week develop dysfunction of the spinal cord, caused by ischemia and remodeling (restructuring) of the muscle “framework”. This condition does not require surgical treatment; symptoms decrease with intensive therapy for a heart attack.
Features of the left ventricle and its functions
Relative to other parts of the heart, the left ventricle is located downward, posterior and to the left. Its outer edge is somewhat rounded and is called the pulmonary surface. During life, the volume of this chamber increases from 5.5 cm3 (for newborns) to 210 cm3 (by eighteen to twenty-five years).
Compared to the right, the left ventricle has a more pronounced oval-oblong shape, is much more muscular and slightly longer.
There are several sections in the structure of the left ventricle:
- The anterior (arterial cone) communicates with the aorta through the arterial foramen.
- Posterior (the ventricular cavity itself), which communicates with the right atrium.
As mentioned above, due to the more developed myocardium, the thickness of the left ventricular wall is eleven to fourteen millimeters.
The function of the left ventricle is to release oxygen-enriched blood into the aorta (respectively into the systemic circulation), and then through a network of smaller arteries and capillaries, the organs and tissues of the whole body are nourished.
What are the papillary muscles of the heart?
Papillary muscles (papillary) are a continuation of the inner layer of cardiac muscle, which protrudes into the cavity of the ventricles, and with the help of chords attached to the apex ensures unidirectional blood flow through the chambers.
Anatomical classification of papillary muscles (PM):
- Right ventricle: Anterior.
- Rear.
- Septal.
- Front.
Physiology
Under normal conditions, the left and right ventricles function synchronously. Their work occurs in two phases: systole and diastole (contraction and relaxation, respectively). Systole, in turn, is divided into two periods:
- Tension: includes asynchronous and isometric contraction;
- Banish: Includes fast and slow banishment.
Asynchronous tension is characterized by uneven contraction of myocardial muscle fibers due to uneven distribution of excitation. The atrioventricular valve is closed at this time. After the excitation covers all myocardial fibers, and the pressure in the ventricles increases, the valve closes and the cavity closes.
After the blood pressure acting on the walls of the ventricle increases to eighty mmHg. Art., and the difference with the pressure on the aorta is 2 mm Hg. Art., the semilunar valve opens and blood rushes into the aorta. When reverse blood flow occurs from the aorta, the leaflets of the semilunar valves slam shut.
After this, the ventricular myocardium relaxes and blood flows from the atrium through the mitral valve into the ventricle. Then the process is repeated.
Main functions
The ultimate goal of the papillary muscles is to ensure unidirectional blood flow from the atrium to the ventricle.
During ventricular systole, the SM contracts synchronously with the myocardium and regulates the tension of the chordae tendineae attached to the edges of the atrioventricular valves. They pull the valves towards themselves, preventing blood from returning inside the atria during systole. Thus, with the help of the papillary muscles, a sufficient pressure gradient is created across the pulmonary and aortic valves.
In the initial stage of ventricular systole, the semilunar (aortic and pulmonary) valves are still closed, and the blood is directed along the path of least resistance back to the atria. But this is prevented by contraction of the papillary muscles and rapid closure of the valve leaflets. For some time, closed ventricular cavities are created, necessary to generate sufficient pressure to open the semilunar valves.
The papillary muscles ensure the proper functioning of the heart valve system. SMs are not attached to the aortic and pulmonary valve cusps, since their passive closure does not require a sharp change in the pressure gradient.
The valves of the atrioventricular connections are more massive and require rapid and strong pressure of the return flow of blood over several milliseconds for effective closure.
Left ventricular dysfunction
There are systolic and diastolic dysfunctions of this chamber of the heart.
With systolic dysfunction, the ability of the ventricle to push blood out of the cavity into the aorta is reduced, which is the most common cause of heart failure.
Such dysfunction usually occurs due to a decrease in contractility, which leads to a decrease in stroke volume.
Diastolic dysfunction of the left ventricle is a decrease in its ability to fill its cavity with blood (that is, ensuring diastolic filling). This condition can lead to secondary hypertension (both venous and arterial), which is accompanied by shortness of breath, cough and paroxysmal nocturnal dyspnea.
Heart defects
They can be acquired or congenital. The latter are a consequence of developmental disorders in the embryonic period. The category of congenital defects includes incorrectly formed valves, additional valves in the left ventricle or with an inappropriate chord length, an open septum between the ventricles, transposition (abnormal location) of the great vessels.
If a child has a ventricular or atrial septal defect, venous and arterial blood mixes. Children with similar defects, when combined with transposition of blood vessels, have bluish skin, which at first is the only symptom.
If transposition is present as an isolated defect, then hypoxia leads to instant death. In some cases (if the defect is detected before birth), surgery may be performed.
Surgical treatment is also necessary for other defects of the left ventricle (for example, defects of the aortic valve or mitral valve).
Causes of cardiac fibrosis
Fibrous fibers replace the focus of necrosis or inflammation in the myocardium. The structure of this tissue resembles a scar. The most common reasons for valves losing their flexibility and mobility are:
- age-related decrease in valve nutrition,
- rheumatic attack,
- tonsillitis, sinusitis, otitis media,
- scarlet fever,
- bacterial endocarditis or myocarditis,
- Marfan syndrome with mitral valve prolapse,
- atherosclerotic deposition of cholesterol on the aortic valves,
- myocardial infarction,
- autoimmune processes.
We recommend reading the article about mitral heart disease. From it you will learn about heart valve defects and their causes, symptoms, methods of diagnosis and treatment, and prognosis for patients.
And here is more information about atherosclerosis of the aorta and valves.
Left ventricular hypertrophy
Characterized by thickening of the ventricular wall.
The causes of this condition may be:
- Constant long-term training (professional sports).
- Physical inactivity.
- Smoking tobacco.
- Alcoholism.
- Farby's disease.
- Muscular dystrophy.
- Stress.
- Pathologies of peripheral vessels.
- Obesity.
- Atherosclerosis.
- Diabetes.
- Ischemia.
- Hypertension.
At first, the disease is asymptomatic, but as the process progresses, cardialgia, fainting, dizziness, and fatigue occur. Then comes heart failure, characterized by shortness of breath (including at rest).
How to treat the left ventricle of the heart
As mentioned above, heart defects most often require surgical treatment.
Left ventricular hypertrophy can be treated with a combination of beta blockers and Verapamil. This method allows to reduce the clinical manifestations of pathology. In addition to medications, it is recommended to follow a diet and give up bad habits, lose weight and reduce the amount of salt consumed.
The diet should be enriched with fermented milk and dairy products, fruits, seafood and vegetables. In addition, it is mandatory to reduce the amount of fats, sweets and flour. Moderate physical activity is recommended.
In addition to conservative therapy, surgical treatment is also used, aimed at removing an area of hypertrophied myocardium. It must be remembered that this pathology develops over several years.
If we are talking about left ventricular failure, then in this case special “heart” drugs are used: “Korglikon”, “Corazol”, “Strofanthin”, “Camphor”, “Cordiamin”, as well as oxygen inhalation and bed rest.