Neuroreflex extrasystole
It is the result of pathological irritation emanating from other internal organs through viscerocardiac reflexes, usually through the vagus nerve.
The reflexes emanating from the abdominal organs are of greatest importance. Therefore, every patient with an unknown cause of extrasystole should carefully examine the abdominal organs. The cause of reflex extrasystole can be processes in the lungs and mediastinum, pleural and pleuro-pericardial adhesions, pneumosclerosis and cervical spondyloarthrosis. In some cases, focal infection can play the role of a pathological reflex focus. Extrasystoles that occur when pressing on the carotid sinus, during swallowing, coughing fits, in a certain position of the body, especially lying on the left side, and in various diseases of the brain, are also of reflex origin, but due to their relative rarity, their clinical significance is less.
Accurate determination of the reflex origin of extrasystole very often encounters great difficulties. Only when the extrasystoles disappear after eliminating the pathological irritation, which is not always easy to achieve, can their reflex pathogenesis be confidently accepted.
The occurrence of reflex extrasystole is favored by the presence of general neuro-vegetative lability. Reflex moments can play a role in the occurrence or increase in extrasystoles in organic heart diseases. In such cases, it is impossible to distinguish reflex from organic extrasystoles.
“Heart rhythm disturbances”, L. Tomov
Extrasystolic arrhythmia
Reasons for the development of extrasystole at rest
Experts note the influence of increased vagus nerve tone on the development of supraventricular extrasystoles. Vagal influences (reflexes) affecting the functionality of the heart usually arise when:
- axial hernia of the esophagogastric opening in the diaphragm;
- deformations of the walls of the esophagus;
- reflux of stomach contents into the esophagus;
- gastric pneumatosis;
- bloating;
- obesity;
- constipation;
- difficulties in moving food through the gastrointestinal tract;
- gallstones;
- prostate adenoma;
- fibroids of the uterus.
In patients with an unknown etiology of extrasystole, it is necessary to examine the organs located in the abdominal cavity. In addition, reflex extrasystole (extraordinary impulses caused by reflexes) can be provoked by pathological processes in the mediastinum and lungs, and cervical spondyloarthrosis. Sometimes pathological reflexes cause pockets of infection.
Extraordinary impulses that are formed when exposed to small dilated areas of the internal carotid arteries, during prolonged coughing, during the process of swallowing, when lying down and with certain pathologies of the brain, are also considered reflex.
Hunting for extrasystole
In the magazine “60 years is not age,” the author talked about how he managed to cope with atrial fibrillation using herbal medicine, breathing exercises and dosed physical activity. Almost 30 years later, he was overtaken by another type of arrhythmia - extrasystole of tension. And he successfully dealt with it using the same proven methods
Last year I was “lucky” to become closely acquainted with another type of cardiac arrhythmias. As funny as it may be (or rather sad!), the reason for this was one of my unsuccessful attempts to convince my own wife of the benefits of Buteyko breathing. Try, for example, when she has a migraine, well, it’s quite easy, in my opinion, the breathing algorithm is 3 + 4 + 4 + 3 (3 steps - full breath, 4 steps - breath holding, pause, 4 step - full exhalation, 3 steps - pause).
“Galya,” I say once while walking, “it’s so simple. I’m not suggesting you hold your breath for a long time. Look, I'll do it now. And nothing will happen to me."
After a normal inhalation, I pause for 30 slow steps. No reaction from my wife. Apparently, the argument is insufficient.
Having quickly caught my breath, I take 40 leisurely steps. Again no reaction! The arguments are apparently unconvincing.
Then, after catching my breath, I venture 50 steps. My wife is somewhat surprised by my vitality. I don't feel well. I feel some interruptions in my heart function and prolonged slight shortness of breath.
Trying to convince my wife, I made a fundamental mistake, which K. Buteyko warned about. Breathing deeply after a long pause is dangerous. After three passionate and gambling runs that followed each other (with a progressively increasing oxygen debt!) I somehow lost my vigilance.
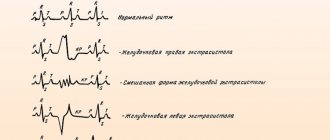
An electrocardiogram revealed a picture of voltage extrasystole. With this cardiac pathology, the normal systole (that is, contraction of the heart or its parts) is followed by an additional one. A sort of "upstart". This is the extrasystole. And after it there usually comes a compensatory pause. Longer, since after the extrasystole the next heartbeat falls out.
By palpation (when feeling the pulse in the arm or neck), I began to feel extrasystole even, it would seem, with light physical activity. For example, with a slight acceleration in walking or slowly climbing the stairs to the second floor.
“Well, unfortunate experimenter, “bright” popularizer of Buteykov’s ideas,” I lynch myself, “wasn’t the epic with atrial fibrillation enough for you? Now fight the extrasystolic!”
Systolic conductor and trainer
I again used almost the entire arsenal of tools involved in the treatment of atrial fibrillation, but I adjusted and added some things.
Hawthorn was included in herbal medicine, the antiarrhythmic properties of which have been known since the time of the ancient Roman physician Dioscorides (1st century AD). In the summer in the village I relied heavily on strawberries, which are also useful for extrasystole.
And now I want to share with you my main cardio-motor discovery, which, I dare to hope, may be useful to other “extrasystolics.” Judge for yourself. For the first time in the drug-free treatment of our illness, the “unhinged” heart will be assigned - no more, no less - conducting and even coaching functions. “Fantastic,” you say. No, it’s a completely feasible reality.
I'll explain now. But first, keep a close eye on my right hand. I feel the pulse in my neck or left arm (it’s great that there are no extrasystoles yet!). And now, solo accompanied by the newly-minted “systolic drummer”, who performs his part in a precise, strict metronome rhythm, I begin to perform simple movements. (Movements are synchronized with the rhythm of the heartbeat.) Banal coaching commands such as: “Start”, “Finish the exercise”, “That’s enough”, “Stop”, etc. - let the “naughty boy” himself serve - until the very first extrasystole.
1. My favorite and very effective exercise. Starting position – standing still, knees slightly bent. I rise high on my toes, stretching myself upward, and then energetically lower myself onto my heels in the metronomic mode set by the “magnificent conductor,” slightly bending my knees. In this way, I send the blood from my legs to my heart with shock. Portion after portion! Rigorously rhythmic! By blocking the spontaneous generation of extrasystole and mercilessly destroying it “in the bud”!
2. Walking on level ground.
3. Shallow half-squats in place.
4. Walking on negligibly rough terrain, carefully overcoming a short, several-degree slope and descending from it.
5. Standing, legs apart, left hand moved to the side (the right hand is on the pulse!). Turns the body left and right.
6. Standing, legs apart. Bend forward.
7. Lying on your back. Pedaling (“bicycle”).
Other simple exercises performed in the correct sinus rhythm will also work.
In his motor-respiratory therapy based on Buteykov’s principles, he limited himself to using the first two algorithms: 3+6+6+3 and 3+6+6+6.
I decipher the first algorithm: 3 steps - full inhalation, 6 steps - pause (breath holding), another 6 steps - full exhalation and then 3 steps - pause.
The second algorithm is more difficult. Here the final pause is extended to 6 steps. Therefore, I switched to it only after mastering—without extrasystole—the first algorithm.
Biysk doctor V. Durymanov also successfully used the method of intermittent (portional) breathing in therapeutic walking. The combination of such breathing and steps looked like this.
A short intermittent (but ultimately full diaphragmatic-thoracic) inhalation through the nose was done in three steps, and an accentuated, complete exhalation (“so that the stomach sticks to the back”) through a slightly open mouth in four. Pauses during and after inhalation and exhalation were filled with three walking steps. Schematically, the entire algorithm of intermittent breathing can be represented as follows: 1/3 inhalation + 3 pause steps + 1/3 inhalation + 3 pause steps + 1/3 inhalation + 3 pause steps + 1/4 exhalation + 3 pause steps + 1/4 exhalation + 3 steps pause + 1/4 exhale + 3 steps pause + 1/4 exhale + 3 steps pause, etc.
Six months later, I again reached my usual level of physical activity. I no longer needed to keep my finger on the pulse when doing exercises or warm-ups, since I first tested each exercise “for strength.” It should not have provoked the appearance of extrasystole either by the pace of movements or by the magnitude of physical effort.
Extrasystoles lying on your back
Saratov State Medical University named after. IN AND. Razumovsky (SSMU, media)
Level of education - Specialist
1990 - Ryazan Medical Institute named after Academician I.P. Pavlova
Extrasystole can occur with any cardiac pathology.
But almost half of such arrhythmias are caused by psycho-emotional overload, vegetative-vascular disorders, reflex effects from internal organs, taking certain medications, electrolyte imbalance, and drinking tonic drinks. It is to this half that the causes of resting extrasystole usually refer.
Types of extrasystole
Extrasystole is a change in heart rhythm caused by extraordinary electrical impulses.
They form in an additional focus of increased activity during diastole and affect the functional homogeneity of the myocardium.
In the absence of cardiac pathologies, the appearance of extraordinary electrical signals (extrasystoles) can provoke increased tone of the vagus or sympathetic nerve.
In this regard, sympathetic and vagal (bradycardic) extrasystoles are distinguished. Vagal symptoms appear at rest, often after meals and against the background of bradycardia, and disappear after exercise. Sympathetic extraordinary impulses, on the contrary, are formed during sports and other physical activities and disappear at rest.
In addition, extrasystoles are classified:
- According to the localization of the ectopic focus of increased activity:
- atrial;
- antrioventricular;
- ventricular;
- rare (no more than five per minute);
- frequent;
- For reasons of occurrence:
- organic;
- functional;
The impact of extrasystole on cardiac activity is largely characterized by the frequency of extraordinary impulses, the localization of the ectopic focus and the characteristics of heart disease.
Reasons for the development of extrasystole at rest
Experts note the influence of increased vagus nerve tone on the development of supraventricular extrasystoles. Vagal influences (reflexes) affecting the functionality of the heart usually arise when:
- axial hernia of the esophagogastric opening in the diaphragm;
- deformations of the walls of the esophagus;
- reflux of stomach contents into the esophagus;
- gastric pneumatosis;
- bloating;
- obesity;
- constipation;
- difficulties in moving food through the gastrointestinal tract;
- gallstones;
- prostate adenoma;
- fibroids of the uterus.
In patients with an unknown etiology of extrasystole, it is necessary to examine the organs located in the abdominal cavity. In addition, reflex extrasystole (extraordinary impulses caused by reflexes) can be provoked by pathological processes in the mediastinum and lungs, and cervical spondyloarthrosis. Sometimes pathological reflexes cause pockets of infection.
Extraordinary impulses that are formed when exposed to small dilated areas of the internal carotid arteries, during prolonged coughing, during the process of swallowing, when lying down and with certain pathologies of the brain, are also considered reflex.
Symptoms of vagal extrasystole
The manifestations of vagal extrasystole are influenced by many circumstances, in particular: individual irritability, contractile function of the heart, normal rhythm frequency and the level of prematureness of extraordinary impulses.
The main sign of the occurrence of extraordinary electrical signals against the background of bradycardic heart rhythm disturbances is a decrease in the heart rate. It is often combined with pressure surges.
During physical activity, the symptoms of extrasystole almost do not appear, they are noticeable only at rest - the more clearly, the less often the heartbeat.
The patient feels as if something like a bag of air is interfering with the normal functioning of the heart, especially when lying on the left side. Observed:
- interruptions in heart rhythm;
- fatigue;
- dizziness;
- a feeling of tightness or retrosternal raw pain;
- decreased muscle tone;
- panic attacks;
- lack of air.
Increased tone of the vagus nerve is expressed by:
- low heart rate (40-60 per minute);
- increased heart rate when inhaling;
- predisposition to hypotension;
- disruptions in the functioning of the vegetative-vascular system (“marbling” and cyanosis of the extremities, cold sweat in the area of the feet and palms, spontaneous urticaria).
The presence of vagal extrasystole is indicated by:
- an increase in the number of extraordinary impulses when reflexes act on the vagus nerve;
- a decrease in the number of extrasystoles or their disappearance when changing body position or after performing several physical exercises;
- reducing the number of extraordinary impulses or eliminating them after the administration of atropine.
Diagnosis and therapy of resting extrasystole
Diagnosis of reflex extrasystole often causes difficulties. An unambiguous diagnosis is made if extraordinary impulses disappear after the elimination of negative stimulation.
Complicating the situation is the fact that the manifestations of the reflex form of extrasystole are influenced by the unstable functioning of the autonomic nervous system. In addition, reflexes are sometimes involved in the formation or acceleration of extraordinary electrical signals in organic cardiac lesions.
Such circumstances make differentiated diagnosis of organic and reflex extrasystole practically impossible. An accurate diagnosis is made retrospectively.
Treatment of vagal extrasystole
If there are cardiac pathologies, the patient is prescribed appropriate medications.
Antiarrhythmic drugs have very serious side effects, so they can only be used as prescribed by a specialist and in recommended dosages.
For bradycardia, Diltiazem, Panangin, Carbamazepine are indicated, for surges in blood pressure - Bisoprolol, Atenolol, Metoprolol, for more severe pathology - Amiodarone, Propafenone.
If the symptoms of extrasystole cause physical suffering to the patient in the absence of cardiovascular pathologies, before prescribing medications, he is usually recommended to reconsider his lifestyle while taking mild sedatives. Often the cause of extrasystoles lies in the body’s reflex response to functional failures, so the patient needs to:
- normalize nutrition (constipation, flatulence cause an increase in the level of the diaphragm);
- control body weight (squeezing the diaphragm causes corresponding reflexes);
- cleanse the gallbladder and liver (a bladder overfilled with bile provokes reflex activity of the vagus nerve).
Extrasystoles subject to therapy
Sometimes, even in the absence of heart disease, extraordinary electrical impulses can significantly affect the performance of the body.
Frequent contractions of the heart, reducing blood output per unit time, can cause loss of consciousness with the subsequent development of angina. Atrial extrasystoles provoke atrial fibrillation.
Frequent multifocal volley ventricular impulses can bring the greatest trouble - they can portend the development of ventricular fibrillation.
Signs of dangerous heart pathologies are often those that appear in a lying position:
- allorhythmia (an extraordinary impulse occurs regularly after several normal heart contractions);
- polytopic extrasystoles (extraordinary impulses are formed in different foci);
- volley impulses (over five per minute);
- extraordinary impulses that occur after atrial fibrillation (with any irritation, the flickering may return).
These conditions require mandatory preventive therapy.
Folk recipes
The list of folk remedies for the treatment of vagal extrasystole is quite large. But they are applicable only as auxiliary methods as part of complex treatment. After consulting with a specialist, you can use “grandmother’s” recipes:
- Hawthorn – use dried flowers as tea leaves (a tablespoon per 200 ml of boiling water). Drink three glasses every day. You can prepare a tincture: per tablespoon of flowers - 200 ml of vodka. After leaving for 10 days in a dark place, drink a teaspoon three times a day;
- Calendula - pour a teaspoon of flowers into a glass of boiling water, let it brew, strain. Drink 100 ml four times a day;
- Horsetail - pour a tablespoon of horsetail into 600 ml of boiling water, leave for three hours. Strain, drink a tablespoon six times a day;
- Cornflower - add a teaspoon of dried flowers to 200 ml of boiling water and leave. Strain, drink on an empty stomach three times a day;
- Lumbago – add two teaspoons of dried flowers to 200 ml of boiling water and let it brew. Drink a third of a glass three times a day;
- Honey and chopped radish - mix in equal proportions, drink a tablespoon three times a day.
For the most part, patients with extrasystole do not need antiarrhythmic treatment. The reticence of specialists when prescribing rhythm stabilizers is understandable: complications associated with their use are often more dangerous than manifestations of extraordinary impulses.
Causes of extrasystole in a horizontal position
Extrasystole is one of the types of cardiac arrhythmia, which is characterized by the appearance of one or more extraordinary contractions of the myocardium.
Extrasystole, the symptoms of which can be observed not only in patients, but also in healthy people, is often caused by psychological overstrain, stress, and overwork. In this case, when the above reasons are eliminated, the heart condition returns to normal and drug treatment of the disease is not required.
With functional extrasystole, most patients do not notice it during the daytime. They exhibit extrasystole in the supine position, and extrasystole is possible before bedtime. You can learn more about what extrasystole is, symptoms, and treatment of this disease from our articles.
What is extrasystole: is it dangerous, its symptoms and treatment.
A normal heart rhythm ensures blood supply to all organs and tissues of the human body. Violation of the uniformity of impacts will lead to pathology of hemodynamics (peculiarities of blood movement).
There must be intervals between contractions of the heart muscle (diastolic intervals), during which blood enters the ventricles and atria. When the duration of pauses decreases, the chambers are not completely filled and during systolic contraction a reduced physiological volume of fluid enters the circulation.
Such hemodynamic disorders are provoked by extrasystoles.
Symptoms and causes of extrasystole
This ailment, extrasystole, is the most common of all existing types of arrhythmia, because improper functioning of the spine (osteochondrosis) can radiate to the heart area. There are a certain number of symptoms that indicate that a person’s health is in danger:
- The patient feels a jolt in the area of the heart, or feels as if it is freezing;
- Short-term fainting;
- A painful sensation in the area of the shoulder blades (between them), after which there is a sharp push in the chest (like a somersault);
- Difficulty breathing, feeling of anxiety;
- Increased sweating, constantly feeling hot;
- When measuring the pulse during extrasystole, a gap or a wave of beats may be observed (this indicates insufficient filling of the ventricles).
If the disease is acute, the patient feels a sharp pain in the neck, which goes down the shoulder to the tips of the fingers, and may also feel dizzy.
The reasons why a person can get extrasystole with osteochondrosis are different. The most basic of which is squeezing or compression of the vertebral artery, which is located along the spine. Another common cause of extrasystole is a heavy load on the spine itself, after which its proper functioning is disrupted. Less common causes of the disease are stress and pinched nerve endings in that area.
What are extrasystoles and do they pose a danger to life?
Extrasystoles are premature excitations of the myocardium, which lead to its extraordinary contraction. In this case, activation of the entire heart muscle or its individual parts is possible.
In a healthy person, when recording an ECG (electrocardiogram) around the clock, there is a 50% chance that extrasystoles will be recorded. They are isolated, occur very rarely, have no clinical manifestations and are not dangerous.
However, if extrasystoles follow each other, this can lead to irreversible hemodynamic disturbances due to a decrease in the pumping activity of the left ventricle.
Prognostic classification of extrasystoles (JT Bigger):
Diagnosis of the disease and methods of treatment
Treatment is prescribed by the doctor based on determining the form of the extrasystole disease. If it is mild, then medication treatment is not prescribed, although it cannot be ignored. It is worth undergoing a full examination in order to eliminate all causes that may affect the further development of the disease. After all, it is known that a mild form can easily develop into a more complex one.
If the patient has a number of extrasystoles exceeding 700 beats per day, it is necessary to prescribe effective treatment. If you feel severe chest pain, you should consult a cardiologist. In due time, the doctor must listen to the patient’s complaints and conduct a special diagnosis. The first thing the doctor should do is measure your blood pressure, listen to your heart and prescribe blood and urine tests. Next you need to send for an ECHO and ECG. In order to measure the frequency of extrasystoles, Holter monitoring is prescribed to the patient. This technique takes longer, but it shows the rate of contraction of the human heart. Ultrasound and MRI are required.
For many, going to see a doctor is a serious move, so there are also folk remedies for curing the disease, but remember that self-medication can lead to serious consequences. The most important thing is to get advice from an experienced specialist and accurately determine the causes of extrasystole.
What are the symptoms of the pathology
Symptoms of extrasystole are:
- periodic sensation of heartbeat;
- freezing in the chest;
- feeling that the heartbeat is arrhythmic;
- lack of air due to chest discomfort;
- failure of breathing rhythm;
- syncope (temporary loss of consciousness).
The occurrence of extrasystoles in the supine position
If the sensation of a change in the functioning of the myocardium manifests itself in the supine position, this indicates the functional nature of the extrasystoles that occur. Symptoms disappear when moving to a sitting position, the pulse becomes rhythmic. This arrhythmia does not pose a danger to the body. In this case, standard drug therapy will be ineffective; taking sedatives will be an effective solution.
Extrasystoles occur in the heart as a result of structural or functional changes in the myocardium. They may be due to:
- heart disease (angina pectoris, heart defects, cardiomyopathies, myocarditis, cardiomyofibrosis, heart failure);
- disturbances of electrolyte (hypokalemia, hyperkalemia, hypomagnesemia, hypocalcemia) or acid-base balance;
- hypoxia (due to chronic lung diseases);
- chronically high or low blood pressure;
- injuries (chest, brain and spinal cord);
- manipulations on the heart (surgical and diagnostic interventions);
- dysfunctions of the autonomic nervous system (structural changes, VSD (vegetative-vascular dystonia), lack of sleep, stress and neuroses);
- hormonal imbalance during menopause (estrogens deficiency);
- immaturity of the cardiac conduction system in newborns;
- psycho-emotional stress and constant training in athletes (extraordinary contractions occur against the background of bradycardia);
- redistribution of blood flow and changes in hormonal levels during pregnancy;
- activation of pathological reflexes due to: diseases of the digestive system (pancreatitis, ulcers, cholelithiasis, enterocolitis, severe flatulence);
- pathologies of the cervical and thoracic spine (spondyloarthrosis, osteochondrosis);
- diseases of the bronchopulmonary system (with a strong prolonged cough);
- prostate adenomas;
- endoscopic examinations (bronchoscopy, laparoscopy, gastroscopy, cystoscopy, colposcopy, sigmoidoscopy);
- toxic effects of drugs:
The described factors contribute to the disruption of the functional and structural integrity of the impulse pathways in the myocardium. Instead of a clear directional movement (from the atrium to the ventricle), the wave of depolarization in a circle returns to the starting point, as a result of which the contraction mechanism is restarted and an extraordinary heart beat occurs.
Another mechanism for the occurrence of extraordinary contractions is the presence of ectopic (abnormal) sources of impulse generation. Activating asynchronously with the sinus node (the main pacemaker), they trigger an extraordinary contraction of the myocardium.
Diagnosis and therapy of resting extrasystole
Diagnosis of reflex extrasystole often causes difficulties. An unambiguous diagnosis is made if extraordinary impulses disappear after the elimination of negative stimulation. Complicating the situation is the fact that the manifestations of the reflex form of extrasystole are influenced by the unstable functioning of the autonomic nervous system. In addition, reflexes are sometimes involved in the formation or acceleration of extraordinary electrical signals in organic cardiac lesions. Such circumstances make differentiated diagnosis of organic and reflex extrasystole practically impossible. An accurate diagnosis is made retrospectively.
Treatment of vagal extrasystole
If there are cardiac pathologies, the patient is prescribed appropriate medications. Antiarrhythmic drugs have very serious side effects, so they can only be used as prescribed by a specialist and in recommended dosages. For bradycardia, Diltiazem, Panangin, Carbamazepine are indicated, for surges in blood pressure - Bisoprolol, Atenolol, Metoprolol, for more severe pathology - Amiodarone, Propafenone.
If the symptoms of extrasystole cause physical suffering to the patient in the absence of cardiovascular pathologies, before prescribing medications, he is usually recommended to reconsider his lifestyle while taking mild sedatives. Often the cause of extrasystoles lies in the body’s reflex response to functional failures, so the patient needs to:
- normalize nutrition (constipation, flatulence cause an increase in the level of the diaphragm);
- control body weight (squeezing the diaphragm causes corresponding reflexes);
- cleanse the gallbladder and liver (a bladder overfilled with bile provokes reflex activity of the vagus nerve).
Extrasystoles subject to therapy
Sometimes, even in the absence of heart disease, extraordinary electrical impulses can significantly affect the performance of the body. Frequent contractions of the heart, reducing blood output per unit time, can cause loss of consciousness with the subsequent development of angina. Atrial extrasystoles provoke atrial fibrillation. Frequent multifocal volley ventricular impulses can bring the greatest trouble - they can portend the development of ventricular fibrillation.
Signs of dangerous heart pathologies are often those that appear in a lying position:
- allorhythmia (an extraordinary impulse occurs regularly after several normal heart contractions);
- polytopic extrasystoles (extraordinary impulses are formed in different foci);
- volley impulses (over five per minute);
- extraordinary impulses that occur after atrial fibrillation (with any irritation, the flickering may return).
These conditions require mandatory preventive therapy.
Group extrasystoles at night
Hello! Nighttime (from 21:00 to 8:00 a.m.) extrasystoles are disturbing, mainly in the supine position. They start one at a time, then in pairs, then in groups and go away after a vertical position in a few minutes. The es-ly first appeared four years ago, I suffered for a year. I have a long-standing bouquet from a 12-pc ulcer, duodenitis, multiple gall bladder polyps. Then examinations in the heart, ECG, Holter, did not catch the es. All kinds of medications (de Nol, Nolpaza, Omez, magnesium) did not give any effect. I also received treatment from a psychotherapist on the advice of a cardiologist, took antidepressants for six months, to no avail. The antiarrhythmic drug was helpful, only instead of extrasystoles there was pain in the heart. The gastroeterologist advised me to remove the gallbladder; on her advice, I started taking duspatalin, and the es decreased. Then I had an FGD in a normal clinic, they found hemorrhagic erosive multiple gastritis, duodenitis, and bile reflux. Intuitively, based on an advertisement, I took phosphalugel, and for the first night in a year I slept peacefully. Then the es began to appear sporadically and not for long, I finished them off with Iberogast. For three years there were almost no extrasystoles. At the beginning of November, nighttime extrasystoles began to appear again, and I immediately ran to the FGDS. They found duodenitis and reflux. The doctor prescribed Trimedat, to no avail. Again I found the panacea, Gaviscon, and took it off as if by hand. at the end of January they began to hammer again, Gaviscon no longer helped, the attacks became longer and more unbearable with pain in the heart and dizziness. I fell ill with a sore throat, they prescribed the antibiotic sumamed, and while I had a fever and took sumamed, there was not a single one. A week later, everything resumed with terrible force, I already wake up at night, so I sleep reclining. nothing helps, the list of tried medications is long. Logic dictates taking an antibiotic against Helicobacter, but how much can you poison the body, and I don’t remember if I drank them, I think I drank them three years ago and they didn’t help. What should I do - continue to undergo treatment at random, or is my heart already starting to skip due to nervousness (by the way, there is something)?
Causes of extrasystole in a horizontal position
Extrasystole is one of the types of cardiac arrhythmia, which is characterized by the appearance of one or more extraordinary contractions of the myocardium.
Extrasystole, the symptoms of which can be observed not only in patients, but also in healthy people, is often caused by psychological overstrain, stress, and overwork. In this case, when the above reasons are eliminated, the heart condition returns to normal and drug treatment of the disease is not required.
With functional extrasystole, most patients do not notice it during the daytime. They exhibit extrasystole in the supine position, and extrasystole is possible before bedtime. You can learn more about what extrasystole is, symptoms, and treatment of this disease from our articles.
How to get rid of extrasystole and remove its manifestations
Extrasystole does not occur on its own. It is a manifestation of pathological processes occurring in the myocardium or other organs.
To get rid of arrhythmia you need to:
- Find a specialist to assess the risk and draw up a treatment program.
- Carry out lifestyle corrections, quitting smoking, alcohol, coffee and strong tea;
- healthy food;
- adequate physical activity;
- minimizing stress factors.
Clinical symptoms and treatment of extrasystole are directly related: the more serious the changes in the patient’s condition, the more radical therapy he will need.
Clinical signs of extrasystole
It is known that the clinical signs of extrasystole largely depend on its type. Below are the symptoms of the main types of extrasystoles.
Ventricular extrasystole is characterized by a feeling of interruptions in the functioning of the heart muscle. It seems to the patient that the heart seems to turn over, then stops (which is caused by a pause after the extrasystole), and then a push occurs and the heart works normally again.
With frequent extrasystole, tachycardia may develop. Physically, the patient feels weak, anxious, dizzy, sweats heavily, and may lose consciousness.
If such symptoms occur for the first time or the patient does not tolerate attacks of extrasystole, then it is necessary to urgently consult a doctor (especially if tachycardia develops and the heart rate exceeds 100 beats per minute).
Ventricular extrasystole can occur during coughing attacks, swallowing, in a certain position of the body (extrasystole, lying on the left side), and brain diseases.
If there is organic damage to the heart, then clinical signs of the underlying pathology are added to the extrasystole (swelling and shortness of breath with heart failure, heart pain with ischemic heart disease, and so on). If ventricular fibrillation develops, the patient is declared clinically dead.
Single atrial extrasystoles do not manifest themselves clinically, therefore they are usually detected by chance during an ECG. The patient feels frequent atrial extrasystoles as interruptions in the functioning of the heart. First, he feels the heart stop, then a strong beat follows, then stops again, and so on. This causes the patient to fear death. Other symptoms of the disease are shortness of breath, darkening of the eyes, and dizziness. If such symptoms appear, you should immediately consult a doctor.
It is possible to distinguish atrial and ventricular extrasystole from each other only with the help of an ECG. Under no circumstances should you select medications against arrhythmia on your own. This will not bring any effect, but on the contrary can cause the development of a number of serious complications, including death.
Extrasystole can be not only an independent pathology, but also a symptom of a number of diseases, including VSD.
In this case, the main symptoms are irritability, anxiety, fear of death, panic attacks and other nervous system disorders.
Patients complain of hot flashes, suffocation, discomfort and general weakness, and sweat profusely.
Extrasystole during VSD is most often functional in nature, and therefore does not require special treatment. Patients need to consult a psychotherapist; for severe attacks, light sedatives may be used.
Extrasystole - treatment
It is necessary to eliminate provoking factors and treat the underlying disease. Single extrasystoles without clinical manifestations are not treated.
Neurogenic extrasystoles are treated by establishing a work-rest regime, giving dietary recommendations, regular exercise is useful, psychotherapy, tranquilizers or sedatives (for example, tincture of valerian) are used. Self-administration of drugs, self-medication using various methods is extremely undesirable and unsafe, as it can be life-threatening if the nature, mechanisms and causes of extrasystoles are not determined.
The choice of treatment method for extrasystole is made by a specialist, taking into account the clinical picture of the disease, data from instrumental diagnostic studies and current Russian and European recommendations.
By taking antiarrhythmic drugs, extrasystoles can be eliminated, but after discontinuation of the drugs, extrasystoles resume. In addition, the most important thing: in people with organic heart disease, against the background of effective treatment of extrasystole with antiarrhythmic drugs, an increase in mortality of more than 3 times was revealed! There was no increased risk of mortality observed with beta blockers or amiodarone alone. However, a number of patients experienced complications, including life-threatening ones. The effectiveness and safety of using potassium and magnesium preparations or the so-called. "metabolic" drugs have not been definitively established.
A fairly radical and effective method of treating extrasystole is catheter ablation (“cauterization”) of the focus of extrasystole. The operation, on average, is performed within 45-55 minutes, and after a day the patient can be discharged from the hospital.
Diagnosis of extrasystole
To diagnose extrasystole, the doctor first conducts a survey and examination of the patient. The specialist is interested in what the patient is complaining about, how often he feels interruptions in the heart, what time of day they usually appear, whether the patient has previously suffered myocardial diseases, and so on.
The information obtained helps the doctor determine the degree and shape of extrasystole, the sequence of extrasystole in comparison with normal heart contractions. After making a preliminary diagnosis, the doctor prescribes a series of laboratory and instrumental studies.
Tests for extrasystole:
- blood test (biochemical and general);
- blood test for thyroid hormones.
Based on the research results, an extracardiac cause of extrasystole can be identified. The main method for diagnosing extrasystole is ECG.
Extrasystole after eating
Another type of cardiac arrhythmia is extrasystole after eating. Most often, a person feels a sinking heart for a couple of seconds, and then a short spasm and a jolt are felt in the chest.
Extrasystole after eating is also a functional form, which depends on the individual characteristics of the body. In most cases, it is considered safe for a healthy person, and since it does not lead to any complications in the functionality of the heart, drug treatment is most often not prescribed.
The reasons for extrasystole after eating can be different - for some people it occurs after eating fast food, for others, heart failure is associated with eating food rich in sodium.
It is quite difficult to determine the specific cause, but we can say how the process of extrasystole occurring after eating occurs:
- after eating food, it enters the gastrointestinal tract, where it undergoes digestion, and this process involves oxygen, which enters the gastrointestinal tract with the blood;
- a large volume of blood is sent to the digestive tract so that there is more oxygen in it;
- the heart muscle experiences a lack of oxygen and contracts more often. This phenomenon is explained by the fact that the heart tries to push more blood through itself in order to restore the lost balance.
Extrasystole on ECG
Signs of extrasystole on an ECG depend on its type. Ventricular extrasystole, the diagnosis of which is extremely important, is defined as follows.
ECG signs of ventricular extrasystole:
- increased duration and deformation of the QRS complex;
- formation of an asymmetric T wave and displacement of the ST segment below or above the isoline;
- complete compensatory pause (may be absent if ventricular extrasystole develops against the background of atrial fibrillation).
ECG signs of atrial extrasystole:
- extraordinary appearance of the P wave, followed by a normal QRS complex;
- the ventricular complex does not change;
- the compensatory pause is incomplete.
In addition to the standard ECG, Holter monitoring can be used to diagnose extrasystole, when the patient carries a portable ECG device with him for a day.
Sincerely, Alexander Yurievich.
Do not be shy. I will help with all I can!
In-person consultation is possible for Kharkov residents and those who can come to Kharkov.
Extrasystoles are called premature excitation of the entire heart or any of its parts relative to the main rhythm.
1) By localization: sinus, atrial, atrioventricular, ventricular.
2) By time of occurrence: early, middle, late.
3) According to the frequency of occurrence: sporadic, allorhythmia (bi-, trigemeny).
4) By sources of occurrence: monotopic, polytopic.
5) In appearance: monomorphic, polymorphic.
Diagnostics
SVES is diagnosed using resting electrocardiography (ECG) and 24-hour Holter ECG monitoring.
Atrial extrasystole is characterized by the premature appearance of an altered P wave, reflecting excitation of the atria from an ectopic focus. It is most often followed by a normal or slightly deformed ventricular complex. Sometimes ventricular contraction does not occur, in which case they speak of blocked SVES. After an atrial extrasystole, an incomplete compensatory pause is usually recorded. This means that the distance between two adjacent beats is less than twice the distance between two normal sinus beats. If the ectopic focus is located in the atrioventricular junction, a premature, unchanged ventricular complex is recorded on the ECG. The P wave is not detected. In other cases, excitation is carried out retrogradely to the atria, so a negative P wave appears after the extrasystolic ventricular complex.
When analyzing 24-hour Holter ECG monitoring, the functional diagnostics physician determines the total number of SVES, clarifies their topic (source), and identifies paired and group SVES. This study provides information about the distribution of extrasystoles over time, their relationship with heart rate, sleep period, physical activity and medication use. Therefore, daily ECG monitoring is an important part of the patient’s examination.
Therapy for the underlying disease is prescribed.
The patient is advised to stop drinking coffee, strong tea, alcohol, and avoid smoking. He shouldn't overeat. It is necessary to increase the potassium content in the diet. You need good sleep and a favorable psychological environment at work and at home.
It is recommended to take herbal sedatives: valerian, motherwort, Zelenin drops. If extrasystole is not associated with heart disease and appears at rest, anticholinergic drugs can be used, in particular, drugs containing belladonna. When it appears against the background of exercise, beta-blockers help.
For organic supraventricular extrasystole, beta-blockers are the drugs of choice. If they are ineffective, verapamil and kinylentine can be used. In case of concomitant circulatory failure, indications for the use of cardiac glycosides are considered.
If there is no effect, you can use drugs that are effective for both supraventricular and ventricular extrasystole. These include amiodarone, disopyramide, allapinin, rhythmonorm and others.
Certain types of extrasystoles
1) an extraordinary P wave is observed on the ECG, which differs in shape and sometimes in polarity from sinus waves;
2) a normal (sometimes aberrant) QRS complex is observed along the P wave;
3) PQ interval from 0.12 to 0.2 s;
4) incomplete compensatory pause.
a) neurogenic: hyperadrenergic (psychogenic), hypoadrenergic (extrasystoles of alcoholics, athletes), vagal (occur during sleep, in a horizontal position, due to damage to the gastrointestinal tract);
b) extrasystoles of asthenics;
c) extrasystoles with hypokalemia;
e) tonsillogenic myocardial dystrophy;
e) sometimes occur in healthy people.
2. Organic origin:
IHD, myocarditis, cardiomyopathies, heart defects, mitral valve prolapse, alcoholic heart disease, cor pulmonale, etc.
In most cases, no treatment is required.
With hyperadrenergic type
They recommend limiting emotional and physical stress, eliminating coffee and alcohol from the diet. Taking into account all contraindications, β-blockers are prescribed (propranolol 20 mg 3 times a day). Verapamil 40 mg 3 times a day can be quite effective.
For vagal type:
normalization of nutrition. Prescribe belloid - 1 tablet. 2-3 times a day for a month or 1 tablet. 1-2 times a day. In all cases, normalization of potassium levels in the blood plasma. In resistant cases, short-term administration of class IA drugs is possible.
Folk recipes
The list of folk remedies for the treatment of vagal extrasystole is quite large. But they are applicable only as auxiliary methods as part of complex treatment. After consulting with a specialist, you can use “grandmother’s” recipes:
- Hawthorn – use dried flowers as tea leaves (a tablespoon per 200 ml of boiling water). Drink three glasses every day. You can prepare a tincture: per tablespoon of flowers - 200 ml of vodka. After leaving for 10 days in a dark place, drink a teaspoon three times a day;
- Calendula - pour a teaspoon of flowers into a glass of boiling water, let it brew, strain. Drink 100 ml four times a day;
- Horsetail - pour a tablespoon of horsetail into 600 ml of boiling water, leave for three hours. Strain, drink a tablespoon six times a day;
- Cornflower - add a teaspoon of dried flowers to 200 ml of boiling water and leave. Strain, drink on an empty stomach three times a day;
- Lumbago – add two teaspoons of dried flowers to 200 ml of boiling water and let it brew. Drink a third of a glass three times a day;
- Honey and chopped radish - mix in equal proportions, drink a tablespoon three times a day.
Read also: Severe sinus bradycardia
For the most part, patients with extrasystole do not need antiarrhythmic treatment. The reticence of specialists when prescribing rhythm stabilizers is understandable: complications associated with their use are often more dangerous than manifestations of extraordinary impulses.
Supraventricular extrasystole: causes, signs, treatment
Supraventricular, or supraventricular, extrasystoles (SVES) are premature contractions of the heart caused by the extraordinary formation of an impulse in areas of the atrial conduction system located below the sinus node.
In this case, an ectopic focus is formed in the wall of one of the atria, generating premature electrical impulses. They cause contraction of the atria and then the ventricles. After the extrasystole, normal sinus rhythm resumes.
SVES make up about a third of all extrasystoles. They are divided into extrasystoles from the atrioventricular junction and from the atrium (atrial). Atrial extrasystoles make up the majority of supraventricular ones. Both atrial and extrasystoles from the atrioventricular junction have the same causes and mechanisms of development. Their treatment tactics are also no different. Therefore, most often they talk about supraventricular extrasystole, without distinguishing between its individual types.
In approximately a third of cases, SVES is not accompanied by organic changes in the heart and is functional. They can also occur in healthy people. In this case, SVES is caused by autonomic disorders, often accompanied by a rare heartbeat, arterial hypotension, increased tone of the vagus nerve, in particular, sweating of the extremities.
SVES often appears with excessive consumption of tea, coffee, alcoholic beverages, and also with smoking. They can be triggered by emotional or physical stress, or changes in body position. With functional extrasystole during the daytime, patients often do not notice the arrhythmia. Extrasystoles begin to bother them in the evening, in a lying position, before bedtime.
SVES accompanies many heart diseases. Most often they are recorded in chronic ischemic heart disease (angina pectoris, post-infarction cardiosclerosis), as well as against the background of an active rheumatic process. The appearance of this arrhythmia is facilitated by enlargement of the atria and stretching of their walls, for example, with mitral stenosis. In this case, supraventricular extrasystole is subsequently replaced by atrial fibrillation.
SVES can occur during acute myocardial infarction and accompany the course of myocarditis, hypertension, and congenital heart defects. They occur in chronic cor pulmonale, pheochromocytoma (hormone-producing tumor of the adrenal gland), thyrotoxicosis, and menopausal myocardial dystrophy. In addition, SVES can be caused by hypokalemia, that is, a lack of potassium in the blood. In rare cases, they appear with an overdose of cardiac glycosides (digitalis intoxication).
SVES occur in acute and chronic infections, tonsillitis, as well as in chronic cholecystitis and other diseases of the abdominal organs.
Symptoms of vagal extrasystole
The manifestations of vagal extrasystole are influenced by many circumstances, in particular: individual irritability, contractile function of the heart, normal rhythm frequency and the level of prematureness of extraordinary impulses.
The main sign of the occurrence of extraordinary electrical signals against the background of bradycardic heart rhythm disturbances is a decrease in the heart rate. It is often combined with pressure surges. During physical activity, the symptoms of extrasystole almost do not appear, they are noticeable only at rest - the more clearly, the less often the heartbeat. The patient feels as if something like a bag of air is interfering with the normal functioning of the heart, especially when lying on the left side. Observed:
- interruptions in heart rhythm;
- fatigue;
- dizziness;
- a feeling of tightness or retrosternal raw pain;
- decreased muscle tone;
- panic attacks;
- lack of air.
Increased tone of the vagus nerve is expressed by:
- low heart rate (40-60 per minute);
- increased heart rate when inhaling;
- predisposition to hypotension;
- disruptions in the functioning of the vegetative-vascular system (“marbling” and cyanosis of the extremities, cold sweat in the area of the feet and palms, spontaneous urticaria).
Read also: Types of ventricular extrasystoles
The presence of vagal extrasystole is indicated by:
- an increase in the number of extraordinary impulses when reflexes act on the vagus nerve;
- a decrease in the number of extrasystoles or their disappearance when changing body position or after performing several physical exercises;
- reducing the number of extraordinary impulses or eliminating them after the administration of atropine.
Clinical signs
Complaints of patients with supraventricular extrasystole depend on many factors. It is believed that young people with functional extrasystole tolerate SVES worse. They may complain of various sensations in the chest and neck, reminiscent of turning over, “fish fluttering,” or freezing. In some cases, extrasystole is accompanied by dizziness and weakness.
If extrasystole occurs against the background of an organic heart disease, it is often not felt, patients get used to it and do not pay attention to it. Complaints are mainly due to the underlying disease.
Can there be extrasystole with osteochondrosis?
More and more often, people with sharp pain in the chest area come to see a doctor with symptoms of pain that are not relieved by taking medications. Extrasystole in osteochondrosis is similar to a pathological disorder of the heart, and it is not detected by the hardware method. The first thing the patient pays attention to is an irregular heart rhythm and poor general condition. Feeling dizzy, sweating, chest pain. Doctors say that the disease is not dangerous, and if you notice small and infrequent abnormalities in the heart area, do not worry. But as practice shows, at the first symptoms, you should immediately contact a specialist.