Increased pressure in the blood vessels of the lungs or pulmonary hypertension is diagnosed in people of different age categories. For various reasons, a barely born baby may also be susceptible to this pathology.
In this case, we are talking about pulmonary hypertension in newborns, also known as persistent or persistent fetal circulation in the newborn (ICD-10 code P29.3).
Description and statistics
Persistent fetal circulation in a newborn is a kind of signal from the baby’s body about the impossibility of fully adapting the blood circulation in the lungs to life outside the womb.
In the prenatal period of development, the lungs undergo a number of changes that prepare them for functioning in the air, but at this time the placenta “breathes” for them. After the birth of a child, “real” breathing should begin , but sometimes for a number of reasons it occurs with pathology.
With pulmonary hypertension, there is a sharp jump in pressure inside the vascular bed of the lungs, as a result of which the child’s heart begins to experience enormous stress.
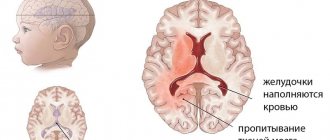
The newborn’s body, trying to avoid impending heart failure, produces an emergency decrease in pressure in the lungs by reducing the volume of blood circulating in them - the blood is “dumped” through the open foramen ovale in the heart or the open ductus arteriosus that babies have.
This in turn leads to an increase in the amount of venous blood in the general bloodstream, a decreased oxygen content in the blood and cyanosis in the child.
According to statistics, the pathology occurs in 1-2 babies out of 1000 . Approximately 10% of newborns requiring intensive care suffer from this disease. Moreover, most of them are full-term or post-term babies.
Fetal circulatory syndrome occurs much more often in children born by cesarean section - in approximately 80-85% of cases.
The overwhelming number of relevant diagnoses (97%) were made in the first three days of life of small patients - such early diagnosis allows us to significantly reduce the number of deaths, since without timely medical care, 80% of sick children can die.
Arterial cardiac hypertension in newborns
One of the diseases of the vascular bed and heart in newborns is hypertension, called arterial hypertension. In medical practice, almost all cases of its occurrence are considered secondary by doctors. In other words, this pathology almost always develops against the background of some other disease.
In a full-term baby, this diagnosis is made when the systolic pressure level is objectively higher than 90, and the diastolic pressure level exceeds 60 mm Hg. Art. For babies born in a state of prematurity, these boundaries shift slightly and become equal to 80 and 50 mmHg, respectively. Art.
Based on scientific research data, we can say that in the vast majority (namely 70% or even more) of cases, the appearance of such an ailment as arterial hypertension in a newborn is dependent on one or another kidney pathology. This is mainly thrombosis of the renal artery, with a slightly lesser probability of congenital stenosis of the latter. Blood clotting disorders, septicemia and arrhythmias can be thrombus-forming factors.
The cause of increased pressure on the right upper limb may be coarctation of the aorta, incl. accompanied by hypoplasia of the aortic arch.
Parenchymal renal pathologies that can cause increased pressure include pyelonephritis, tumors, renal hypoplasia, and renal failure.
Hypertension in the arterial bed can also appear as a result of excessive blood transfusion.
With such a pathological condition as arterial hypertension in newborns, signs of the disease may be completely absent, which occurs in approximately a third of infants suffering from this disease. However, for the most part, manifestations still make themselves felt.
The clinical picture, as a rule, includes signs of dysfunction of the main body systems. First of all, this concerns the heart: the pulse changes, vasomotor instability is noted, cardiomegaly and contractile heart failure develop. Changes in the respiratory system are reduced to the appearance of cyanosis and shortness of breath. Tremor, asymmetry of reflexes and the occurrence of seizures indicate dysfunction of the central nervous system.
Once a diagnosis of arterial hypertension in newborns has been established, treatment should be aimed not only at bringing the pressure to the proper level, but also at eliminating the cause of its rise.
If mild hypertension occurs, then it is advisable to use diuretics (for example, hydrochlorothiazide) or ACE inhibitors (such as Captopril).
Rarely, surgery may be required. In this way they fight coarctation of the aorta or remove blood clots.
Children suffering from this disease must be closely monitored. The goal of the latter is timely treatment of relapses, as well as monitoring the functional state of the kidneys.
Causes and risk factors
In rare cases, the causes of pulmonary hypertension cannot be established - then the pathology is called primary or idiopathic. But most often the cause of an inadequate increase in pressure in the pulmonary vessels is:
- Prenatal stress in the form of hypoxia, hypoglycemia, hypocalcemia, aspiration of meconium or amniotic fluid. As a result of this, after birth, a spasm of the arterioles of the lungs may occur, followed by sclerotic changes in their walls.
- Delayed intrauterine maturation of vascular walls with partial preservation of their embryonic structure after birth. Such vessels are subject to spasms to a much greater extent.
- Congenital diaphragmatic hernia , in which the lungs in general and their vessels in particular are underdeveloped and cannot function normally.
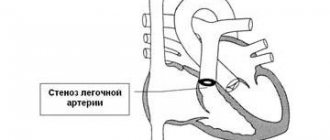
- Increased pulmonary blood flow in the fetus due to premature closure of the fetal ductus arteriosus and foramen ovale.
- Congenital heart and lung defects in a child: pulmonary hypoplasia, ventricular septal defects, transposition of the great vessels, etc. Another article describes a detailed classification of congenital heart defects.
Risk factors for this pathology are:
- intrauterine hypoxia;
- intrauterine infections or sepsis;
- unauthorized use by a pregnant woman of certain medications (non-steroidal anti-inflammatory drugs, antibiotics, aspirin;
- polycythemia in a newborn is an oncological disease in which the number of red blood cells in the blood increases significantly;
- congenital heart and lung defects in a child.
What is pulmonary hypertension
This pathology is a syndrome of a number of diseases united by a common feature. In pulmonary hypertension (PH), a narrowing of the lumen of the arteries is observed, provoked by the proliferation of endothelium - the cells lining their inner surface. This causes blockage of the capillaries and arterioles of the lungs. Pathology can also be caused by an increase in blood flow. This situation leads to:
- circulatory decompensation;
- increased systolic pressure in the artery of the respiratory organ;
- increased load on the heart;
- disruption of blood flow and gas exchange.
With the development of the disease, relative insufficiency of the pulmonary artery valve occurs, the work of the main cardiac muscle is weakened, and right ventricular overload occurs. Doctors, depending on the progression, distinguish four degrees of pathology. According to ICD-10 (International Classification of Diseases), the code is assigned only to the primary form - 127.0. An indicator of the presence of pathology is the parameter average MPAP (specific pressure in the organ), measured in millimeters of mercury (mmHg), which is:
- at rest – 25;
- at load – 35.
Primary
This form of the disease is rare and the exact mechanism of its development is unknown. Primary pulmonary or idiopathic pathology is characterized by persistent vascular resistance. When examined by echocardiography, the value of MPAP at rest exceeds 25 mm Hg. Art. The disease is diagnosed by exclusion:
- pathologies of the respiratory system, heart;
- tumors;
- chronic thromboembolism of an artery organ;
- structural features of the body.
Experts believe that the following factors can provoke idiopathic respiratory hypertension:
- autoimmune conditions;
- congenital pathologies of pulmonary capillaries in the fetus;
- hereditary causes;
- taking birth control pills;
- development of the atherosclerotic process in the branches of the artery;
- increased tone of the sympathetic nerve;
- vasculitis of organ vessels;
- herpes virus type eight.
Secondary
A disease is considered secondary if it develops as a result of chronic diseases of the heart, liver, etc. Under their influence, the walls of blood vessels thicken, the lumen of small arteries narrows, and spasms of arterioles occur, which causes a dangerous pathology. Secondary hypertension of this organ of varying severity is provoked by:
- Congenital heart defect;
- the occurrence of blood clots;
- structural defects of the chest and spine;
- neoplasms of the heart, respiratory organs;
- chronic inflammation - liver cirrhosis, pneumosclerosis, tuberculosis.
Types and stages of the disease
Different authors classify this pathology on different grounds:
| Basis for classification | Types of pulmonary hypertension |
| Etiology |
|
| Mechanism of occurrence |
|
| Nature and duration of the course |
|
| Morphological type |
|
As with pulmonary hypertension in adults, persistent fetal circulation in children has 4 degrees of severity. In most cases, the disease is diagnosed at the first, reversible stage - then it is compensated with the help of treatment.
If medical intervention turns out to be ineffective, then within a year the child may have stage 2 of the disease, and by the age of 3, irreversible destructive changes in the structure of the lungs and heart, characteristic of stages 3 and 4 of the disease, will occur.
Prognosis for patients
The appearance of pulmonary hypertension in primary or secondary form is considered as one of the extremely unfavorable signs. It significantly aggravates the condition of children with congenital developmental pathologies, and with rapid progression, it reduces the chances of successful surgical treatment of heart disease.
Without surgery, such patients have a fairly low chance of maintaining health and life. Children who were able to survive have deviations in physical and mental development; they are susceptible to chronic diseases of the pulmonary system, ENT organs, and heart.
Pulmonary hypertension in children occurs with developmental defects or intrauterine infections, hypoxia. The primary form has an unknown origin and a rapidly progressive course. With secondary PH due to heart and respiratory diseases, the initial stages are asymptomatic, and manifestations occur with irreversible changes.
Treatment includes drug therapy, surgical correction, and lung transplantation. The pathology is characterized by an unfavorable prognosis.
Symptoms
A newborn with pulmonary hypertension immediately after birth or several hours later:
- breathes heavily, with shortness of breath;
- when inhaling, the chest is drawn inward;
- has pronounced cyanosis (blue discoloration) of the skin and mucous membranes;
- responds poorly to oxygen therapy: the condition does not improve as expected.
Read about other symptoms of this disease (not only in children) and its treatment here.
Diagnostics
A child is diagnosed based on:
- Anamnestic data - history of pregnancy and childbirth.
- Data from examination and auscultation of the heart.
- Laboratory test results. Indicators of blood oxygenation (oxygen saturation), which are always extremely low in this disease, are of diagnostic importance.
- Results of instrumental studies. The electrocardiogram in this case is not very informative. X-ray and ultrasound with Doppler have greater diagnostic value.
- The child’s body reacts to the supply of oxygen - with pulmonary hypertension, oxygenation indicators after oxygen supplementation remain practically unchanged.
As a result of the diagnostic measures carried out, an experienced doctor will be able to make the correct diagnosis and conduct a differential diagnosis of pulmonary hypertension in children and other diseases with similar clinical manifestations - congenital heart disease, pulmonary embolism (about its symptoms and treatment - here), myocarditis, respiratory diseases .
Do you know how varicocele manifests itself in adolescents and children? Find out how to diagnose the disease at home and how to actually cure it. What is Kawasaki disease and for what reasons does it develop in children? Everything about its dangers and precautions is here.
Clinical picture
In the formation of pulmonary hypertension, the main role belongs to the excessively active growth of the inner layer of the capillary walls. Along with this, dysfunction of the vascular structure is observed. It is at the level of the latter that the inflammatory process occurs. Numerous blood clots gradually form in the bed of the capillaries, and the body begins to produce vasoconstrictor substances in excess volumes.
As a result, persistent oxygen starvation is formed. As a response to ongoing processes, small vessels undergo spasms. The resistance of the vascular bed increases sharply, so the pressure in the pulmonary artery also increases. Against the background of these disorders, the load on the main muscle of the body increases, which inevitably leads to heart failure.
Pulmonary hypertension in children is characterized by a certain clinical picture. First, the number of respiratory contractions increases sharply. The skin acquires a characteristic bluish tint. Its intensity may vary on different parts of the body.
Blood pressure in pulmonary hypertension is usually low. When listening to the heart, a systolic murmur is detected. Doctors explain its appearance by insufficiency of the so-called tricuspid valve. Hypoxemia with this disease can progress quite rapidly. Some patients on ventilators still die. In children who managed to cope with the first symptoms of the disease, the condition usually improves a week after confirmation of pulmonary hypertension.
Diagnostic methods
If you notice signs of hypertension in a child, you should immediately consult a doctor. In a maternity hospital, this could be a pediatrician or a regular neonatologist. Every minute of reflection with such a diagnosis can be fatal.
To confirm pulmonary hypertension, it is extremely important for the doctor to take a history of the child and his mother. For this purpose, he can ask a number of clarifying questions regarding the course of pregnancy and the first days of the baby
After this, the specialist begins to examine the little patient.
Additionally, some laboratory tests may be required. The most informative among them is a routine blood test. The correctness of the preliminary diagnosis should be judged by blood oxygenation indicators. In pulmonary hypertension, this parameter is almost always outside the lower limit.
Also, a small patient is required to undergo an ultrasound with Doppler and an x-ray. The electrocardiogram in this case is characterized by low information content.
Separately, it is necessary to mention differential diagnosis. Since pulmonary hypertension is accompanied by a clinical picture similar to other ailments, it is logical to differentiate it from other pathologies. These include congenital defects, myocarditis, thromboembolism, etc.
Treatment methods
Treatment of newborns with this pathology is carried out in the intensive care unit and involves a number of measures to reduce pressure in the vessels of the lungs, relieve their spasm and prevent complications:
- Carrying out artificial hyperventilation of the lungs with oxygen . Recently, it has been practiced to add nitric oxide to the respiratory mixture, which increases the effectiveness of treatment.
- Introduction of drugs that relax the walls of blood vessels and eliminate their spasm (prostaglandins, Tolazoline, sodium nitroprusside and others). In this case, constant monitoring of blood pressure is necessary.
- In severe cases with a high risk of death, the method of extracorporeal membrane oxygenation .
This is an invasive method of saturating a child’s blood with oxygen using a special device - a membrane oxygenator. This unit is connected to the baby using subclavian catheters, cleans and oxygenates the baby’s blood. Sometimes donor blood is used to replenish the volume of circulating blood in a newborn. - Administration of drugs to prevent the development of heart failure (Dopamine, Dobutamine, Adrenaline) and hypoxia (Eufillin).
- Administration of surfactant to ensure full expansion of the lungs.
- Antibiotic therapy in case of suspected infectious cause of the disease.
- Diuretics and anticoagulants are rarely used in pediatric practice and only for strict indications, in contrast to the treatment of adults with pulmonary hypertension.
Forecasts and preventive measures
With prompt diagnosis and initiation of treatment, the prognosis for life in children with pulmonary hypertension is generally favorable: 9 out of 10 children survive. As a rule, the child’s condition stabilizes by 1 year .
But 30% of children may subsequently suffer from the consequences of respiratory failure and hypoxia in the form of delayed psychophysical development, visual or hearing impairment.
Prevention of pulmonary hypertension in a newborn should be carried out by his mother during pregnancy. To do this, she must eliminate all possible risk factors from her life:
- no smoking;
- minimize the likelihood of intrauterine infection of the fetus;
- do not take medications without permission, without a doctor’s prescription;
- strictly follow all recommendations of the gynecologist.
These recommendations will allow you to avoid many problems and complications of the child’s health, and take care of the baby’s future even before his birth. If it was not possible to avoid pulmonary hypertension in a child, there is no need to despair. It is necessary to contact a professional doctor as soon as possible who can help the child and compensate for his health condition.