A disease whose main symptomatic manifestation is persistent high blood pressure is arterial hypertension. There are two forms of it - primary, secondary.
Primary hypertension (essential) or hypertensive disease (HD) occurs in more than a quarter of the world's population.
It is characterized by a chronic course, and the main clinical manifestation is a long-term persistent increase in blood pressure. It is not possible to find out a single reason for the increase, so the main therapy for hypertension is lifelong use of antihypertensive drugs. In primary hypertension, morphological changes most often affect the heart and blood vessels, however, they are different at different time periods of the pathology. Hypertension is diagnosed only after excluding all hypertension of secondary origin.
The main difference between secondary (symptomatic) arterial hypertension and hypertension is the following: the specific cause of increased blood pressure is always determined, the elimination of which allows not only to lower blood pressure, but also to prevent possible complications in the future. There are such types of it - endocrine, neurogenic, cardiovascular, medicinal, toxic, nephrogenic (renal).
Nephrogenic arterial hypertension is one of the types of symptomatic hypertension, the cause of which is serious dysfunction of the kidneys or pathologies (congenital, acquired) of their vessels.
The share of nephrogenic, among all other types of secondary, accounts for about 30-35 percent. This pathology is a complication after suffering serious kidney diseases, which have a negative impact on the condition of the parenchyma and vascular system of this organ.
Classification
The classification of renal hypertension is based on two main directions. There are three groups based on the causes of origin and two main forms based on the nature of the disease.
Groups
Depending on the complication of what pathology renal hypertension is, the following groups of the disease are distinguished:
- parenchymal;
- Vasorenal;
- mixed.
The parenchymal form develops after serious damage to the renal parenchyma - especially the renal glomeruli within the renal vascular system. These lesions are most often caused by pathologies of a diffuse nature - primary glomerulonephritis, vasculitis, nephritis caused by systemic diseases, nephropathy due to diabetic lesions..
With the development of parenchymal arterial hypertension, an important role is played by chronic pyelonephritis. With unilateral damage, hypertension is recorded in 35 percent of patients, with a bilateral form of pathology - in 43 percent of patients. In addition, the development of this group of nephrogenic hypertension can be provoked by kidney tumors of various origins, tuberculosis, polycystic disease, hydronephrosis, and kidney stones.
Vasorenal renal hypertension develops as a complication after a unilateral/bilateral disruption of the normal functioning of the renal artery or its large branches. The main cause of the pathology is a violation of the flow of arterial blood to the kidney.
Vasorenal hypertension is divided into:
- congenital;
- acquired.
Congenital is a consequence of such genetic changes as:
- the aorta develops incorrectly, anomalies are observed;
- arteriovenous fistula;
- damage to the renal artery by an aneurysm;
- fibromuscular arterial dysplasia;
- hypoplasia of the renal artery.
Acquired renovascular nephrogenic hypertension can develop as a complication after the following serious pathologies:
- embolism/thrombosis of the main artery of the kidney;
- panarteritis;
- atherosclerotic artery stenosis;
- artery/vein stenosis that arose as a complication of nephroptosis.
Mixed renal hypertension - this term speaks for itself. It is fixed if simultaneous damage to the parenchyma and renal artery is diagnosed.
Forms
The clinical course of the disease is practically no different in symptoms from ordinary essential hypertension. Although there are certain features, they are what make it possible to more accurately determine the form of renal pathology.
The disease can occur in two forms:
- benign;
- malignant.
Benign variant – systolic and diastolic pressure is steadily increased, with no tendency to decrease. A sick person quickly gets tired and complains of general weakness. He has severe pain and dizziness, discomfort, pain in the heart, and increased heart rate may occur.
In the malignant form, as a rule, only diastolic pressure is increased (lower number on the tonometer). The pathological process progresses quickly. The main danger is the possibility of developing serious visual impairment, called hypertensive retinopathy
. In the malignant course of the disease, a person often feels nauseous, vomits, has a severe headache in the back of the head, and experiences severe dizziness.
1. Renal parenchymal hypertension syndrome
Urinary system
Renal arterial hypertension
Many kidney diseases, primarily acute and chronic
glomerulonephritis, pyelonephritis, nephrosclerosis, lesions of various etiologies
blood vessels of the kidneys, accompanied by an increase in blood pressure -
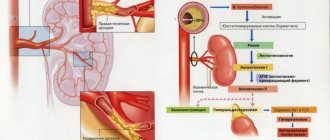
hypertension. This is due to the participation of the kidneys in the regulation of blood pressure. IN
juxtaglomerular apparatus of the kidneys, which is a collection of special
cells at the vascular pole of the glomerulus in the place where the afferent artery approaches the
the initial part of the distal convoluted tubule, in case of renal ischemia
parenchyma intensively produces renin. Renin, acting on the produced
by the liver, hypertensinogen, which belongs to the plasma CC2-globulin fraction, converts
it into angiotensinogen, which, under the influence of the so-called converting enzyme
turns into angiotensin (hypertension). Angiotensin causes increased production
aldosterone, constriction of arterioles and increased blood pressure. Lastly
Since then, works have appeared in the literature linking the occurrence of renal
hypertension also with impaired secretion of special substances by the affected kidneys,
having a hypotensive effect.
According to various authors, renal hypertension accounts for about 10-12% of all
hypertension. It should be noted that hypertension itself, accompanied by
widespread spasm of arterioles and creating the preconditions for atherosclerotic
damage to the arteries, leads to disruption of the blood supply to various organs, including
including the kidneys, and therefore contributes to their increased secretion of renin.
Therefore, at a certain stage of development of hypertension, an increase
blood pressure is already largely determined by renal
mechanism. Renal hypertension as opposed to hypertension of other origins
often (in approximately 1/5 of cases) prone to particularly rapid and malignant
flow.
Hypertension of renal (as well as other) origin is manifested by a number of unpleasant
subjective sensations: headache, dizziness, tinnitus. With a sharp
a rise in blood pressure, the headache is especially painful, often
accompanied by vomiting and paresthesia. As a rule, performance, sleep,
the patient cannot concentrate on doing any work for a long time,
especially mental. When measuring blood pressure, an increase is detected
both systolic and diastolic pressure, the latter often being
relatively high. Usually there is an accent of the second tone on the aorta.
Due to high and persistent hypertension, the load on the heart increases sharply.
Initially, due to constant overload, hypertrophy of the left muscle occurs.
ventricle Myocardial hypertrophy of the left half of the heart can be judged by the increase
apex impulse, some muffling of the first tone at the apex, as well as
characteristic changes revealed by x-ray (rounding of the apex
heart) and electrocardiographic studies (deviation of the electrical axis
heart to the left, a slight increase in the amplitude of the R1 wave in the future - lowering
segment ST1, below the isoline, negative or biphasic wave TI, II). In the chest
ECG leads reveal a high R wave (RV6 > RV5 > RV4).
It should be noted that
initial signs of left ventricular hypertrophy can often be detected later
month from the onset of hypertension.
Subsequently, the growth of the myocardial vasculature usually lags behind the increase in mass
muscle fibers and myocardial oxygen needs, dystrophic
changes in the heart muscle, and then cardiosclerosis. During the same period, due to
characteristic of hypertension and many kidney diseases, especially those occurring with
nephrotic syndrome, a tendency to lipid metabolism disorders may develop
atherosclerosis of the coronary arteries of the heart, which further impairs blood supply
myocardium. Pain in the heart area occurs, often like angina pectoris. For chronic
Kidney diseases may further develop circulatory failure.
In some acute kidney diseases, accompanied by rapid and
significant increase in blood pressure, primarily in acute
glomerulonephritis, the left ventricle does not have enough time
hypertrophy to compensate for the sharply increased load. Therefore maybe
acute deficiency is observed, manifested by an attack of cardiac asthma and
even pulmonary edema.
Renal hypertension is characterized by specific changes in the fundus,
manifested as renal neuroretinitis. However, changes in the fundus during
kidney diseases (in particular, with glomerulonephritis) are caused not only by spasm
arteries and arterioles of the retina and optic nerve, but also to some extent a violation
permeability of the walls of their capillaries, as well as in the final period of chronic renal
diseases ending in nephrosclerosis, uremic intoxication. This
explains the presence of fundus changes caused not only by dystrophic
process, but also increased extravasation through the porous capillary wall, as well as
hemorrhagic syndrome.
In the initial phase, some narrowing of the arteries and arterioles of the retina is observed,
tortuosity of the small veins of the macula, flattening of the veins at the place of their intersection with
arteries with a small ampulla-shaped expansion in front of the intersection (Salus
—Hun I). During this period, patients do not yet complain of visual impairment,
the noted changes are functional in nature and disappear upon normalization
blood pressure (for example, when recovering from acute nephritis or
nephropathy in pregnant women).
Subsequently, due to ongoing spasm and hyalinosis of the walls of their arterioles
the lumen decreases, larger arteries and veins narrow and become tortuous
appear to be compressed by the arteries crossing them, their more pronounced
ampulla-shaped expansion in front of the place of decussation (Salyus-Hun II).
In the final phase, the arteries and arterioles are sharply spasmed and tortuous, reminiscent of
silver wires. Small retinal veins are compacted and sclerosed, in place
intersections with arteries, they form a bend, pressing deep into the retina and creating
illusion of a break (Salus-Hun III). Grayish-white or yellowish lesions are detected
retinal edema and dystrophy, hemorrhage. The optic disc is swollen. In area
yellow spot, radially located foci of dystrophy often resemble a figure
stars. Due to visual dystrophic changes in the fundus and hemorrhages
vision is impaired.
It should be noted that the fundus of the eye is a very convenient place in the body where
you can directly see small vessels and trace their changes, as well as
changes in the surrounding tissue (in this case, the retina) in the dynamics of the disease.
Therefore, examination of the fundus gives a lot of information to the therapist for both diagnosis
renal disease, and to assess its stage and prognosis. In some cases
due to the fact that many kidney diseases can proceed for a long time without
obvious symptoms of their damage, patients can first contact an ophthalmologist
regarding deterioration of vision, and only a characteristic picture of changes in the fundus
allows us to assume renal pathology in these cases, which is confirmed
relevant research.
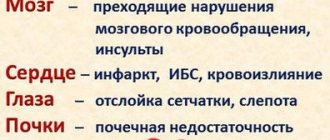
Finally, as a consequence of hypertension and atherosclerosis, disorders may develop
cerebral circulation with paralysis, sensitivity disorders, impairment
functions of the pelvic organs, etc., as well as myocardial infarction.
Causes of development of renal hypertension
The development of hypertension in the parenchymal form is provoked by the following mechanisms:
- the water-electrolyte balance is disturbed;
- hormonal pressor systems are activated;
- depressors are inhibited.
Damage to the parenchyma reduces the total mass of nephrons. Sodium filtration decreases and its reabsorption increases. This causes sodium and water retention in the body - hyperhydration and hypervolemia develop, cardiac output increases - as a result, we have a persistent increase in blood pressure.
In the pathogenesis of the renovascular form, the renin-angiotensin-aldosterone system plays a major role. Insufficient arterial inflow causes increased production of renin. This is a special hormone responsible for the tone of the vessel wall. With an excessive amount of it, the tone of the arteries increases, their lumen narrows - as a result, we observe an increase in pressure.
Symptoms
Signs of the disease in nephrogenic hypertension directly depend on the form of the disease and the nature of the course. One of the main ones, high blood pressure, will always be accompanied by a clinical picture of the pathology that caused the development of renal hypertension.
So, with the parenchymal form, the following manifestations are observed:
- strong thirst;
- general weakness;
- lower back pain;
- frequent urination;
- other dysuric phenomena;
- sometimes elevated temperature.
Vasorenal nephrogenic hypertension manifests itself as follows:
- heaviness, mild pain in the lower back;
- headache, eye pain;
- tinnitus;
- memory impairment;
- insomnia;
- heaviness and pain behind the sternum, rapid heartbeat;
- muscle weakness, convulsive attacks, paresthesia.
In the malignant form (most often found in the renovascular group), vision deterioration rapidly progresses, persistent severe pain in the head is recorded against the background of nausea and vomiting.
Diagnostics
If nephrogenic hypertension is suspected, the doctor first carefully collects an anamnesis, the data of which helps to recognize the secondary nature of the pathology. Nephrogenic arterial hypertension is different:
- sudden onset;
- an increase in blood pressure immediately after acute lower back pain of unknown origin, after a kidney injury, immediately after surgery;
- malignant course of the process;
- rapid progression of hypertension in young people;
- ineffectiveness of conventional antihypertensive treatment;
- lack of heredity to HD.
To make a diagnosis, the following is prescribed:
- general blood test;
- biochemical blood test - allows you to see increased levels of urea, uric acid, creatinine, glucose (in case of diabetes);
- general urinalysis - shows leukocyturia and bacteriuria in case of pyelonephritis, hematuria and proteinuria in case of glomerulonephritis, glucosuria in diabetes, will allow you to see changes in the density of urine;
- Reberg's test;
- studies on the concentration of aldosterone in the blood and the activity of renin.
The following diagnostic procedures are also carried out:
- Ultrasound of the kidneys;
- biopsy;
- dynamic nephroscintigraphy;
- excretory urography;
- angiography (selective renal arteriography, aortography);
- Doppler examination of the renal arteries;
- MRI, spiral CT.
Treatment
Almost all types of nephrogenic arterial hypertension are severe.
Therefore, it is important to carry out effective therapy as soon as possible after identifying the pathology. Without treatment, secondary damage to the heart, brain, and kidneys may develop. The direction of therapy depends on the causes of renal hypertension.
The main treatment method for renovascular hypertension today is balloon angioplasty.
It allows you to expand the stenotic areas of the kidney arteries. In order to avoid repeated stenosis, the renal artery is stented at the same time - a vascular stent (a special elastic metal tube) is installed inside it. The operation is prescribed for atherosclerosis, fibromuscular dysplasia of the renal artery. Contraindications to its implementation are occlusion or damage to the mouth of the artery.
If there are such contraindications, then open surgery is performed to normalize blood flow and preserve kidney function. The operation is performed if there are no pathologies of functionally active epithelial cells, defects in the development of the kidney, or disorders of general circulation.
For the parenchymal type, therapy includes two directions - treatment of the underlying disease and drug hypotensive effects. Specific, sometimes surgical, treatment for the parenchymal form aims to reduce the activity of inflammation, restore the outflow of urine, normalize the immune status and blood clotting functions.
Treatment of nephrogenic hypertension at home
Treatment of nephrogenic hypertension can be done at home if the developed condition does not pose a threat to the patient’s life. If nephrogenic hypertension develops due to life-threatening kidney disease, then treatment in a medical hospital will be a priority.
Treatment of hypertension at home should not imply independent choice and use of medications; it is important to undergo a full examination and follow the doctor’s instructions based on it.
Patients with nephrogenic arterial hypertension should be under clinical observation over the next years, which allows, if necessary, to constantly adjust antihypertensive therapy. Examinations are indicated once every 3 months, and monthly if chronic renal failure develops.
Forecast
In renal hypertension, the prognosis depends on the duration of the pathology, as well as on how timely and effective the therapy was. If the operation was successful (BP decreased noticeably) and was performed before arteriosclerosis developed in the second kidney, the prognosis will be favorable.
If two kidneys are affected at once, the prognosis is definitely unfavorable.
In this case, such dangerous complications develop as progressive renal failure with a chronic course, myocardial infarction, stroke, and dysfunction of the heart muscle. These complications, without immediate adequate treatment, often lead to the death of the patient.
It should be clearly understood that the main component of success in the treatment of nephrogenic arterial hypertension is timely initiation of therapy and strict adherence to all specialist recommendations. Only in this case can we give confident guarantees of a favorable prognosis.
Signs and symptoms
Arterial hypertension of renal origin most often develops gradually, differs from primary hypertension by a higher level of blood pressure during the relaxation phase of the heart. Blood pressure is resistant to antihypertensive therapy. Patients complain of headaches, most often localized in the back of the head, thirst, constant fatigue, loss of appetite, which is typical for hypertension. In the morning, swelling often appears (mainly on the face - of renal origin), which decreases in the evening; with a certain pathology, a laboratory test reveals a certain amount of protein in the urine that exceeds the norm.