Classification of gastrointestinal bleeding is necessary to determine patient management tactics. Along with the rapid development of endoscopic technologies at the end of the last century, the need arose to accumulate and systematize the obtained data and search for their practical application. What was needed was a simple, accessible and obvious classification of bleeding, easy to use. One of the first to meet these requirements was the classification of gastrointestinal bleeding proposed in 1974 by J. Forrest. Having spread quite quickly around the world, it is still the most convenient, having undergone only minor changes in 30 years. It's all about its clinical and prognostic essence: the ability to assess the patient's current condition, treatment tactics and prognosis.
In addition, it allows a surgeon, therapist and endoscopist to have a unified view of the disease. That is why the Forrest classification of gastrointestinal tract is necessary to know not only endoscopists, but also all other doctors of clinical specialties. With the development of endoscopic technologies, other research methods (X-ray, CT, MRI) in diagnosing “gastrointestinal bleeding” have faded into the background. Endoscopy is a reliable method, the gold standard, which allows not only to guarantee the correct diagnosis, but also to perform therapeutic procedures without the use of severe mutilating open surgery. Even with extremely massive bleeding, where endoscopic methods are useless in terms of hemostasis, they make it possible to accurately indicate the location of the lesion, which greatly facilitates surgical intervention. Let us analyze the modern version of the Forrest classification of gastrointestinal bleeding. 1 group. Active bleeding. This includes all types of ongoing bleeding, that is, blood from the defect continues to flow into the lumen of the gastrointestinal tract.
What may indicate the presence of stomach bleeding
Approximately 70% of all hemorrhages of the digestive tract are due to bleeding from ulcerated areas of its upper parts, namely the esophagus, duodenum and stomach.
The characteristics of blood loss are determined by the duration of development of the pathological condition that provoked damage to human blood vessels, as well as the general condition of the patient’s body. Symptoms that indicate a person may have stomach bleeding include:
- pale skin, cold sweat;
- general weakness, dizziness, flashing of black spots before the eyes;
- pain in the heart area;
- constant feeling of thirst;
- uncontrollable vomiting. In this case, by the nature of the vomit, one can tentatively guess in which part of the digestive tract the source of bleeding is localized. Thus, in case of bleeding from the esophagus, the vomit contains an admixture of scarlet blood, and in case of gastric bleeding, where the blood is exposed to gastric juice, the vomit has the appearance of coffee grounds;
- melena stool (black). Blood is detected in a stool test. Since gastric emptying takes at least 12 hours, this is not an early symptom.
- low blood pressure, pulse becomes frequent and weakly filled;
https://www.youtube.com/watch?v=ytadvertiseen-GB
Cold sweat as a sign of gastric hemorrhage
Signs of gastrointestinal bleeding (GIB)
Bleeding from ulcerative formations of the upper digestive organs, which include the esophagus, stomach and duodenum, accounts for more than 70% of all bleeding of the digestive tract. The duration and intensity of the pathological process depends on the disease that led to the violation of the integrity of the vessel, and the general condition of the body.
Symptoms of gastrointestinal tract include:
- weakness, drowsiness;
- dizziness, flashing “black dots” before the eyes;
- decreased blood pressure, increased heart rate, pain in the heart area;
- pale, cold skin;
- thirst;
- vomiting of scarlet blood (with intense bleeding), “coffee grounds” (with moderate bleeding);
- melena stool, black stool (several hours after the onset of blood loss).
With primary bleeding, the fatal outcome is no more than 10% and is more common in elderly patients with severe concomitant pathology. In the event of a relapse (recurrence) of the pathological process, mortality rates increase to 40%, regardless of age and unfavorable prognostic factors.
What causes such bleeding?
Before we look at Forest’s classification of bleeding, let’s talk in more detail about them themselves.
What is the cause of bleeding in the upper gastrointestinal tract? Several points can be highlighted here:
- Internal organ injuries.
- Intoxication of the body.
- Inflammatory processes.
- Damage to the gastrointestinal tract by infection.
- Ulcer or tumor of the stomach, esophagus or duodenum.
- A rarer cause is hereditary pathologies affecting blood vessels and blood. In particular, Rendu-Osler disease, hemophilia.
- Internal organ injuries.
- Intoxication of the body.
- Inflammatory processes.
- Damage to the gastrointestinal tract by infection.
- Ulcer or tumor of the stomach, esophagus or duodenum.
- A rarer cause is hereditary pathologies affecting blood vessels and blood. In particular, Rendu-Osler disease, hemophilia.
Forrest 1A
Jet bleeding
Continuing stream bleeding, regardless of intensity. When large vessels are damaged at the bottom of the ulcer (for example, along the anterior wall of the duodenal bulb), a stream of blood can hit the opposite side of the organ, quickly filling the lumen. In this case, it is unlikely to qualitatively visualize and stop the bleeding. However, by performing injection hemostasis, the endoscopist can reduce bleeding, visualize the vessel, and apply a clip (or perform ligation). However, you should not hesitate for a long time; bleeding of such intensity quickly leads to massive blood loss. In this case, it is better to perform an open emergency operation. For low-intensity jet bleeding, vessel clipping is the method of choice. Stream bleeding occurs in approximately 10% of cases.
Symptoms and treatment of dyspepsia
Main symptoms
It is important for the patient to know not only the Forest classification of bleeding, but also the symptoms of this pathological condition. These will include the following:
- Blood streaks that will be observed in the vomit.
- Uncharacteristic shade of vomit. Most often the color of coffee grounds.
- Loss of strength, chronic feeling of weakness.
- Constant feeling of thirst.
- Low blood pressure.
- Dizziness.
- “Flies are flying before my eyes.”
- Pale skin.
- Tachycardia.
- Black stool.
- Blood streaks that will be observed in the vomit.
- Uncharacteristic shade of vomit. Most often the color of coffee grounds.
- Loss of strength, chronic feeling of weakness.
- Constant feeling of thirst.
- Low blood pressure.
- Dizziness.
- “Flies are flying before my eyes.”
- Pale skin.
- Tachycardia.
- Black stool.
Systematization of gastric bleeding
Modern medicine has decided to classify bleeding according to Forest. Dr. Forest, based on his research, developed it in the late 70s. This classification describes the clinical picture of the source of the unpleasant condition and accurately reflects the important points of the examination. The chosen tactics aimed at treating the disease and the prognosis for the patient depend on this. This classification method has the following points:
- F1 – active bleeding during examination. In this state, discharge can flow in a stream or because. “effusion” (drop by drop).
- F2 – during the study, blood loss was stopped. At the base of the ulceration there may be a thrombosed vessel, the diameter of which reaches no more than 2 mm, or an attached clot of the same size, or thrombosed capillaries.
- F3 – no blood loss is observed, and the bottom of the ulcer is clean.
The presence of bleeding requires that appropriate measures be taken by specialists. So, they must urgently stop it. If these measures are completed successfully, they move on to replenishing lost fluid, as well as normalizing the level of red blood cells, hemoglobin, pressure, and pulse. If hemorrhage is undetected, there is a possibility that the defect is undergoing a healing stage or there are no deviations in vascular integrity.
It is also important to take into account that for accurate results of instrumental research it is necessary to wash suspicious areas of the gastrointestinal mucosa using special solutions. We are talking about clots, erosion, non-uniform surface. All this gives a false picture of the disease.
Timely seeking help will help you recover quickly, without negative consequences for health and life, and also prevent the recurrence of hemorrhage. Be healthy!
How is diagnosis carried out?
If a person is suspected of having gastric bleeding, specialists use an integrated approach to diagnose it.
That means:
- collecting anamnesis, that is, history, disease;
- identifying early signs of gastric bleeding;
- laboratory testing of blood to determine its clinical indicators (primarily, determining the level of hemoglobin and studying the properties of coagulation);
- conducting instrumental examination using, first of all, endoscopic methods (FGDS).
Carrying out fibrogastroduodenoscopy (FGDS) allows you to establish the presence of gastric bleeding, determine the location of the damaged vessel and the degree of intensity of blood loss.
Bleeding, if present, is classified according to different criteria - by etiology, by severity, by the size of the pathology and other signs. A doctor named Forrest and her team created a unified system for describing pathologies of the stomach and duodenum and developed a protocol that is still filled out after FGDS.
The diagnosis itself includes: taking an anamnesis, testing blood in a laboratory setting, and conducting an instrumental examination.
Additional Research
In addition to FGDS, the gastroenterologist will need other data about the patient’s well-being. A clear diagnosis will be established after several step-by-step studies. The doctor needs the readings to complement each other and create an overall picture.
A comprehensive study of the whole organism is necessary.
- Study of the patient's blood composition. A biochemical blood test is needed.
- Composition of urine.
- Medical history (anamnesis), as well as information about the presence of other diseases.
- MRI diagnostics of all internal organs.
If lethargy, pallor, and clouding of consciousness are observed - these are clear signs of blood loss, the patient’s blood pressure and hemodynamics of the heart must be monitored. Those diagnosed with any heart disease undergo fibrogastroscopy under the supervision of an experienced cardiologist.
Important information: How to treat esophageal bleeding and its symptoms
Danger to the patient
Along with Forest's classification of bleeding, many are interested in how dangerous this pathological condition is for humans. If such blood loss occurs for the first time in a patient, then statistics will show a small risk - 10% of cases are fatal. But recurrent bleeding in the upper gastrointestinal tract is already dangerous. There are 50% of deaths from all diagnosed cases. Moreover, the age of the patients does not have a significant impact on this figure.
However, it is noted that the risk of bleeding in the upper gastrointestinal tract is most typical for older people. The reason is that they are more likely to develop serious complications of any pathological processes in the body. And most often it is the upper parts of the digestive system that are affected - this is 70% of all cases.
Along with Forest's classification of bleeding, many are interested in how dangerous this pathological condition is for humans. If such blood loss occurs for the first time in a patient, then statistics will show a small risk - 10% of cases are fatal. But recurrent bleeding in the upper gastrointestinal tract is already dangerous. There are 50% of deaths from all diagnosed cases. Moreover, the age of the patients does not have a significant impact on this figure.
However, it is noted that the risk of bleeding in the upper gastrointestinal tract is most typical for older people. The reason is that they are more likely to develop serious complications of any pathological processes in the body. And most often it is the upper parts of the digestive system that are affected - this is 70% of all cases.
Along with Forest's classification of bleeding, many are interested in how dangerous this pathological condition is for humans. If such blood loss occurs for the first time in a patient, then statistics will show a small risk - 10% of cases are fatal. But recurrent bleeding in the upper gastrointestinal tract is already dangerous. There are 50% of deaths from all diagnosed cases. Moreover, the age of the patients does not have a significant impact on this figure.
However, it is noted that the risk of bleeding in the upper gastrointestinal tract is most typical for older people. The reason is that they are more likely to develop serious complications of any pathological processes in the body. And most often it is the upper parts of the digestive system that are affected - this is 70% of all cases.
Advantages of the method
The advantage of the FGDS method is the ability to carry it out almost anywhere - both in a specialized office and in a department ward. Based on the results of the examination, having classified the bleeding according to Forest, the specialist can decide on the tactics of further treatment measures - either prescribe conservative methods of treatment, that is, using hemostatic drugs, or immediately refer the patient to the surgical department.
The use of endoscopic methods also makes it possible to determine the volume of necessary surgical intervention - suturing a damaged vessel, excision of an ulcerated area of the mucosa, resection of the stomach. Under endoscopic control, it is possible to directly influence the damaged vessel wall - coagulation, clipping, fibrin filling, injecting the damaged area with hemostatics.
https://www.youtube.com/watch?v=ytpressen-GB
The procedure for fibrogastroduodenoscopy
It is believed that Forest's classification is the most informative. This methodology is now used all over the world. Using gastrofibroscopy, the system clearly allows you to visualize what is happening to the ulcer and understand what treatment to prescribe. Doctors anywhere in the world can read the disease and make a decision.
Another advantage of the classification is the ability to immediately assess the degree of risk of rebleeding and the possibility of preventive treatment.
Diagnostics
Forest's classification of gastric bleeding is used by doctors specifically when diagnosing such cases. The doctor begins his work with the following:
- The patient's medical history is collected. The doctor analyzes the symptoms of the pathological process.
- First of all, laboratory methods are prescribed to study the patient’s health status - a general analysis of a blood sample, a study of its coagulability.
- The patient is prescribed FGDS - fibrogastroduodenoscopy. If a person is admitted to the hospital with gastric or intestinal bleeding in critical condition, then this diagnostic method will be the only one for him.
Forest's classification for gastrointestinal bleeding will explain the examination results obtained using the FGDS technique. Its recognized effectiveness is confirmed by several factors:
- Helps document an episode of gastrointestinal bleeding.
- Determines the location of the damaged vessel.
- Sets the intensity of bleeding. And this helps specialists understand how much blood a person has lost.
Another plus is the convenience of the procedure. It is performed both at the patient’s bedside and in a specialized treatment room.
Analyzing the endoscopic classification of bleeding according to Forest, I would like to draw the reader’s attention to another useful function of FGDS. The technique allows you to influence the defect of a “leaky” vascular wall:
- clipping;
- coagulation;
- fibrin filling;
- injecting the damaged area with drugs that stop bleeding.
If bleeding occurs from the upper parts of the digestive tract, an anamnesis (history) of the disease is collected, the symptoms of gastrointestinal tract are ascertained, and laboratory examination methods are prescribed (general blood count, study of coagulation factors). However, in conditions of urgent (urgent) admission to the hospital with signs of blood loss, the only method for effectively diagnosing the disease in a short time is considered to be FGDS, which allows:
- record an episode of gastrointestinal tract infection;
- determine the location of the damaged vessel;
- set the intensity of bleeding.
The procedure for fibrogastroduodenoscopy
The procedure can be performed directly at the patient’s bedside and in a specialized office. The results obtained make it possible to determine further tactics of patient management, prescribe conservative (drug) therapy or surgical intervention, the specifics and scope of surgical treatment (suturing, excision of ulcers, gastric resection).
Signs of stomach bleeding
Diseases that cause bleeding from the upper digestive tract include:
- peptic ulcer of the stomach and duodenum (occurs with increased acidity of gastric juice);
- tumor disintegration;
- erosive gastritis;
- hereditary Rendu-Osler disease (appearance of defective blood vessels);
- leukemia, hemophilia, uremia.
Contraindications for FGDS include the acute period of myocardial infarction, stroke, and agonal state.
- The patient's medical history is collected. The doctor analyzes the symptoms of the pathological process.
- First of all, laboratory methods are prescribed to study the patient’s health status - a general analysis of a blood sample, a study of its coagulability.
- The patient is prescribed FGDS - fibrogastroduodenoscopy. If a person is admitted to the hospital with gastric or intestinal bleeding in critical condition, then this diagnostic method will be the only one for him.
Another plus is the convenience of the procedure. It is performed both at the patient’s bedside and in a specialized treatment room.
Contraindications
The Forrest classification of ulcerative bleeding is thus applied only on the basis of diagnostic data obtained by fibrogastroduodenoscopy. This gradation cannot explain the results of other studies.
Contraindications to EGD therefore make it impossible to use the classification for abnormal gastrointestinal bleeding in an individual patient. These include the following:
- Stroke.
- Acute stage of myocardial infarction.
- State of agony.
Obvious diagnostic indications for fibrogastroduodenoscopy are:
- clarification of the localization and prevalence of pathology;
- differential diagnosis;
- pathology biopsy (the type of ulcer or oncology is specified).
https://www.youtube.com/watch?v=https:accounts.google.comServiceLogin
In addition to diagnostic ones, there are also therapeutic indications. The main therapeutic indications include:
- Removal of small oncology.
- Stopping dangerous bleeding (F1a and F1b).
- If the bleeding was not severe, but there is a risk of complications, the doctor may prescribe a resection operation - removal of part of the stomach.
The classification has been developed only for erosive and ulcerative diseases. For bleeding caused by rupture of the mucous membrane of the gastric junction or cancer infiltration, the Forest classification cannot be used. This is interpreted as a medical error with consequences.
Contraindications are divided into absolute and relative. Absolute, i.e., those in which it is clearly impossible to diagnose, include:
- the presence of bronchial asthma in the patient;
- epilepsy with frequent seizures;
- atlantoaxial subluxation is an injury to the cervical spine.
And also, FGDS is never performed for a tumor of the esophagus or a severe burn.
Relative contraindications are:
- ischemic disease;
- inflammatory diseases of the oral cavity, pharynx, esophagus or respiratory tract;
- aortic aneurysm, etc.
Diagnosis in these cases will be carried out during the period when the patient begins remission. Or diagnosis will have to be carried out in other ways if the patient does not want to undergo a study that is dangerous for him.
Indications for performing FGDS are the presence of the following diseases in the patient's medical history:
- peptic ulcer of the stomach and/or duodenum;
- malignant forms of cancer, in which the disintegration of neoplasms is observed;
- erosive gastritis;
- Randu-Osler syndrome (hereditary pathology in which defective blood vessels are formed);
- oncological and genetic pathologies of the circulatory system.
Indications for use
Doctors say that the presence of such diseases is an indication for contacting FGDS:
- Stomach and duodenal ulcers. These ailments are formed due to the increased level of acidity of gastric juice.
- Malignant tumors in which the tumors disintegrate.
- Gastritis of erosive type.
- Randu-Osler syndrome, which is a hereditary disease characterized by the formation of defective blood vessels.
- Oncological, genetic pathological processes of the circulatory system.
Important! FGDS should not be performed after a recent heart attack, stroke, or in an agonal state.
More than 67 million rubles are planned to be spent on repair work at the Central District Hospital...
News 2019-04-20 11:04:56
News 2019-04-20 11:04:40
The Forrest classification plays an important role in assessing the patient's risk of rebleeding and death. Based on the endoscopic picture, it is possible to determine the volume of endoscopic manipulations to achieve hemostasis or the indications for surgical intervention.
F1A—stream bleeding from an ulcer
F1B—drip bleeding from an ulcer
FIIA—thrombosed vessels at the bottom of the ulcer
FIIB—blood clot closing the ulcer
FIIC—ulcer without signs of bleeding
FIII sources of bleeding were not detected
F1 a- jet bleeding
https://www.youtube.com/watch?v=ytcopyrighten-GB
F1b - parenchymal bleeding
F2a - thrombosed vessel at the bottom of the ulcer
F2b - blood clots at the bottom of the ulcer
F2c - inclusions of hydrochloric acid hematin at the bottom of the ulcer.
F3 - ulcer without signs of bleeding
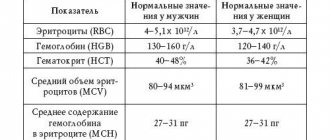
| Forrest classification | Rebleeding rate | Surgery | Deaths |
| Ia Ib | 55-100% | 35% | 11% |
| IIa IIb | 40-50% | 34% | 11% |
| 20-30% | 10% | 7% | |
| III | 5% | 0,5% | 2% |
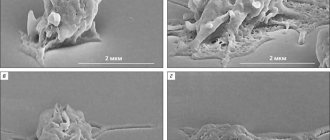
Forrest 2A.
A thrombosed vessel is visible
A thrombosed vessel at the bottom of the ulcer (or several vessels) in the form of a “stump” is clearly visible. No blood comes from the “stump”. You should not think with relief that the bleeding does not continue and the patient is not in danger. Without treatment, recurrent bleeding occurs in most cases. The preferred treatment methods are clipping or ligation, however, they do not completely protect against recurrence. The patient requires intensive monitoring. It is observed in 30-40% of all bleeding cases.
Classification of bleeding according to Forest, its meaning
This classification was developed by Dr. Forest back in 1974. It was intended for the gradation of bleeding, which was established during fiberoscopy of the gastric region and duodenum. The basis for the classification was clinical studies that were directly conducted by Forest himself.
The significance of gradation today is that it has introduced into medical practice that unified system for drawing up a protocol, which is done by a specialist after each FGDS procedure. In particular, this is a technique for visualizing a pathological focus of bleeding. It is important to highlight that it helps to choose the most appropriate treatment tactics for the patient, which directly affects the speed and quality of his recovery.
How does ulcer bleeding stop?
Ulcerative bleeding is fraught with loss of hemoglobin, deterioration of oxygen exchange in tissues, decreased heart rate and other consequences. One of the doctor’s tasks during endoscopy is to stabilize hemostasis so that blood does not leak into the gastrointestinal tract.
Methods of hemostatic effects are different. Mechanical, electrothermal and chemical methods are popular. The most effective hemostasis is injection endoscopic. Using an endoscope, a chemical is injected into the submucosa next to the ulcer, which can quickly stop the pulsation of blood. For this, 1% adrenaline mixed with saline is used.
Ulcerative bleeding is fraught with loss of hemoglobin, deterioration of oxygen exchange in tissues, decreased heart rate and other consequences. One of the doctor’s tasks during endoscopy is to stabilize hemostasis so that blood does not leak into the gastrointestinal tract.
Representation of Forest classification
Let us present to readers the classification of ulcerative bleeding according to J. A. F. Forrest.
The first group is F1 (bleeding in the active stage). Within it, two additional categories will be distinguished:
- F1a - in this case, blood will flow out of the damaged vessel in a stream (sometimes in a pulsating stream).
- F1b - here the blood mass flows out of the vessel drop by drop. Another name is vessel sweating.
The second group is F2. In these cases, the bleeding has already stopped. The group also has its own subcategories:
- F2a - the device detects a thrombosed vessel at the bottom of the ulcer. Diameter - less than 2 mm.
- F2b - a fixed blood clot was found at the bottom of the ulcer. The diameter here will be more than 2 mm.
- F2c - black spots are visible at the bottom of the ulcer. This is what a network of small, already thrombosed vessels looks like.
The last group is F3. There are no subcategories here - this is how the specialist will indicate the result of the examination, in which no gastric or intestinal bleeding was detected (the bottom of the ulcer is clean).
https://www.youtube.com/watch?v=upload
Thus, the classification makes it possible to determine both the stage of pathological bleeding and its activity. The peculiarity of the gradation is that it helps to choose the right therapy for a particular patient:
- If blood loss is observed, the specialist first takes measures for hemostasis (stopping bleeding).
- If vascular bleeding has stopped, then help to the patient is aimed at replenishing the volume of fluid lost by his body, restoring normal blood counts, blood pressure, and pulse.
- If bleeding was not detected, then this fact indicates either the absence of defects in the vascular wall or the healing stage.
The first group is F1 (bleeding in the active stage). Within it, two additional categories will be distinguished:
- F1a - in this case, blood will flow out of the damaged vessel in a stream (sometimes in a pulsating stream).
- F1b - here the blood mass flows out of the vessel drop by drop. Another name is vessel sweating.
The second group is F2. In these cases, the bleeding has already stopped. The group also has its own subcategories:
- F2a - the device detects a thrombosed vessel at the bottom of the ulcer. Diameter - less than 2 mm.
- F2b - a fixed blood clot was found at the bottom of the ulcer. The diameter here will be more than 2 mm.
- F2c - black spots are visible at the bottom of the ulcer. This is what a network of small, already thrombosed vessels looks like.
The last group is F3. There are no subcategories here - this is how the specialist will indicate the result of the examination, in which no gastric or intestinal bleeding was detected (the bottom of the ulcer is clean).
The first group is F1 (bleeding in the active stage). Within it, two additional categories will be distinguished:
- F1a - in this case, blood will flow out of the damaged vessel in a stream (sometimes in a pulsating stream).
- F1b - here the blood mass flows out of the vessel drop by drop. Another name is vessel sweating.
The second group is F2. In these cases, the bleeding has already stopped. The group also has its own subcategories:
- F2a – the device detects a thrombosed vessel at the bottom of the ulcer. Diameter – less than 2 mm.
- F2b – a fixed blood clot was found at the bottom of the ulcer. The diameter here will be more than 2 mm.
- F2c – black spots are visible at the bottom of the ulcer. This is what a network of small, already thrombosed vessels looks like.
The last group is F3. There are no subcategories here - this is how the specialist will indicate the result of the examination, in which no gastric or intestinal bleeding was detected (the bottom of the ulcer is clean).
Classification
Detected bleeding may be active or stopped. If it is not there, the doctor records that it was not detected. In total, there are 3 main groups of bleeding according to Forest.
Forrest 1a
A damaged vessel was found. The bleeding is intense. It is necessary to stop the bleeding, otherwise the pulse will drop and the hemodynamics of the heart will begin to suffer. In such cases, surgery is indicated. The risk of complications is almost 80%. The mortality rate in the postoperative period is also high.
Forrest 1b
Multiple minor bleedings. Capillaries are damaged. In the case of diffuse blood leakage, electrocoagulation is effective as a method of hemostasis. The risk of relapse is about 10%. With the help of electrocoagulation, the threat is prevented and the patient is prescribed bed rest for several days.
Complications with these types - Forrest 1A and 1B - occur in more than half of the cases.
Forrest 2a
A recently bleeding vessel is detected on the endoscope screen. There are risks of re-exacerbation of the ulcer and blood loss. The second group is established when signs of recent bleeding are detected. Doubts often arise about this group. To avoid them, it is customary to make a diagnosis using an endoscope when, during an examination, stigmata are detected in the stomach cavity. Stigmas are bruises.
Forrest 2b
A blood clot has been detected. If a blood clot was detected until 1998, it was considered that there was no danger. The patient was not prescribed anything. But a study conducted in 1998 by D. Lowe showed that a clot often only covers a damaged, eroded vessel. Therefore, anticoagulant drugs are still needed.
Forrest 2c
A black bottom of the ulcer was discovered. A layer of hydrochloric acid hematin is found in the ulcer. Hematin is a product of the oxidation of hemoglobin contained in the blood. This means that there was a slight loss of red blood cells, but there was no threat of death. The prognosis is favorable. Treatment is prescribed conservatively.
Important information: How many days does bleeding last after hysteroscopy surgery?
Forrest 3
An ulcer with a clean bottom is Forrest 3. The diagnosis means that the source of blood loss has not been identified. Upon morphological examination of areas of such ulcers, it became clear that the white bottom can bleed. The eroded vessel due to fibrin is not visible during examination. Fibrin is a protein involved in the process of blood clotting (coagulation). But drip bleeding may be present there.
Further treatment
The diagnostic results allow you to choose the optimal treatment method for a particular patient:
- Conservative. This is drug therapy.
- Operational. This is a surgical intervention of various specifications and scope - from excision and suturing of the ulcer itself to resection of the gastric region.
Today, as progress develops, Forest's classification is used in various modifications and variations. However, the entire system of grading gastrointestinal bleeding is still aimed at determining the activity of the pathological process and selecting the best treatment option for the patient. Classification helps to identify the likelihood of relapse of the pathology, which can be fatal for the patient.
In order to establish a more accurate diagnosis, doctors examine the gastrointestinal tract using fibrogastroscopy. If bleeding is detected, it is necessary to determine how dangerous it is and whether urgent measures need to be taken. Thanks to Forest's classification of bleeding, it is possible to differentiate between extremely dangerous and slightly dangerous conditions. A clear system allows you to describe the specifics of the pathology and developmental changes that have occurred since the previous endoscopic examination.
- Conservative. This is drug therapy.
- Operational. This is a surgical intervention of various specifications and scope - from excision and suturing of the ulcer itself to resection of the gastric region.