In medical practice, there are situations when an individual’s heart beats quite frequently, and the reason for this phenomenon lies not in a stressful situation, but in a permanent type of atrial fibrillation. In the medical history, this pathology is indicated by code I 48, according to the ICD tenth revision. This anomaly is considered life-threatening, since in approximately thirty percent of cases it leads to a failure of cerebral circulation, i.e., a stroke. Moreover, more and more such patients are registered every year. This is due to an increase in life expectancy, including for older individuals with such a diagnosis.
Atrial flutter and atrial fibrillation: what's the difference?
A disruption of the heart rhythm, in which muscle fibers contract chaotically and at a tremendous frequency, reaching up to six hundred beats per minute, is called atrial fibrillation. Externally, this process manifests itself as a rapid pulse, but it is very difficult to palpate. It looks like it's flickering. Thanks to this unusual comparison, the disease received a second name - atrial fibrillation.
A milder variation of arrhythmia is flutter. In this case, the heart rate reaches four hundred beats per minute, but the heart beats at regular intervals.
Quite often, these two rhythm disturbances are identified, but this cannot be done, since the manifestations and genesis of these disturbances are different, which is necessarily reflected in the medical histories. Atrial fibrillation is a random contraction of heart muscle cells at unequal intervals, as well as the presence of several foci that are located in the left atrium and send extraordinary abnormal discharges. Fluttering occurs at regular intervals due to coordinated muscle contraction, since the impulses come from only one focus.
Symptoms of atrial fibrillation
All the main symptoms of atrial fibrillation are associated with increased heart rate. Naturally, such a frequency cannot go unnoticed by a person who suddenly clearly feels a heartbeat and feels weak. A disturbance in the rhythm leads to a lack of oxygen , so the patient most often feels shortness of breath . Chest pain may also be added to the described symptoms .
Symptoms of atrial fibrillation may vary in duration. As a rule, they appear and disappear simultaneously with the attacks. That is, they can take from a couple of seconds to several hours, up to a day (during this time, the degree of manifestation may vary).
In the first few days, the symptoms of atrial fibrillation disappear in a short time, even without the use of any medications. But you need to understand that such attacks never come alone. After the first, short attack, the next one will come. Therefore, when the first signs occur, you should seek treatment from a specialist.
Classification of atrial fibrillation
Let's look at the systematizations used by practicing doctors. According to its form, atrial fibrillation is divided into:
- Newly identified - diagnosed at the moment, and there are no further mentions of its discovery. This type can be asymptomatic and with severe symptoms, paroxysmal or permanent.
- Persistent – fibrillation lasts more than a week. In practice, it is quite difficult to differentiate this and paroxysmal forms.
- Long-term persistent, or also called stable, bothers the patient for a year or more. A pronounced clinical picture is observed only during the period of physical activity.
- The paroxysmal form of atrial fibrillation is indicated in the medical history by its sudden appearance and spontaneous disappearance within two days. If the attacks last up to seven days, then they are also classified as this form of the disease. The patient experiences periodic disruptions in the functioning of the heart, which are accompanied by weakness, pressure changes, shortness of breath, dizziness and chest pain. In rare cases, a pre-fainting state occurs.
- A long-persistent disease is constant atrial fibrillation. The medical history reflects a mutual decision (doctor and patient) that no attempt will be made to restore normal sinus rhythm. With the consent of the individual, i.e. when he changes his mind, measures are taken to control the rhythm. In this case, the arrhythmia again becomes protracted and persistent.
Clinical classification or cause of occurrence. According to this systematization, atrial fibrillation is differentiated by concomitant diseases or conditions that increase the risk of arrhythmia. Let's consider the types of fibrillations:
- Secondary – the provocateurs are heart disease.
- Focal - typical for young patients, especially if there is a history of atrial tachycardia or short-term cases of fibrillation.
- Polygenic – formed against the background of multiple gene mutations at a fairly early age.
- Monogenic – occurs with a single gene mutation.
- Postoperative – open cardiac surgery is a provocateur.
- In professional athletes, it occurs in paroxysms and depends on intense and long training.
- In patients with valve abnormalities, it is formed after operations to correct the valve apparatus, as well as with mitral stenosis.
By severity. EAPC scale, it is used to assess quality of life:
- 1 – there are no symptoms of the disease.
- 2a – minor manifestations, no threat to the individual.
- 2b – palpitations and shortness of breath are felt, but the ability to perform daily activities is not lost.
- 3 – pronounced signs of arrhythmia: weakness, palpitations, shortness of breath.
- 4 – the ability to care for oneself is lost.
Prevention
Individual program of dispensary observation of the patient.
A cardiologist observes:
- at least 2 times a year and when the condition of patients on preventive antiarrhythmic or rhythm-slowing therapy worsens;
- the first 6 months and further - 1-2 times a year for patients after uncomplicated catheter ablation and surgical treatment, for complicated ones - as needed;
- counseling patients if their condition worsens.
Patients with newly diagnosed AF/AFL undergo a comprehensive examination to exclude CVD, obstructive apnea syndrome, hyperthyroidism and other potential risk factors.
A routine outpatient examination once a year includes:
- ECG in 12 leads,
- general and biochemical blood test,
- daily/multi-day ECG monitoring,
- echocardiogram,
- blood tests for thyroid hormones.
All patients receiving VKA are recommended to monitor the INR at least once every 4-6 weeks.
Monitor renal function every 6 months in patients taking NOACs.
Prevalence. Genetic aspects
As an analysis of medical documentation, or more precisely, medical histories shows, coronary artery disease and the tachysystolic form of atrial fibrillation occur in individuals twenty years of age and older, i.e., in approximately three percent of the adult population. The explanation for this fact is as follows:
- early detection;
- the occurrence of concomitant diseases that provoke the appearance of atrial fibrillation;
- increase in life expectancy.
In addition, it was found that the risk of getting sick is higher in men, but representatives of the fair sex are more susceptible to strokes, since they have many concomitant pathologies and a pronounced clinical picture of heart rhythm disturbances.
It has been proven that the disease is based on a gene mutation, i.e., an individual, even if he does not have associated cardiovascular risks, is at great risk of developing atrial fibrillation. Doctors know about fourteen variants of changes in the genotype that lead to rhythm failure.
General information
Atrial fibrillation is one of the possible heart rhythm disorders, with fibrillation being perhaps the most common disorder. As a rule, those changes in the normal functioning of the heart that will be discussed occur as complications of coronary ( coronary heart disease ).
However, although coronary heart disease is the main, it is far from the only cause leading to atrial fibrillation. These may also include increased function of the thyroid gland, which, in turn, also occurs against the background of characteristic diseases.
In medicine, atrial fibrillation is distinguished in two forms: permanent (also called chronic ) and temporary (also called paroxysmal ).
Speaking briefly about the symptoms of atrial fibrillation, we can note their similarity with arrhythmias . The patient also feels periodic interruptions in the heart rhythm; a pre-fainting or fainting state may periodically occur, which is accompanied by darkening of the eyes. In this regard, a synonym for fibrillation is atrial fibrillation .
Although the disease itself is a complication of coronary artery disease, it can also have negative consequences for the body and cause other ailments. The most common consequences are strokes resulting from vascular thrombosis .
The formation of blood clots in the arteries is facilitated by changes in heart rhythm. As a result, clots may appear in the blood - thrombi, which immediately end up in the atrium. There, sticking to the inner wall, they develop.
All this suggests that the disease should under no circumstances be neglected, and the doctor’s recommendations should be strictly followed. It has been proven that if atrial fibrillation is diagnosed in a timely manner and the patient follows the procedure for taking appropriate medications, the risk of thrombosis, as well as other complications, is significantly reduced.
Diagnostics
Before making a diagnosis of atrial fibrillation, the doctor enters an anamnesis into the medical history, where the following information will be important:
- the presence of abnormalities of the thyroid gland, gastrointestinal tract, lungs and others;
- whether there were similar rhythm disturbances in close relatives;
- in women – manifestations of menopause;
- If the patient himself notices rhythm disturbances, then the doctor will be interested in how long they last.
Next is a physical examination. With its help, the doctor also makes a differential diagnosis of flutter. When listening, the heart rate will differ from the pulse rate at the wrist. The conclusion about the regularity of the rhythm is made based on the results of the ECG, which is considered a particularly informative diagnostic method. All information received is also recorded in the medical history. When examining elderly individuals, an electrocardiogram is required. This measure allows us to reduce the number of patients who subsequently develop acute heart failure and ischemic stroke, as well as improve the diagnosis of asymptomatic and paroxysmal forms of fibrillation. To diagnose the latter, it is best to resort to 24-hour Holter monitoring.
Currently, there are innovative methods with which individuals can independently identify violations. However, in terms of information content they are inferior to a cardiogram.
Therapeutic measures
After a diagnosis of atrial fibrillation is made, comprehensive treatment is carried out. This takes into account factors such as:
- symptoms;
- blood pressure numbers;
- heart rate;
- risk of cerebral circulation failure;
- probability of restoration of sinus rhythm;
- the presence of concomitant pathology that aggravates the course of arrhythmia.
After assessing the patient’s condition, the doctor decides on the tactics of its management.
For the prevention of stroke the following are indicated:
- "Warfarin";
- "Dabigatran", "Apixaban".
To control the heart rate, the following strategies are followed:
- heart rate control;
- resumption of natural sinus rhythm.
Of course, the choice of treatment tactics for atrial fibrillation depends on a number of reasons - the length of the pathology, the severity of symptoms, the presence of serious concomitant ailments, age, and others. In elderly patients, the first strategy is most often used. Thanks to this approach, the manifestations of the disease are reduced, and the activity of patients in everyday life improves.
The medications of choice for quickly reducing heart rate are Verapamil, Diltiazem and Bisoprolol. When arrhythmia is combined with heart failure, combinations of beta blockers with digitalis derivatives - Digoxin - are indicated. For individuals with unstable blood pressure, intravenous administration of Amiodarone is recommended.
For regular use use:
- Beta blockers - Carvedilol, Metoprolol, Nebivolol. Regardless of age, they are well tolerated.
- "Digoxin". It is important to choose the right dosage due to toxicity.
- The reserve medicine is Amiodarone.
Thus, in case of a disease - atrial fibrillation - in order to achieve the target level (110 beats per minute) of heart rate, the choice of medications is carried out individually. Initially, a minimum dose is recommended, which is then increased gradually until a therapeutic effect is obtained.
In practice, it has been proven that percutaneous catheter ablation is effective in the treatment of atrial fibrillation, and especially in reducing symptoms. The use of this method together with the latest anticoagulants and new generation antiarrhythmic drugs significantly improves the prognosis. Treatment for atrial fibrillation is:
- taking anticoagulants;
- correction of cardiovascular pathology;
- relief of symptoms.
According to the latest clinical guidelines, the treatment of atrial fibrillation is based on new approaches to antiarrhythmic therapy. To reduce the incidence of atrial fibrillation or limit its manifestations, various non-drug interventions are actively used.
Emergency cardioversion
In another way, it is also called electropulse therapy - this is a manipulation with the help of which it is possible to restore the disturbed rhythm of heart contractions by exposure to electrical discharges. The source of electrical impulses is the sinus node, which ensures uniform contraction of the myocardium; it is located in the wall of the heart. Cardioversion is divided into:
- Pharmacological - sinus rhythm is normalized in approximately fifty percent of patients when using the drugs Amiodarone, Flecainide, Propafenone and others in the treatment of paroxysmal atrial fibrillation. It gives the best result if it is started no later than forty-eight hours from the onset of the attack. In this case, there is no need for preparatory measures, unlike the hardware method. In addition, there is a way to normalize your heart rhythm at home. It was called "pill in the pocket." They use “Propafenone” and “Flecainide” for this.
- Electrical - this method of cardioversion is indicated for individuals with pronounced circulatory disturbances due to the resulting paroxysm of atrial fibrillation.
Let's consider a case from practice. According to the medical history, paroxysmal atrial fibrillation is a preliminary diagnosis that was made to a 25-year-old patient. He made the following complaints:
- inability to breathe deeply;
- heartbeat;
- feeling of lack of air;
- general weakness;
- dizziness.
The young man was seriously engaged in powerlifting and lost consciousness during the next approach. Atrial fibrillation was diagnosed in the patient’s mother and grandmother. Upon objective examination:
- pallor of the dermis;
- shortness of breath at rest;
- low pressure, the upper limit of which is 90 and the lower limit is 60 mm. rt. Art.;
- on auscultation, the heart rate is 400 beats per minute, the first tone is heard louder than normal;
- abnormal rhythm on the radial artery;
- pulse 250 beats per minute.
Additional examinations were ordered to substantiate the diagnosis.
During the period of inpatient treatment, daily ECG monitoring was carried out; paroxysms of atrial fibrillation were not recorded in the medical history, i.e. they were not observed. The patient underwent pharmacological cardioversion with Dofetilide. As a result, sinus rhythm resumed. The young man is advised to limit physical activity.
Classification of the disease
Atrial fibrillation is classified according to several criteria. Based on heart rate, the following forms of the disease are distinguished:
- Tachysystolic form. In this case, the heart rate exceeds 90 beats per minute.
- Bradysystolic form. The myocardial contraction frequency does not reach 60 beats per minute.
- Normosystolic form. In this case, the contraction frequency fluctuates within normal limits, 70 – 80 beats per minute
According to the frequency of occurrence of attacks and their course, the classification is presented as follows:
- Paroxysmal form of atrial fibrillation. The term paroxysm translated from Greek means anger, irritation. This is the most severe form of pathology, associated with severe attacks. Acute paroxysm of atrial fibrillation against the background of myocardial infarction, myocarditis, post-infarction cardiosclerosis often leads to the death of the patient. The paroxysmal form is more often than other varieties detected during the initial detection of the disease; attacks can last from 1 to 5 days.
- Persistent form of atrial fibrillation. It is characterized by a wave-like course, in which attacks of fibrillation are replaced by remission. The attack lasts up to 7 days, but if detected in a timely manner, it can be stopped in 3 to 8 hours.
- The permanent variant or constant form of fibrillation is characterized by a systematic disturbance of the rhythm, without the possibility of restoring normal sinus rhythm.
As a type of atrial fibrillation, atrial flutter is classified as a separate group. This is a variant of very intense heart contractions, more than 400 per minute, provoking a high load on the myocardium.
Atrial fibrillation: treatment
Let's consider treatment options using the example of several real case histories:
- IHD, paroxysmal atrial fibrillation, heart failure - the diagnosis was made on the basis of anamnesis, examination, and research. Patient N., 70 years old, was admitted to the hospital with complaints of severe compressive pain in the retrosternal region, which appears during exercise, palpitations, persistent shortness of breath and a feeling of heaviness in the chest. After taking Nitroglycerin, the pain disappeared within five to ten minutes. The patient was diagnosed with coronary artery disease a year ago. She did not receive any treatment. Upon admission, the dermis is pale, the borders of the heart are shifted to the left. Muffled heart sounds, tachyarrhythmia, systolic murmur, one hundred and twenty beats per minute heart rate. The following therapeutic treatment was prescribed at the healthcare institution: Anaprilin, Cordarone, Celanide, Nitroglycerin and intravenous infusion of glucose.
- The following is an example of a medical history. IHD, paroxysmal atrial fibrillation, ventricular extrasystole, chronic heart failure. Patient T., 60 years old, on the day of arrival at a hospital facility presented with complaints such as interruptions in heart function (lasting for 24 hours), appearing mainly during the day during psycho-emotional arousal and physical activity, shortness of breath, rapid heartbeat, weakness. Stoppages in the functioning of the main organ began to be felt fourteen years ago; rhythm disturbances such as paroxysmal atrial fibrillation and ventricular extrasystole were diagnosed a month before hospitalization. After additional examinations, it was revealed: abnormal and irregular sinus rhythm, sixty-six heart rate, manifestations of left ventricular hypertrophy, heart rhythm failure such as paroxysmal atrial fibrillation. The medical history includes the following treatment: bed rest, statins - Atorvastatin, anticoagulants - Clexane, then Warfarin, Aspirin Cardio, Clopidogrel, Asparkam, Prestarium, Betaloc ZOK, intravenous "Sodium chloride".
- Patient K, 70 years old, was admitted to the hospital with complaints of shortness of breath, fatigue, mild chest pain, and rapid heartbeat during physical activity. I fell ill two years ago (suddenly there was palpitations, weakness, shortness of breath, pain in the area of the heart, radiating to the left limb and shoulder blade), I had my first attack, during which I lost consciousness. He doesn’t remember what treatment he received and what diagnosis was made. On admission, the pulse was irregular and synchronous, eighty-six beats per minute. After receiving the results of additional examinations and examination data, as well as the history of the disease, a clinical diagnosis was made: diffuse cardiosclerosis, coronary artery disease, atrial fibrillation. The medical history indicates the following treatment plan: in case of repeated attacks, create conditions to ensure an influx of fresh air, sit down and calm the patient. Inject sodium chloride, Cordarone, Isoptin, Novocainamide intravenously. Use cardiac glycosides, beta-blockers.
- Patient V., 66 years old. At the time of admission, there were complaints of pressing pain in the area of the heart that occurs during exercise. In this case, the pain radiates to the lower jaw, left shoulder blade and upper limb. After taking nitrates, it stops after three minutes. When walking fast - shortness of breath. In addition, the individual notes interruptions in the functioning of the main organ, which are accompanied by rapid heartbeat, dizziness, and general weakness. I first felt unwell six years ago. He was treated on an outpatient basis and in a hospital, taking nitroglycerin, Metoprolol, Veroshpiron, and acetylsalicylic acid. Preliminary diagnosis, according to the medical history: “Ischemic heart disease, atrial fibrillation, exertional angina.” The patient is scheduled for further examination. A treatment plan has been formed, including the use of nitrates, beta-blockers, and calcium ion antagonists. In the absence of monotherapy with medications from the indicated pharmacological groups, combination treatment is used.
Manifestation of atrial fibrillation
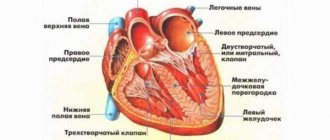
As we have already noted, atrial fibrillation is one of the types of heart rhythm disturbances. In a normal state, this main organ of the human body works like a high-precision mechanism, each part of which is coordinated with each other. In the case of the described disease, atrial contractions can become significantly more frequent, up to six hundred contractions per minute.
If the same frequency were transmitted to the ventricles , the disease would be even more serious than it is. However, despite the lack of coordination between the atria and ventricles, only a frequency of up to 200 impulses/minute can reach them. This is due to the fact that the atrioventricular node cannot produce a larger number of contractions and, in fact, acts as a filter of excessive frequency. Naturally, in this case, the sinus node no longer performs its function of “setting” the rhythm.
We said that atrial fibrillation exists in two forms. If the temporary form is several hours, then the risk of blood clots is relatively small. The same cannot be said about cases where the duration of fibrillation is several days. In this case, the risk of stroke increases significantly. Over time, the paroxysmal form can become permanent, then the possible development of heart failure .
Relief of atrial fibrillation
For each patient with atrial fibrillation, two of the following programs are simultaneously indicated for treatment in the medical history:
- For all individuals - prevention of thromboembolism. This is the primary task of doctors. For these purposes, indirect anticoagulants are used - Warfarin, Dabigatran etexilate, Rivaroxaban. In case of contraindications to their use, clopidogrel, Ticagrelol, and acetylsalicylic acid are used. Due to the fact that the use of antithrombotic therapy is dangerous due to the occurrence of bleeding, their prescription to patients is decided individually, taking into account all the risks.
- In the persistent form - relief of arrhythmia and prevention of relapses, i.e. rhythm control. With this type of atrial fibrillation in the medical history, the drug of choice is Amiodarone. In addition, clinical recommendations also include medications such as Propafenone, Ajmalin, Novocainamide, Dofetilide, and Flecainide.
- With a permanent form, the heart rate is restored. For this, drugs with a quick effect are indicated - Metoprolol or Esmolol, which are administered intravenously, or sublingually Propranolol. If it is impossible to use pharmacotherapy or there is no effect, ablation is used with simultaneous implantation of a pacemaker.
- For paroxysmal atrial fibrillation, the medical history outlines a treatment plan to prevent new episodes of arrhythmia. For this purpose, it is recommended to regularly take antiarrhythmic drugs - Metoprolol, Bisoprolol, Propafenone, Sotalol, Amiodarone. The listed drugs have minimal side effects, including the risk of complications in the form of secondary arrhythmia.
Complications and prognosis
The main complication of atrial fibrillation is the high risk of sudden death of the patient. A lethal outcome is not excluded in any subsequent attack, especially in cases where emergency assistance is not provided in a timely manner. Also, against the background of atrial fibrillation, the following develop: chronic heart failure, thrombosis, strokes, and cardiomyopathies. Any complication is a severe pathology that worsens life and leads to disability.
The prognosis of the disease is favorable with timely diagnosis and compliance with all recommendations of cardiologists, regular use of antiarrhythmic drugs, and lifestyle correction.
The life prognosis is worsened by late detection of the disease, the presence of chronic pathologies, old age and poor lifestyle.
Treatment of coronary artery disease
To substantiate this diagnosis, its clinical form is established. Myocardial infarction or angina pectoris are the most common and most typical manifestations. Other clinical signs are rarely recorded. Having analyzed thousands of medical histories, coronary artery disease and the arrhythmic variant of atrial fibrillation were found in isolated cases. This form manifests itself in the form of pulmonary edema, attacks of cardiac asthma, and shortness of breath. Its diagnosis is difficult. The final diagnosis is formed based on the results of observation and data from selective coronary angiography or electrocardiographic studies in stress tests. Specific therapy depends on the clinical form. General treatment measures include:
- Limiting physical activity.
- Diet food.
- Pharmacotherapy - antiplatelet agents, beta-blockers, fibrates and statins, nitrates, lipid-lowering and antiarrhythmic drugs, anticoagulants, diuretics, ACE inhibitors.
- Endovascular coronary angioplasty.
- Surgical intervention.
- Non-drug treatment methods - stem cells, hirudotherapy, shock wave and quantum therapy.
The prognosis of the pathology is unfavorable, since treatment stops or slows down the process, but does not provide a complete cure. The disease is chronic and progressive.
Different approaches to the treatment of permanent atrial fibrillation. Disease history
In most individuals, atrial fibrillation becomes permanent or persistent, which aggravates the course of the underlying disease.
In this case, the goal of normalizing sinus rhythm is basically not worth it. However, in the uncomplicated stage of the disease, doctors sometimes make attempts to normalize sinus rhythm using pharmacotherapy or cardioversion. In other cases, the goal is to achieve no more than eighty shocks at rest and one hundred and twenty under load. In addition, it is necessary to reduce the risk of thromboembolism. It is prohibited to restore sinus rhythm if, with a permanent form of atrial fibrillation, the medical history contains information about the presence of the individual:
- heart defects requiring surgical intervention;
- thyrotoxicosis;
- left ventricular aneurysm;
- rheumatic diseases in the active stage;
- chronic heart failure of the third degree;
- intracardiac thrombi;
- severe arterial hypertension;
- dilated cardiomyopathy;
- frequent attacks of arrhythmia;
- weakness of the sinus node and bradycardic form of atrial fibrillation and decreased heart rate.
With constant fibrillation, the effect of using medications used to restore rhythm is within forty percent. If the illness lasts no more than two years, then the use of electrical pulse therapy increases the chance of success by ninety percent. When the rhythm failure lasts for a long time and neither the doctor nor the patient makes any attempts to restore it, then the reason for this behavior is that there are doubts about maintaining sinus rhythm for a long time with diagnosed permanent atrial fibrillation.
The medical history, which is considered an important medical document, reflects the patient’s condition, the scheme of diagnostic and therapeutic procedures, and the dynamics of the disease. History is not just a list of information received from the patient and what the doctor discovered during the examination, it is a generalized set of data presented in the form of a detailed and logically coherent report. The quality of this document directly depends on the doctor’s level of knowledge. In addition, when registering it, you should adhere to special rules, compliance with which will help you avoid various mistakes, including legal ones. For example, when the main diagnosis is “IHD, permanent atrial fibrillation,” the medical history indicates in great detail: complaints, medical and life history, objective and additional examination data, treatment plan. In the case of a permanent arrhythmia, surgical treatment is indicated - ablation and installation of a special device (pacemaker). After surgery, the prognosis for an individual’s life is favorable.
Drug treatment of atrial fibrillation
All patients with atrial fibrillation, especially those who have developed for the first time, are hospitalized in a medical facility. After general tests and diagnostics of the body, treatment is prescribed taking into account the indications.
- Most often, treatment of atrial fibrillation in a hospital setting begins with the administration of digoxin (a cardiac glycoside). This drug effectively stops an attack in ⅔ of cases.
- The use of procainamide half an hour after the administration of digoxin significantly enhances the effect of the latter. The only thing is that novocainamide gives a number of side effects (nausea, vomiting, headache, loss of appetite, insomnia, hallucinations).
The drugs can only be administered in a hospital setting, as ECG monitoring is necessary. Their incorrect use can lead to a sharp decrease in blood pressure and heart rate, which can lead to cardiac arrest.
- In some cases, spontaneous cessation of short-term paroxysms is observed. Most often, this happens due to the patient’s excessive excitability, so in such cases it is recommended to take sedatives or take an anaprilin tablet under the tongue.
- An attack of arrhythmia due to alcohol-toxic origin is treated with potassium chloride, which has a high antiarrhythmic effect. Frequent tachycardia is relieved with digoxin; if necessary, therapy is supplemented with obzidan tablets or anaprilin.
- Paroxysm in elderly people who have organic diseases of the heart and blood vessels is first treated with the slow administration of strophanthin. If there is no contraindication (digitalis intoxication), digoxin is used. The absence of results from administration after half an hour is an indication for the use of procainamide. If the remedy also does not produce an effect, then electropulse therapy is used.
Patients with a permanent form of atrial fibrillation are hospitalized only in cases where the refractory period of the atrioventricular node decreases or the heart rate increases. In such cases, reducing therapy is used, including cardiac glycosides, potassium chloride, and isoptin.
Clinical pharmacology case history: atrial fibrillation
The history describes in detail the following anamnesis of the individual: life, hereditary, expert-labor, pharmacological, allergological. As well as objective examination data, results of instrumental and laboratory research methods, rationale for differential and clinical diagnosis, purpose and objectives of treatment. A reasonable choice of pharmacological groups is made to cure a particular patient. For example, the most important directions in treating atrial fibrillation are getting rid of the arrhythmia directly and preventing thromboembolic consequences. There are two ways to treat atrial fibrillation:
- Restoration and maintenance of sinus rhythm - cardioversion (pharmacological and electrical). When performing it, there is always a risk of thromboembolism.
- Control of ventricular rhythm while maintaining atrial fibrillation. Stabilization of sinus rhythm is mandatory in persistent atrial fibrillation. In the case histories of different patients, both electrical and pharmacological cardioversion are found. In addition, maintaining sinus rhythm is also necessary in individuals with paroxysmal atrial fibrillation. The most commonly used medications for this purpose are Disopyramide, Propaphenone, Procainamide, Amiodarone.
When choosing a drug from one group, medications that can worsen the patient’s condition are excluded. The medical history describes both the interaction of the selected medications and the negative phenomena that may appear during pharmacotherapy. The effectiveness of the treatment is described below.
European Society of Cardiology presents 2020 guidelines for atrial fibrillation
The new European Society of Cardiology (ESC) guidelines, which replace the 2020 recommendations, propose an ABC approach to the treatment of patients with AF, where A is anticoagulation for stroke prevention, B is better control of symptoms and C is identification and treatment of comorbidities. At the same time, experts emphasize joint decision-making between the doctor and the patient regarding the choice of therapy. The text of the recommendations is presented in the European Heart Journal.
The authors of the recommendations noted the recently proposed transition from the classification of AF to the characteristics of the disease - the 4S-AF scheme (Stroke risk, Symptom severity, Severity of AF burden, Substrate severity), which proposes to evaluate four main factors: stroke risk, severity of symptoms, severity of disease burden, as well as CVD risks and associated pathologies. The ESC recommends that such assessment be considered in all patients with AF.
Key New Recommendations
Prevention of thromboembolic events
- Periodic assessment of stroke and bleeding risk is recommended to guide treatment decisions and the prevention of potentially modifiable risk factors.
- In patients with AF and an initially low risk of stroke, the first risk reassessment should be performed 4–6 months after the first.
- In the absence of absolute contraindications to oral anticoagulants (OACs), the risk of bleeding should not guide decisions about the use of OACs for stroke prevention.
- The pattern of AF (newly diagnosed, paroxysmal, persistent, long-term persistent, permanent) should not determine the indication for thromboprophylaxis.
Cardioversion
- Pharmacological cardioversion of AF is indicated only for hemodynamically stable patients after assessing the risk of thromboembolism.
- In patients with sick sinus syndrome, atrioventricular conduction disturbances, and QT interval prolongation, pharmacologic cardioversion should not be used unless the risks of proarrhythmia and bradycardia are considered.
Rhythm control and catheter ablation of AF
- To make a decision about ablation, it is recommended to take into account the risks of the procedure and the main risk factors for recurrence of AF.
- Repeat pulmonary vein isolation (PVI) should be considered in patients with recurrent AF if symptoms improve after the first PVI procedure.
- PVI should be considered for rhythm control in patients with paroxysmal or persistent AF after beta-blocker treatment failure or poor tolerability.
- ILV may be considered as first-line therapy for rhythm control in certain patients with paroxysmal episodes of AF or persistent AF without risk factors for relapse as an alternative to class I and III antiarrhythmic drugs.
- Control of risk factors and avoidance of precipitating factors are recommended as part of a rhythm control strategy.
Risk of stroke with cardioversion and catheter ablation
- In patients with AF lasting more than 24 hours, anticoagulation therapy should be continued for at least 4 weeks after successful cardioversion to restore sinus rhythm; If the duration of AF is less than 24 hours and the risk of bleeding is very low, four weeks of anticoagulant therapy may not be used.
- For patients with risk factors for stroke who were not taking OAC before catheter ablation, initiation of anticoagulant therapy is recommended. Preferably, OAC at least 3 weeks before the procedure.
- Ablation without stopping anticoagulant therapy is recommended for patients starting warfarin, dabigatran, rivaroxaban, apixaban and edoxaban.
Long-term therapy with antiarrhythmic drugs
- When treating with sotalol, monitoring of the QT interval, blood potassium levels, creatinine clearance and other factors affecting the risk of arrhythmia is recommended.
- When treating with flecainide, concomitant use of drugs for atrioventricular blockade should be considered.
Lifestyle changes, control of risk factors and concomitant diseases
- Identification and treatment of comorbidities and risk factors are recommended as part of the management of patients with AF.
- Lifestyle changes and treatment of comorbidities are recommended to reduce the burden of AF and the severity of symptoms.
- Opportunistic screening for AF is recommended in patients with hypertension; it should also be considered in patients with obstructive sleep apnea.
Recommendations for percutaneous coronary intervention (PCI)
- For patients with acute coronary syndrome, early discontinuation of aspirin and continuation of dual antiplatelet therapy (DAPT) for up to 12 months after PCI are recommended if the risk of thrombosis is low or the possible risk of bleeding outweighs the risk of thrombosis; for chronic coronary syndrome, the recommended duration of DAPT is 6 months.
Pregnancy
- In pregnant women with hypertrophic cardiomyopathy and persistent AF, cardioversion should be considered.
- If treatment with beta blockers fails, digoxin or verapamil should be considered; If AV block drugs fail, flecainide, propafenone, or sotalol should be considered.
Postoperative AF
- In patients at risk of stroke following non-cardiac surgery, long-term OAC therapy should be considered to prevent thromboembolic events.
- In patients undergoing noncardiac surgery, beta blockers should not be routinely used to prevent postoperative AF.