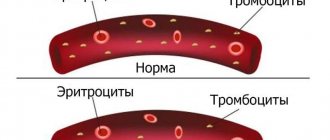
Embolism is the transfer of foreign particles by the bloodstream and their blockage of the lumen of the vessel. The particles themselves are called emboli. Most often, emboli are individual fragments of blood clots that are carried through the bloodstream (thromboembolism). Less commonly, the embolic material is other substances.
“Embolism (from the Greek embollo - throw in, push in) is the blockage of blood or lymphatic vessels by particles and bodies brought with the blood or lymph flow” (BME, vol. 18, Kraevsky, Pytel).
Particles carried by blood or lymph flow are called emboli. Emboli can be endogenous or exogenous. The nature of the embolus determines the type of embolism. An embolus may consist of a blood clot that has broken off somewhere (thromboembolism), fat that has entered the vascular bed (fat embolism), air or gas (air or gas embolism), certain body tissues (tissue embolism), bacteria (bacterial embolism), and also from foreign bodies..." [1]
Depending on the direction of movement of the embolus, there are:
- ordinary (orthograde) embolism (movement of the embolus through the bloodstream);
- retrograde embolism (movement of the embolus against the blood flow under the influence of gravity);
- paradoxical embolism (in the presence of defects in the interatrial or interventricular septum, an embolus from the veins of the systemic circle, bypassing the lungs, enters the arteries).
Forms of the disease
The classification of embolism is based on the type of embolus and its final location after migration has ceased.
Emboli carried by the venous system enter the heart, and from there to the lungs. Emboli carried by arteries can block blood vessels in different parts of the body.
Based on the origin of the embolus, the following types of embolism are distinguished:
- thromboembolism – emboli are blood clots in the arteries, veins and heart;
- air and gas - blockage of blood vessels when air enters the veins or from blood gas bubbles;
- adipose – fat cells act as emboli;
- tissue or cellular embolism – emboli are pieces of tissue or cell complexes;
- liquid embolism - blockage of amniotic fluid;
- bacterial embolism - blockage of blood vessels by accumulations of microbes;
- embolism with foreign bodies.
The most common are thromboembolism, fat embolism, air embolism, and gas embolism.
The severity of thromboembolism symptoms varies from almost complete absence to rapidly developing acute pulmonary heart failure.
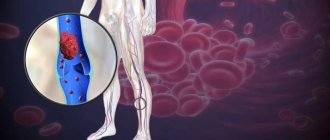
Thromboembolism is the most common type of embolism and occurs when a blood clot breaks off, enters the circulating blood and blocks a blood vessel. If venous thrombi forming on the valve cusps of the left heart, in a cardiac aneurysm, in the left atrial appendage, in the aorta and other arteries become emboli, then the blood flow in the vessel stops, and thromboembolic syndrome develops with ischemic infarction. If the source of thromboembolism is thrombi in the chambers of the right half of the heart or in the veins of the systemic circulation, they enter the branches of the pulmonary artery system. In this case, spasms of the bronchial tree, coronary arteries of the heart, and branches of the pulmonary artery are observed. As a result of blockage of its small branches, hemorrhagic pulmonary infarction develops; damage to large branches can result in death.
With a fat embolism, a blockage of the venous bed occurs with drops of fat from destroyed or melted fat cells of the body. This becomes possible with extensive damage and trauma. Sometimes fat embolism occurs with the intravenous administration of fat solutions or preparations prepared in oil that are not intended for intravenous injection. Once in the arterial bed, fat droplets do not dissolve in the blood, but accumulate in certain places. If the size of such a cluster exceeds the diameter of the vessel (6-8 microns), blood flow is disrupted. Fat embolism affects the small capillaries of the lungs and brain. It can have a subacute, acute (develops in the first hours after injury) and fulminant form (the onset of sudden death within a few minutes).
Possible consequences of fat embolism include pneumonia and acute pulmonary failure.
Air-gas embolism occurs when the lumen of the arterial vessels of the pulmonary circulation is blocked by bubbles of air or other gas, which accumulate in the cavity of the right heart and stretch it. If large veins are damaged, air can get into them, then air bubbles with the blood flow enter the heart and spread throughout all arterial basins. Even a small volume of air entering the peripheral veins can become fatal.
In the origin of gas embolism, the main role is played by sudden changes in atmospheric pressure (caisson disease, which develops during immersion and rapid rise from water), due to which undissolved gas bubbles block small arterial vessels without compromising their integrity.
Description
Fat embolism is an extremely dangerous condition in which particles of adipose tissue enter the body’s circulatory system, causing life-threatening and health-threatening complications.
Fat embolism develops most often with injuries to the extremities, including during surgical interventions, when long tubular bones are fractured. Also, a similar condition can develop with multiple pelvic fractures. The sharp edges of the bone fragment damage the vessels lying next to the bone, and the fatty components of the yellow bone marrow enter the vascular bed from the medullary canal. A similar condition, which is called fat embolism syndrome, can occur in conditions such as sepsis, acute pancreatitis, shock of various origins, prolonged compression syndrome, crush injuries of subcutaneous fat, sickle cell anemia and diabetes mellitus. Entering the circulatory system, fat particles in the form of small bubbles that can connect and increase in size enter the vessels of the lungs. In the lungs, fat emboli clog a vessel, depriving one or more areas of the lung of blood supply. Because of this, it is often difficult to immediately make a correct diagnosis, because the symptoms of fat embolism are similar to pulmonary embolism or pneumonia. There are two stages in the development of fat embolism syndrome.
The first is the mechanical stage. Fat from yellow bone marrow or damaged loose subcutaneous fat enters the vascular bed due to a local increase in pressure. In normal condition, the pressure of the bone marrow canal does not exceed 50 millimeters of mercury. Against the background of the general serious condition of the patient, the pressure inside the bone can increase from 50 to 100 millimeters of mercury. Because of this, fat droplets (globules) exit through the capillaries that feed the bone into the bloodstream. The body responds to the appearance of fat emboli in the blood with the active production of fat-dissolving enzymes, the active release of fat from fat depots and the development of an inflammatory reaction in places where the emboli have entered the bloodstream. It has been proven that fat emboli can be detected in the pulmonary capillaries within a few seconds, after injury or surgical manipulation in the bone marrow canal.
The second stage is called biochemical. Leading pathological processes occur in the lungs, since they are a kind of blood filter. Large fatty particles, 10 micrometers or more in size, are not able to pass through the capillaries. Therefore, they remain in the lungs, clogging blood vessels and thus reducing blood flow in certain areas. Smaller emboli pass through the lungs and enter the systemic circulation. Under the influence of enzymes, fat drops are converted into fatty acids, which have a destructive effect on the inner lining of blood vessels. This causes intravascular inflammation, which causes the accumulation of various substances in the blood that negatively affect the general condition of the patient.
The amount of proteins and phosphate compounds in the blood and their functional state affects the fat droplets circulating in the blood. When the metabolism of phosphates and proteins is disrupted, the surface tension of fat emboli changes, which leads to their fusion into larger particles. Because of this, active formation of microthrombi occurs in the blood, intravascular coagulation develops, severe intoxication syndrome develops, and the membranes of the cells that make up the walls of blood vessels are damaged. However, if the described mechanisms of damage have not started, then the presence of small fat droplets in the bloodstream may not appear in any way.
After passing through the pulmonary circulation (pulmonary vessels), small fat drops are able to merge into larger drops and affect not only the lungs, but also other organs with a wide network of microcapillaries. This may also be due to the ability of fat droplets to change their shape - to stretch and deform to the shape of the vessel. The target organs that will be primarily affected by fat embolism syndrome include the brain, retina, kidneys, and skin.
Fat embolism is divided into the following forms:
- Fulminant, which leads to death within a few minutes after fatty elements enter the bloodstream;
- Spicy. With this form of fat embolism, clinical manifestations develop several hours after injury;
- Subacute, with a period of clinical well-being from 12 to 72 hours.
Fat embolism may develop 14 or more days after injury. Most likely, such cases are associated with violation of the rules of immobilization (immobility) of the injured limb.
Causes and risk factors
Each type of embolism has its own causes.
Causes of vascular thromboembolism:
- myocardial infarction;
- heart rhythm disturbances, atrial fibrillation;
- left ventricular aneurysm;
- surgeries on the pelvic organs, abdominal cavity and limbs, amputation of limbs;
- elevated cholesterol levels;
- blood hypercoagulation;
- endocarditis;
- lung diseases;
- rheumatism;
- diabetes;
- oncological diseases;
- diseases of the venous system of the pelvis and extremities (varicose veins, thrombophlebitis, postthrombophlebitis syndrome);
- hypertension.
Causes of fat embolism:
- massive skeletal injuries, fractures of the upper or lower extremities;
- extensive soft tissue injuries;
- fatty liver;
- bone marrow biopsy;
- intravenous injections of liposoluble drugs containing fatty elements that are not intended for this purpose;
- severe burns;
- pancreatic necrosis in severe form;
- long-term corticosteroid therapy;
- osteomyelitis.
The consequences of gas embolism include decompression sickness and severe disturbances in the blood circulation and brain.
Reasons for the development of air and gas embolism:
- decompression sickness;
- injuries of large veins;
- gas gangrene;
- abnormalities in lung function;
- gross violations of the technique of infusion therapy, non-compliance with the rules of venous catheterization, puncture;
- tissue damage during gynecological operations with violation of their technique;
- tissue damage during difficult childbirth.
The main risk factor is prolonged immobility of patients after surgery in the lower extremities, after injuries. The risk group includes all bedridden patients, people forced to lead a sedentary lifestyle, and patients with heart failure. Risk factors also include taking certain medications (chemotherapy, hormone replacement therapy, use of hormonal contraceptives).
Embolism prevention
To avoid gas and oil embolism, you should follow the rules for carrying out invasive procedures - operations, injections, intubation procedures, etc. You can prevent septicopyemia by sanitizing foci of infections in a timely manner and refraining from independently getting rid of pustular skin processes (especially in the nasolabial area). It is impossible to reduce the risk of developing fluid, fat, and tissue embolisms by following any instructions. The likelihood of thromboembolism also cannot be calculated or prevented; however, a decrease in the percentage of complications during operations on varicose veins has been observed with a preliminary course of using anticoagulants.
Symptoms of embolism
Symptoms of embolism depend on the location of the embolus.
Thromboembolism is manifested by hemodynamic disturbances:
- chest pain;
- shortness of breath and rapid breathing;
- drop in blood pressure
- tachycardia;
- arrhythmia;
- sweating;
- tachypnea;
- coughing up blood.
The severity of thromboembolism symptoms varies from almost complete absence to rapidly developing acute pulmonary heart failure.
Source: stopvarikoze.ru
The main manifestations of fat embolism:
- dysfunctions of the central nervous system (disorders of consciousness and psyche, attacks of severe headaches, motor restlessness, “floating” eyeballs, delirium, delirium, meningeal symptoms, pyramidal insufficiency, paresis, paralysis, coma);
- signs of acute respiratory distress syndrome, acute respiratory failure, hyperthermia, chest pain, shortness of breath, apnea, cough with bloody sputum, tachycardia, tachyarrhythmias;
- petechial rashes on the cheeks, on the skin of the neck, chest, back, and in the armpit area;
- oliguria;
- hemorrhages on the oral mucosa, eye membranes and conjunctiva.
Source: cardiobook.ru
Prevention of fat embolism includes injury prevention, proper immobilization of the limb in the event of injury, and early surgical stabilization of pelvic and long bone fractures.
The main manifestations of air and gas embolism:
- arterial hypotension;
- swelling of the neck veins;
- tachycardia;
- increased central venous pressure;
- chest pain;
- dyspnea;
- bronchospasm of unknown origin;
- motor excitement;
- disturbance of consciousness, fear of death.
Source: orlandohyperbarics.com
Treatment of fat embolism
What it consists of is interesting to everyone. Numerous therapeutic methods proposed to get rid of PVCs are not effective: administration of glucose to reduce the mobilization of free fatty acids, ethanol to reduce lipolysis. Serious injuries are often accompanied by coagulopathy. Usually, during the first three days, Heparin (including low molecular weight) is prescribed, which increases the risk of bleeding and increases the concentration of fatty acids in the plasma, and such treatment is generally not indicated.
There is no evidence that frequently prescribed drugs for the treatment of PVCs, such as sodium hypochlorite, Contrikal, Gepasol, Lipostabil, Essentiale, and nicotinic acid, can have a positive effect on the pathology. Therefore, treatment is predominantly symptomatic.
The purpose of respiratory therapy is to maintain PaO2 levels above 70-80 mm Hg. Art. and 90% ≤ SpO2 ≤ 98%. If the case is mild, then oxygen therapy through nasal catheters is sufficient. The occurrence of ARDS in patients requires special modes and approaches of mechanical ventilation.
If it is reasonable to limit the amount of infusion treatment and use diuretics, then it is possible to reduce the accumulation of fluid in the lungs and reduce ICP. Until the patient's condition stabilizes, saline solutions (Ringer's solution, 0.9% sodium chloride) and albumin solutions are used. Albumin promotes effective restoration of volume inside blood vessels and to some extent reduces ICP, and also, by binding fatty acids, can reduce the progression of ARDS.
If the patient has serious cerebral manifestations of fat embolism, then sedative treatment and artificial pulmonary ventilation are used. There is some correlation between the level of increase in ICP and the depth of coma. The management of such patients is in many ways reminiscent of the management of people with traumatic brain injury of a different origin. It is also necessary to prevent the temperature from rising above 37.5 °C, and therefore non-steroidal analgesics are prescribed, as well as physical methods of cooling, if necessary.
Drugs with a wide range of effects are prescribed, most often third-generation cephalosporins - as initial treatment. If clinically significant coagulopathy develops, fresh frozen plasma is used.
The effectiveness of the use of corticosteroids in the treatment of fat embolism in hip fractures has also not been proven. However, they are often prescribed because they think that they can prevent the progression of the process in the future. It is advisable to prescribe corticosteroids for PVCs in large doses. Bolus - Methylprednisolone from 10 to 30 mg per kg for 20-30 minutes. After this, use a dispenser of 5 mg/kg/hour for two days. In the absence of Methylprednisolone, other corticosteroids (Prednisolone, Dexamethasone) are used in equivalent doses.
Diagnostics
To diagnose embolism, a comprehensive examination is prescribed: it is important not only to establish an accurate diagnosis, but also to find out the nature and cause of the embolism.
Diagnosis of thromboembolism is based primarily on the use of computed tomography (CT), a method that allows one to determine the presence of a blood clot in the pulmonary vessels. Other diagnostic methods are also used (ventilation-perfusion scintigraphy, venous compression ultrasonography, pulmonary vascular angiography), which are of auxiliary value.
Source: cardiobook.ru
In case of fat embolism, laboratory tests can reveal:
- decreased oxygen content in the blood;
- decreased hemoglobin levels;
- decreased platelet count, decreased fibrinogen levels;
- the presence of neutral fat in urine, blood, sputum, liquor;
- the presence of fatty retinal angiopathy;
- presence of fat on skin biopsy in the area of petechiae.
Instrumental studies (MRI, CT) make it possible to establish the origin of the embolism; chest radiography allows us to exclude or confirm pneumothorax and the presence of acute respiratory distress syndrome. Monitoring using pulse oximetry and control of intracranial pressure are also used.
Diagnosis of air embolism is made using the following methods:
- capnogram - a non-invasive method of measuring and recording carbon dioxide levels during the respiratory cycle;
- blood gas examination reveals external respiration disorders - hypoxemia and hypercapnia;
- transesophageal echocardiography allows you to measure the volume of air entering the systemic circulation and detects atrial septal defect;
- precordial and transesophageal Dopplerography - does not provide information on the amount of air incoming, but is a highly sensitive diagnostic method and allows you to monitor the left and right parts of the heart simultaneously;
- transcranial Doppler sonography - used to assess the speed of blood flow in vessels; it can also diagnose air emboli in the vessels of the brain.
Consequences and complications of amniotic fluid embolism can include acute cerebrovascular accidents, acute renal failure, and death of the mother and fetus.
Diagnosis of embolism.
Diagnosing embolism of the main arteries of the extremities is not difficult. The main clinical sign that allows you to determine the location of the embolus is the absence of pulsation in the place below the blockage of the arteries.
Differential diagnosis is made with spasm and acute thrombosis. Embolism has a more acute onset than thrombosis. Anamnesis plays an important role. Embolism is characterized by the presence of heart disease, which is accompanied by atrial fibrillation. This occurs, while a history of intermittent claudication is more often observed with atherosclerotic lesions, against the background of which thrombosis of the main arteries occurs. In the case of atherosclerotic lesions, systolic murmur is often observed on the other side and in other arterial territories.
More difficult is the differential diagnosis in elderly patients, who may simultaneously have embologenic diseases, obliterating atherosclerosis of the main arteries and aorta. X-ray contrast angiography and Doppler ultrasound are used as diagnostic techniques, which make it possible to determine the proximal level of occlusion, and in the case of atherosclerotic lesions, to determine the condition of the arteries located above the lesion.
Treatment
The choice of embolism therapy methods is based on the type of emboli circulating in the blood and the factors that provoked the development of pathology.
The main directions of treatment of thromboembolism:
- hemodynamic and respiratory support (taking cardiac glycosides, glucocorticoid hormones, diuretics, cerebroprotectors; oxygen instillation);
- anticoagulant therapy - thinning the blood, improving its rheological properties;
- thromboembolectomy - surgical removal of emboli from the pulmonary arteries using a Fogarty probe;
- emergency fibrinolysis – dissolution of thromboemboli;
- oxygen therapy for patients with hypoxemia;
- antibiotic therapy for infectious complications, ulcers and bleeding.
Treatment of fat embolism:
- resuscitation measures, artificial ventilation;
- instillation of an oxygen mixture;
- lytic therapy - the use of disemulsifiers of fat emboli in the blood;
- taking glucocorticoid hormones, anticoagulants, cardiac glycosides.
Treatment of air embolism:
- emergency measures, elimination of the source of embolism;
- rapid aspiration of air through the central venous catheter;
- if the condition worsens - resuscitation measures, artificial ventilation;
- oxygen instillation;
- infusion therapy with plasma expanders;
- taking vasopressors to treat arterial hypotension;
- hyperbaric oxygenation (treatment in a pressure chamber);
- stabilization of hemodynamic parameters.
Types of embolism
There are two types of fat embolism depending on the speed of manifestation. Thus, they talk about fulminant embolism, when damage to the musculoskeletal system leads to the rapid entry of fat into the blood. In this case, death occurs within a few minutes. And the second option is subacute embolism. Here the clinical picture develops within 12-72 hours, and may appear 2 weeks after the injury. 3-13% of cases result in death.
Based on the lesion, pulmonary embolism, mixed embolism, and cerebral embolism are distinguished.
Possible complications and consequences of embolism
The consequences of embolism depend on the location of the emboli. The main complication of thromboembolism is pulmonary infarction, paradoxical embolism of the vessels of the large circle, chronic increase in pressure in the vessels of the lungs. Possible consequences of fat embolism include pneumonia and acute pulmonary failure.
Emboli carried by the venous system enter the heart, and from there to the lungs. Emboli carried by arteries can block blood vessels in different parts of the body.
The consequences of gas embolism include decompression sickness and severe disturbances in the blood circulation and brain. Consequences and complications of amniotic fluid embolism can include purulent-inflammatory complications in the postpartum period, acute cerebrovascular accidents, acute renal failure, and death of the mother and fetus.
Development mechanism
The formation of fat embolism is based on several points. They can be isolated, but are quite capable of meeting in a group. Identifying the essence is required to determine treatment tactics and further management of the person.
The first is the mechanical separation of adipose tissue particles when blood vessels are damaged. This problem arises with fractures, especially multiple ones, when lipids enter the bloodstream and begin to move along it with the blood flow.
Usually the process is accompanied by damage to the arteries, veins, and capillary network, which in itself is dangerous and can provoke a rapid death.
For this reason, the prognosis is negative as such. It is quite possible that an air embolism may also occur, especially with open injuries.
The second option is blood thickening. As a result, the concentration of fatty substances in the liquid connective tissue increases sharply.
The result is the formation of large lipid structures that clog arteries and capillaries and do not allow the tissues to be properly supplied with nutrition and oxygen.
The third option for the development mechanism is a biochemical change in the concentration of fatty substances in the bloodstream.
This is a response to deviations in the level of specific hormones. As a rule, against the background of severe emergency conditions, severe injuries, shock. It becomes the result of the body’s activation of defense mechanisms, a desperate struggle to maintain an adequate level of nutrition of cells and tissues.
Thus, in all cases, fatty embolism develops as a result of a biochemical abnormality or mechanical damage to tissue. It all depends on the specific primary diagnosis.
Without a provoking factor, the disorder does not develop; theoretically, this is possible, but in extremely rare cases (about 0.5% of the total number of recorded situations).
Prevention
Prevention of thromboembolism: timely treatment of cardiac arrhythmias, taking anticoagulants if necessary, therapy for venous pathology of the lower extremities, monitoring blood clotting parameters.
Prevention of fat embolism includes injury prevention, timely and correct immobilization of the limb in case of injury, early surgical stabilization of pelvic and tubular bone fractures, stabilization of bone fragments, and adherence to infusion therapy techniques.
Prevention of air embolism: compliance with the rules of lifting from the depths, correct and timely treatment of areas with damaged venous vessels.
Video from YouTube on the topic of the article:
Causes
A disease such as embolism can have multiple causes. Blood clots along the walls of the left cardiac ventricle appear if the heart muscle is affected. This happens when it comes to aneurysms, extensive myocardial infarction and other diseases of the cardiovascular system.
Embolism affects a large circle of blood circulation, when a blood clot moves from the heart to peripheral organs, this can result in thrombosis of both the upper and lower extremities, problems with the intestines and blood vessels of the brain.
If we are talking about heart pathologies that are associated with problems with the relationship between different parts of the chambers, then emboli can end up in the arteries, moving from the bed of the veins. This type of embolism is called paradoxical.
Classification
The form of the condition depends on the causes and location of the inflammatory focus.
According to the nature of development, pathology is divided into several types:
- fulminant - this type is the most dangerous, since the signs of fat embolism increase rapidly, and the death of the patient can occur after 10 - 20 minutes;
- acute - this form of the disease is characterized by an increase in symptoms within 2-3 hours after a fracture or injury, for example, a fracture of the femur;
- subacute – in this form, gradually (within 72 hours) increasing manifestations of fat embolism syndrome (FES) are observed.
Tips for prevention and care
In addition to paying attention to risk factors, the main goal of preventing fat embolism is to prevent bone fractures, especially long bones in the lower body. To do this, remove obstacles and keep the bathroom and laundry dry at all times to avoid accidental slippage. It is also important to engage in physical exercise that helps improve balance and strengthen bones and muscles.
If you have broken bones or need to undergo any orthopedic surgery, it is important to be aware of the symptoms within the first few hours after the event. Your doctor will likely prescribe prophylactic steroid medications to help prevent fat embolism syndrome.
If a broken bone needs to be repaired, it is important to remain still until surgery is performed. Additionally, surgery should be performed as soon as possible within 24 hours to reduce the risk of fat embolism.
Symptoms
Most often, symptoms appear only when an oil drop gets into the respiratory system. In this case, the following manifestations occur:
- sudden, unreasonable attacks of suffocation (if the patient has asthma, then an oil drop in the pulmonary canal will significantly aggravate the course of the disease);
- sudden cough, sometimes to the point of gagging;
- cyanosis of the upper body occurs;
- strong pressure in the chest area. The patient feels as if something heavy is lying on his chest. An itchy feeling in the lungs also appears. This is one of the sure signs of an oil drop entering the pulmonary system.
Sudden cough and asthma attacks are the first signs of embolism
In addition to all the above symptoms, severe pain at the injection site is the first to appear. The area around the injection may become red and swollen. Some experts may attribute this to individual intolerance to the drug or a peculiar reaction of the body. This is mistake! In 90% of cases this is a sure sign of drug embolism. It is necessary to visit specialists in the near future, before the onset of secondary symptoms (heat throughout the body, swelling, etc.).