Thrombocytopenia in children
Thrombocytopenia is a decrease in the number of platelets. The indicator is monitored by clinical blood testing.
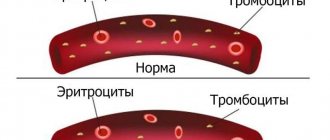
Platelets are a type of blood cell. Like other cells, they are produced in the bone marrow. They have a lamellar shape and in case of injury (cut, scratch or internal tissue rupture) they help stop bleeding. The cells, due to their special properties, stick together to form a single clot and cover the damaged walls of blood vessels. A condition in which there is a persistent decrease in the number of these blood cells is considered thrombocytopenia. It should not be confused with a natural decrease in the indicator. This occurs after injury with bleeding, surgery, menstruation in teenage girls, etc.
Thrombocytopenia of newborns
Thrombocytopenia in newborns is not uncommon.
Which children need treatment? What is the best therapeutic approach? And what can happen if you do nothing? Thrombocytopenia is a disease leading to a decrease in the number of platelets in the blood due to an immune conflict between antigens and platelets.
All forms of thrombocytopenia are considered acquired, even when clinical signs of the disease are detected immediately after birth. Depending on the origin and mechanism of antibody formation, idiopathic and immune forms of the disease are distinguished. Thrombocytopenia is divided into acute and chronic. Thrombocytopenia becomes chronic if it continues for more than six months.
Thrombocytopenia develops in 18% to 35% of patients in the neonatal intensive care unit, and in 73% in cases where the baby had an extremely low birth weight (extremely low body weight).
The incidence of thrombocytopenia in newborns is 1-2 cases per 10,000 births. The mortality rate for this pathology is quite high (13%) due to bleeding.
Forms of thrombocytopenia in newborns
Primary:
- Alloimmune/isoimmune: arise due to incompatibility in one of the blood group systems when foreign platelets are transferred to the child and in the presence of antibodies to them, or when antibodies penetrate to the child from the mother, immunized with an antigen that is absent in the mother, but present in the child.
- Transimmune: occurs in newborns born from a mother with idiopathic thrombocytopenia, systemic lupus erythematosus. The disease occurs through transplacental transfer of antiplatelet antibodies;
- Autoimmune : develop as a result of exposure to platelets by autoantibodies, which are produced by the body in response to its own normal blood platelets.
- Heteroimmune: occur under the influence of a virus or in the presence of an antigen, when the antigenic structure of blood platelets changes, as a result of which the immune system attacks platelets, which serves as a signal for the production of antiplatelet antibodies.
Secondary (symptomatic) can be with:
- infectious diseases
- immunodeficiency states
- Kasabach-Merritt syndrome (large hemangioma)
- hemoblastoses
- aplastic anemia
- prematurity
- postmaturity
- acute asphyxia, etc.
Everything you need to know about thrombocytopenia: causes, symptoms, treatment
Other forms of thrombocytopenia
Immune form: Currently, the immune basis for the formation of thrombocytopenia is most common.
As a rule, the disease begins 2-3 weeks after the newborn has suffered an infectious disease (ARVI, measles, chickenpox, mumps, infectious mononucleosis). In some children, the onset of the disease is preceded by taking certain medications, as well as vaccination (administration of gamma globulin).
Heteroimmune form: The antigenic structure of the platelet can be disrupted by bacteria, viruses, or toxins, as well as certain drugs or vaccines. Another way to develop this form of thrombocytopenia is the formation of antiplatelet antibodies, which are adsorbed on the surface of platelets and, as a result, destroy them.
Isoimmune form: this form can develop as a result of the transfer of platelets from the fetus to the mother (as with Rh incompatibility), or with group incompatibility of platelet antigens of the mother and fetus, as well as due to blood transfusion or platelet mass.
Autoimmune form: this form of thrombocytopenia consists of an initial “breakdown” of the immune mechanism, which begins to produce antibodies against platelets.
Heteroimmune form: this form begins acutely. For hapten forms of the disease after recovery from a viral infection or removal of the drug from the body. When signs of infection disappear, the patient recovers.
Thrombocytopenic purpura clinic
Thrombocytopenia is represented by hemorrhagic syndrome, which may differ in polymorphism. These can be hemorrhages into the skin and mucous membrane in the form of petechiae, ecchymoses, as well as bleeding, regardless of injury.
Causes of pathology
Thrombocytopenia may be primary or secondary. In the first case, the disease is called idiopathic thrombocytopenic purpura. In this pathological condition, the body experiences a decrease in the level of lamellar cells for an unknown reason. Doctors are inclined to develop an autoimmune process.
Secondary thrombocytopenia is a symptom of another disease or pathology. In this situation, a full medical examination is carried out and treatment is directed to the primary disease. The reasons for a drop in platelet count can be divided into several groups:
- Disruption of their production in the bone marrow. Pathology occurs with the development of cancer, metastases in the bone marrow, leukemia in acute or chronic form, anemia, severe viral diseases, intoxication, etc.
- Splenomegaly. A pathological condition in which platelets accumulate in the spleen. At the same time, there is a significant increase in its size.
- Significant destruction of platelets without the production of new lamellar cells by the bone marrow. The pathology is caused by the development of malignant neoplasms, disseminated intravascular coagulation syndrome, thrombosis, and immune disorders due to impaired respiratory function in premature infants.
- Severe bleeding due to injury.
- The reason for the decrease in the indicator in children under one year old and older may be an improper, unbalanced diet or starvation.
Primary stage of the disease
Autoimmune purpura is a pathology in which blood platelets are destroyed under the influence of autoantibodies. A mild form of the disease is characterized by headache, surges in blood pressure, and malaise. At the same time, the content of platelets in the bone marrow is normal or increased. The reason why the disease develops is not fully known. In acute cases, the pathology process does not take longer than six months.
Diseases in children
Autoimmune primary purpura occurs in children under six years of age. The pathological process is observed after a previous viral illness. In some cases, heteroimmune pathology develops after vaccination against viruses. The disease has the same statistics among boys and girls. But during the period of growing up and puberty, girls get sick twice as often.
The pathological process occurs suddenly, unprecedentedly and proceeds violently. Symptoms of the disease in children:
- Rashes on the body of different colors: yellow, red, blue, greenish.
- The spots on the skin take on asymmetrical shapes.
- Rashes appear unexpectedly. Most often this occurs after waking up from a night's sleep.
The course of the disease is accompanied by bleeding from the gums and nose. Girls experience uterine discharge during puberty. Urination is accompanied by blood. Brain damage is extremely rare. A cerebral hemorrhage is indicated by a rash in the mouth, on the mucous membranes, excessive sensitivity of the gums, and redness of the eyeball.
When this pathology occurs in children, the spleen is enlarged to a large size. At the same time, the body temperature remains moderate. The duration of the disease is from six weeks to six months. After a course of therapy, a stable induced remission is achieved in 80% of cases. In some children, autoimmune pathology becomes chronic. The following factors contribute to this forecast:
- Propensity to bleeding, signaling six months before the outbreak of the disease.
- Unprecedented occurrence of the disease.
- The child has infectious foci of a chronic form.
- Lymphocytic pathological reactions in bone tissue.
- Bruising and subcutaneous hematomas that do not go away during therapeutic treatment.
- Acute purpura in girls who have reached puberty.
In children with a chronic pathological form, unexpected remissions are observed. In general, the disease follows the same scenario in adults and children.
Severity
A quantitative indicator of the level of platelets in the blood counts a huge number of these cells. A decrease in their concentration in medicine is divided into four different conditions according to severity.
- Easy. The decrease occurs at 75–99×10 9 /l. In this case, thrombocytopenia does not manifest itself as clinical symptoms or signs of deterioration in the child’s well-being. The problem can be detected after a clinical blood test.
- Moderate. The concentration of blood cells is 50–74×10 9 /l. Manifests itself with mild symptoms. The formation of bruises and hematomas, prolonged bleeding from cuts and scratches that end on their own are possible.
- Moderate weight. The platelet level drops to 20–40×10 9 /l. Symptoms of the pathology become more pronounced, and stopping bleeding requires significant effort. In this case, the child needs treatment.
- Heavy. The platelet count drops below 20×10 9 /l, which poses a serious danger to the child’s life. Urgent medical care is required in a hospital setting.
Thrombocytopenia of newborns
Thrombocytopenia in newborns is not uncommon.
Which children need treatment? What is the best therapeutic approach? And what can happen if you do nothing? Thrombocytopenia is a disease leading to a decrease in the number of platelets in the blood due to an immune conflict between antigens and platelets.
All forms of thrombocytopenia are considered acquired, even when clinical signs of the disease are detected immediately after birth. Depending on the origin and mechanism of antibody formation, idiopathic and immune forms of the disease are distinguished. Thrombocytopenia is divided into acute and chronic. Thrombocytopenia becomes chronic if it continues for more than six months.
Thrombocytopenia develops in 18% to 35% of patients in the neonatal intensive care unit, and in 73% in cases where the baby had an extremely low birth weight (extremely low body weight).
The incidence of thrombocytopenia in newborns is 1-2 cases per 10,000 births. The mortality rate for this pathology is quite high (13%) due to bleeding.
Forms of thrombocytopenia in newborns
Primary:
- Alloimmune/isoimmune: arise due to incompatibility in one of the blood group systems when foreign platelets are transferred to the child and in the presence of antibodies to them, or when antibodies penetrate to the child from the mother, immunized with an antigen that is absent in the mother, but present in the child.
- Transimmune: occurs in newborns born from a mother with idiopathic thrombocytopenia, systemic lupus erythematosus. The disease occurs through transplacental transfer of antiplatelet antibodies;
- Autoimmune : develop as a result of exposure to platelets by autoantibodies, which are produced by the body in response to its own normal blood platelets.
- Heteroimmune: occur under the influence of a virus or in the presence of an antigen, when the antigenic structure of blood platelets changes, as a result of which the immune system attacks platelets, which serves as a signal for the production of antiplatelet antibodies.
Secondary (symptomatic) can be with:
- infectious diseases
- immunodeficiency states
- Kasabach-Merritt syndrome (large hemangioma)
- hemoblastoses
- aplastic anemia
- prematurity
- postmaturity
- acute asphyxia, etc.
Everything you need to know about thrombocytopenia: causes, symptoms, treatment
Other forms of thrombocytopenia
Immune form: Currently, the immune basis for the formation of thrombocytopenia is most common.
As a rule, the disease begins 2-3 weeks after the newborn has suffered an infectious disease (ARVI, measles, chickenpox, mumps, infectious mononucleosis). In some children, the onset of the disease is preceded by taking certain medications, as well as vaccination (administration of gamma globulin).
Heteroimmune form: The antigenic structure of the platelet can be disrupted by bacteria, viruses, or toxins, as well as certain drugs or vaccines. Another way to develop this form of thrombocytopenia is the formation of antiplatelet antibodies, which are adsorbed on the surface of platelets and, as a result, destroy them.
When medical attention is needed
As a rule, parents are not aware of a decrease in platelet levels in children. A slight deviation from the norm does not manifest itself as severe symptoms. However, the child must be taken to the doctor immediately if the following types of ailments occur:
- The baby often hurts himself, bruises appear on his body even from minor injuries or when touched;
- The appearance of nosebleeds;
- The appearance of blood while brushing your teeth;
- Urine has become pink, red or brown;
- Darkening of the stool;
- Bleeding from cuts and abrasions does not stop for more than 10 minutes. The appearance of spider veins and pinpoint hemorrhages on the skin;
- The child often has a headache;
- Heavy and prolonged menstruation in teenage girls.
A pediatrician examines young patients. Based on the clinical picture, the doctor prescribes additional tests. A blood test is required to determine the concentration of platelets, hemoglobin and leukocytes. If a thrombocytopenic state is detected, further treatment can be carried out by a hematologist.
Symptoms and manifestations
Thrombocytopenia is a disease that has a characteristic and pronounced clinical picture. Symptoms of the disease include:
- Frequent and prolonged nosebleeds.
- Heavy and prolonged menstruation in teenage girls.
- Increased bleeding of the gums, which is detected even with a slight impact on them (for example, while brushing teeth or chewing solid food), and after visiting the dentist, the child experiences intense bleeding.
- With minor exposure to the child’s skin, a hematoma appears in this area.
- A characteristic rash (thrombocytopenic purpura) appears on the child’s body and face.
- You can notice the content of bloody elements in urine and feces.
- The child experiences numerous internal bleeding, for example, in the gastrointestinal tract and joints, which leads to disruption of the functioning of the damaged organs.
- The white of the eye is covered with numerous bloody streaks, indicating the presence of hemorrhages in the retina.
Treatment
To normalize the indicator, various medications are used. Treatment of thrombocytopenia in children and adults begins with establishing an accurate diagnosis. In most cases, a decrease in the level of these blood cells is caused by a corresponding disease or pathological process. After recovery, platelet levels return to normal naturally. In the absence of disease, the cause of thrombocytopenia remains unidentified. Treatment is carried out according to the symptoms.
At the first stage of therapy, you should stop taking any blood thinning medications (Aspirin, Ibuprofen, etc.). If necessary, eliminate iron and vitamin B12 deficiency. The diet is adjusted for thrombocytopenia in children. The diet includes more red meat, liver, nuts, buckwheat porridge, pumpkin, etc.
In some cases, it is recommended to change the child’s daily routine. Lack of sufficient time to rest can cause disruption of hematopoietic function.
Drug treatment is prescribed only by the attending physician; bed rest is recommended for the child. In severe cases, the patient should be treated only in a hospital. This need is due to the risk of emergency conditions that can only be treated in a hospital.
For treatment, intravenous immunoglobulins, corticosteroid hormones, rutin, anti-Rhesus serum, and platelet transfusion from a donor are used. If there are appropriate indications, removal of the spleen is prescribed.
Nutrition
Thrombocytopenia is not an indication for dietary nutrition, but the diet is still worth reviewing. You cannot further expose the body to stress, so spicy and too hot foods, fast food, processed foods, smoked foods, products containing dyes and preservatives, and alcohol are excluded from the menu. They irritate the mucous membrane of the digestive tract, therefore increasing the likelihood of gastrointestinal bleeding. Nutrition for thrombocytopenia should be as gentle as possible.
Under no circumstances should you eat food that thins your blood. These are tomatoes, mushrooms, cranberries, viburnum, olive and flaxseed oil, citrus fruits and other foods high in vitamin C.
A diet for thrombocytopenia involves eating only healthy foods, high in vitamins and microelements. If you have iron deficiency anemia, you should include foods that increase hemoglobin in your diet. These are buckwheat, beef liver, nuts, oatmeal, corn and barley. If you are deficient in vitamin B12, you should eat legumes, apricots, peaches, and melons.
Every day it is worth drinking freshly squeezed fruit and vegetable juices (apple, banana, beetroot, cabbage, black radish), it is useful to drink tea from rowan berries, currant branches, raspberry, strawberry, blackberry and strawberry compotes.
To reduce bleeding, you can take a decoction of nettle, with the addition of yarrow, rowan fruits, rose hips, strawberries, chicory and water pepper.
Mild thrombocytopenia in children can be treated only with diet. Medicines are not used. More severe forms require complex treatment.
Prevention
The best way to prevent the development of diseases is a healthy lifestyle and good nutrition for the child. For the normal development of the baby, there should be no deficiency of vitamins and minerals. The diet is balanced, rich in vitamin C and A.
Children should not fast or become vegetarians. The daily menu must include meat and fish dishes. The diet is also supplemented with fresh seasonal vegetables and fruits, nuts, vegetable oils and herbs.
The platelet level is one of the important indicators of health. However, you should not rush to conclusions and panic. A slight decrease in the number of lamellar cells is not a pathology. Only a qualified doctor should make a diagnosis and prescribe treatment.
Thrombocytopenia in children: causes and treatment
Thrombocytopenia
- a condition in which the platelet count is below 150x109/l. The risk of bleeding depends on the platelet count. • Severe thrombocytopenia (platelet count
Diagnosis of immune thrombocytopenia in children
Immune thrombocytopenia
is a diagnosis of exclusion, so careful attention must be paid to the history, clinical features and blood smear to ensure that no more serious diagnosis has been missed. In young children, congenital causes (such as Wiskott-Aldrich or Bernard-Soulier syndromes) should be considered. Any atypical clinical manifestations, such as the presence of hepatosplenomegaly or severe lymphadenopathy, require immediate bone marrow examination to exclude acute leukemia or aplastic anemia.
Research needs to be done
bone marrow if the child is planned to be treated with glucocorticoids, since this therapy can temporarily mask these diseases. It is also necessary to assume SLE. However, if there are characteristic clinical symptoms in the absence of changes in the blood, except for a low platelet count, and there is no intention to treat, then a bone marrow test is not required.
For immune thrombocytopenia
With the exception of prominent skin manifestations and a significantly reduced platelet count, the condition is good and most patients experience rapid remission without any intervention.
Management of children with immune thrombocytopenia
Approximately 80% of children have the disease
It is acute, benign and usually resolves spontaneously within 6-8 weeks. Most children can receive care at home and do not require hospitalization. The approach to treatment is controversial. Most children do not require any therapy, even if the platelet count is less than 10 x 109/L, but treatment should be started if there is evidence of major bleeding (eg, intracranial or gastrointestinal) or ongoing minor bleeding (eg, persistent oral bleeding).
Clinical guidelines
At the legislative level, a procedure has been established for the diagnosis and treatment of children suffering from thrombocytopenia. In particular, it is said that a child who is diagnosed with a severe form of the disease must be hospitalized.
He is prescribed mandatory medication and, in emergency cases, surgery. Children diagnosed with mild or moderate forms of the disease should have regular blood tests to monitor platelet levels.
Thrombocytopenia in children - federal clinical guidelines.
Thrombocytopenia in childhood - causes and manifestations
Childhood thrombocytopenia is a group of diseases that are characterized by a decrease in the number of platelets. They lead to hemorrhagic syndrome (sometimes very severe). Most often it develops due to a sharp drop in platelet levels below a critical value.
Based on statistics, almost 25% of six-month-old babies admitted to the intensive care unit or intensive care unit have platelet levels below normal. The causes of thrombocytopenia in children can be very different. In some cases, this is an increased destruction of platelets, and in others, a decrease in the rate of their formation. Sometimes the reason can be mixed.
Symptoms
The main symptom of thrombocytopenia is a decrease in platelet levels below normal. Normal values for adults are 180–320×109.
Up to 70% of all platelets are in the blood, the rest are in the spleen, where they are destroyed. They live up to 10 days.
There are 3 stages of thrombopenia, depending on the platelet level:
- Stage I – within 50–150×109, this is a satisfactory indicator;
- Stage II – 20–50×109, the main manifestations are subcutaneous hemorrhages in the field of injuries, continuous bleeding after injuries;
- Stage III – below 20×109, the most dangerous condition due to the high risk of spontaneous internal bleeding.
Symptoms of thrombocytopenia in adults
Photo from the site lecheniedetej.ru
Thrombocytopenia in adults is manifested by the following symptoms:
- subcutaneous bruising (purpura, hematoma);
- bruises that do not resolve over a long period of time;
- prolonged bleeding from wounds, cuts and scratches;
- bleeding gums;
- prolonged bleeding after dental procedures or surgical interventions;
- heavy menstruation (in women).
The most dangerous manifestation of thrombocytopenia is internal bleeding. They can be suspected by the red color of urine and feces, weakness, fatigue, pale skin, dizziness, decreased blood pressure and pulse. The patient may lose consciousness or even die from significant blood loss.
Symptoms of thrombocytopenia in children
Thrombocytopenia in children at the initial stage is manifested by small papules or red dots on the skin (usually in the lower extremities), areas of hemorrhage (hematomas) after impacts or compression of the skin.
Thrombocytopenia in newborns can go undetected for a long time because it is asymptomatic.
In childhood, scratches and skin lesions take a long time to bleed and heal. The child often has repeated nosebleeds or gum bleeding. With internal hemorrhages, infants may have blood in their stool and urine. If such a sign appears, the child needs hospitalization.
Platelet functions
The main physiological role of platelets is their participation in blood clotting. In the presence of activating factors, they release certain substances that lead to the formation of a blood clot. In addition to platelets, it contains red blood cells, fibrin threads and other components.
Additional functions of red blood cells are:
- Angiotrophic. It lies in the fact that when platelets are destroyed, growth factors are released in the body. They stimulate the growth of blood vessels and ensure their normal functioning. These same factors are necessary for proper wound healing.
- Protective. Platelets secrete interleukins. They participate in the immune response together with leukocytes. For this reason, some thrombocytopenia in children may be accompanied by immunodeficiencies.
general characteristics
Manifestations of thrombocytopenia in a child - photo:
Thrombocytopenia is a condition in which the platelet count in the blood sharply decreases. Platelets are important elements of blood in the process of blood clotting.
For example, if a child is injured, that is, the integrity of his skin and blood vessels is compromised, platelets accumulate at the site of injury, preventing the development of extensive hemorrhage (this is called blood clotting).
When the level of these cells in the blood decreases, the clotting process is complicated, which means that even a small damage can cause severe bleeding , which is a very dangerous condition, especially when it comes to infants.
The level of platelets in the blood decreases as a result of massive death of these cells, or in case of disturbances in the hematopoietic process, when the body initially produces an insufficient number of platelets.
Platelet norms
The second name for platelets is blood platelets. It emphasizes the external form on the basis of which the laboratory assistant calculates them in a general clinical analysis. The platelet count is measured in thousands per microliter of blood. It is quite dynamic and depends on many factors:
- Age
- Paula
- Associated conditions.
For the female body, the norm is from 180 to 320 thousand units/μl, for the male body – from 200 to 400 thousand units/μl. It is important that in women, a decrease in platelet levels during menstruation or pregnancy is considered a physiological condition.
Recommended examinations
Definitely, if the tests show deviations from the norm, it is worth consulting with a doctor, who at the first stage will prescribe a comprehensive examination. It includes:
- analysis to determine the content of C-reactive protein
- performing ultrasound of internal organs
- Analysis of urine
- blood tests for iron content.
In some cases, a bone marrow puncture may be required. It is a mandatory study if an oncohematological disease is suspected. In this case, the patient remains under the careful supervision of a doctor. Repeated tests to determine platelet levels must be taken every 5-7 days.
The causes and treatment of thrombocytopenia in children are directly related. Only after conducting a comprehensive examination and determining the true cause of the deviation from the norm, the doctor prescribes treatment.
Diagnostics
To make a diagnosis, you need to undergo an examination, which includes the following tests:
- biochemistry;
- general blood analysis;
- coagulogram;
- Duke test (to determine the duration of bleeding).
If hemoblastosis, cancer metastases, Marchiafava-Miceli disease and B12-deficiency anemia are suspected, a sternal puncture and bone marrow trephine biopsy are performed.
Additionally, a chest x-ray, ultrasound of the spleen or liver, endoscopic examination, enzyme-linked immunosorbent assay and platelet antibody test may be required.
Causes of thrombocytopenia
Most often in childhood, a decrease in platelets is associated with purpura, in which antibodies against platelets are formed. But there may be other etiological diseases:
- tuberculosis
- leukemia
- lymphogranulomatosis
- kidney or liver cancer
- erythrocytosis
- arthritis
- various acute infections
- anemia
- hemolysis.
The level of platelets can also decrease in case of poisoning, severe stress, or large blood losses.
Clinical symptoms
Symptoms of childhood thrombocytopenia differ from clinical signs in adults. In children, they are characterized by a microcirculatory-vascular type of bleeding. In other words, the child experiences petechial (point) hemorrhage. On mucous membranes it can be more significant, for example, gingival bleeding. Hemorrhages into internal organs in childhood are rare. The most dangerous of them is intracranial.
However, thrombocytopenic purpura usually manifests itself:
- pinpoint rashes on the skin
- they don't tower over her
- color from purple to brown (depending on the rate of hemoglobin destruction)
- ease of appearance of rashes with a pinch test
- Petechiae can appear on the skin and mucous membranes, incl. and on the conjunctiva.
Treatment
Thrombocytopenic purpura is based on immune mechanisms. Therefore, glucocorticosteroid hormones are first-line drugs. They inhibit the formation of antibodies directed against platelets. Most often, the course of treatment begins with prednisolone, the dose depends on the severity of the disease. Note that immediately after the start of therapy, the platelet level begins to increase.
In severe cases of the disease, splenectomy may sometimes be required - removal of the spleen. However, the improvement of medical science has minimized the number of these disabling operations, especially in childhood. If thrombocytopenia is caused by certain medications, then stop taking them. Most often, after this, the platelet level returns to normal even without specific treatment.
If there is a critical decrease in blood platelets in the child’s body, a platelet transfusion is required. This manipulation is performed in a hospital.
Thrombocytopenia: features and causes
Plate-shaped blood components are formed in the bone fluid from megakaryocytes - giant bone marrow cells, inside of which there is cytoplasm. During maturation, microparticles called platelets detach from megakaryocytes and later enter the bloodstream. The formation and growth of megakaryocytes is controlled by a special hormone of protein origin - thrombopoietin.
It is formed in the liver, kidney tissue and muscles. Then it penetrates into the red bone marrow with the blood flow and provides the blood process for the formation of platelets and megakaryocytes. At the same time, thrombopoietin production is inhibited. This helps to balance these microorganisms and maintain their number at a normal level.
Platelets in the blood
The blood component performs two functions in the human body:
- Stopping bleeding, hemostasis. When the structure of an artery or blood vessel is damaged, platelets are immediately released. Then serotonin is produced - a substance that spasms blood vessels. Platelet processes, connecting with the wall of the damaged vessel, form a barrier that inhibits bleeding. Within a few minutes the hemorrhage stops.
- Supplying blood vessels with nutrients. When destroyed, activated platelets contribute to the growth factor that nourishes the walls of the damaged vessel or artery. The described action helps speed up the recovery process.
Platelets are vital blood cells, without which stopping bleeding and healing wounds is impossible.
Disturbances in physical processes lead to a sharp decrease in the number of platelets in the blood. This causes bleeding and disruption of blood circulation. Depending on the principle of action and distribution system, thrombocytopenia occurs:
- Hereditary.
- Productive.
- Destructive.
- Type of consumption.
- Distribution.
- Type of breeding.
The following article describes each type in detail.
A lack of platelets in the blood can be inherited. In this case, a person detects a blood abnormality from birth. Eg:
- Hereditary pathology of May-Hegglin. Autosomal recessive type of the disease. If one of the parents has the disease, the probability of infecting the child is 50%. There is a disrupted process of division of platelets contained in the red bone fluid, as a result of which the concentration of cells of impressive size decreases. In addition, leukocytosis occurs, impaired functioning of leukocytes in the peripheral blood type.
- Wiskott-Aldrich disease, transient pathology. Characterized by the formation of too small platelets. Due to their irregular structure, their breakdown in the spleen increases, and life expectancy is reduced to two to three hours. The disease is accompanied by inflammatory processes on the skin and decreased immunity. Therefore, additional infection and viruses occur. The disease occurs only among boys of school and preschool age.
- Bernard-Soulier pathology. Occurs in a child only if both parents are ill at the same time. The defect syndrome appears in early childhood. The formation of giant but non-functioning platelets occurs. They are not attached to the damaged artery wall, and are massively destroyed in the spleen.
- Amegakaryocytic thrombocytopenia. An autosomal disease that manifests itself in infancy. A process of deformation occurs in the gene that produces a sensitive reaction to the appearance and formation of megakaryocytes. As a result, the production of platelets by the bone marrow is impaired.
- TAR syndrome. A rare congenital pathology that appears at birth. Accompanied by the absence of radial bones and platelet deficiency. The gene that causes megakaryocytes to grow and develop mutates. As a result, the number of these cells is reduced and leads to an insufficient platelet count in the blood.
Genetic mutations are detected in early childhood and infancy. A doctor specializing in this area can detect pathology and make a diagnosis after a careful examination.
This type of pathology is characterized by a disruption of the process of platelet formation in the bone marrow. A blood defect is observed in diseases of the described nature:
- Aplastic anemia. A process occurring in the red bone marrow that inhibits hematopoiesis, helping to reduce the concentration of all blood cells. The causes of thrombocytopenia are different: taking medications, environmental pollution, increased levels of radiation and HIV infection.
- Myelodysplastic pathology, polycythemia vera. A complex of tumor neoplasms that disrupt the blood flow of red bone tissue. There is a rapid proliferation of blood cells, but the maturation process is disrupted. This leads to an increased concentration of cells that are unable to perform their functions in the body.
Blood cell maturation
- Megaloblastic anemia. Develops when there is insufficient folic acid in the body. There is a disruption in the functioning of DNA cells, which are responsible for storing genetic information data, as well as for the development and formation of blood cells. The circulatory system and mucous membranes of a person are primarily affected.
- Acute form of leukemia. It is a tumor formation of the circulatory system that causes deformation of bone marrow stem cells. Accompanied by excessively rapid division of these cells that are not capable of performing standard functions. Subsequently, tumor cells fill the red bone marrow, eliminating hematopoietic, vital microorganisms from it.
- Myelofibrosis. In the process of this disease, fibrous tissues and mutation of stem cells of the human body are formed. Over time, specific tissue fills the entire space, displacing vital microelements. Pathology also develops in other internal organs, contributing to their enlargement.
- Malignant neoplasms. The final stage of oncology is characterized by the spread of metastases throughout the body and internal processes. This also affects the disruption of the production of hematopoietic cells, leading to a deficiency of platelets and other microorganisms.
- Hypersensitivity to the effects of medications. Some organisms have a feature - excessive sensitivity to medications. The action of some medications has a negative effect on the bone marrow, blocking the formation and formation of platelets.
- Radioactive radiation. When treating oncology, radiation therapy has a negative effect on bone marrow function, slowing platelet formation. The formation of tumors of the hematopoietic system is possible.
- Excessive alcohol consumption. Ethanol contained in alcoholic beverages in excessive quantities leads to deforming processes in bone tissue. The number of necessary components and cells in the blood decreases. The destructive process is observed with the systematic and regular use of alcoholic substances. In the latter case, irreversible processes and complications occur in the body and brain.
The causes listed above affect the development of a productive anomaly when the blood component is disrupted at the formation stage. These cases of pathological processes are studied clinically.
In this type of pathology, the disease is observed in the process of destruction of platelets in the internal organs of a person. For example, possible types:
- Autoimmune thrombocytopenia. The number of platelets in the blood decreases, with minimal consequences for other cells in the body. The exact cause of the pathology is unknown. It is believed that the defect is congenital, genetic in nature. Presumably, the disease can be caused by: hypothermia, viral infections and bacteria, as well as the action of medicinal drugs. Pathology can also develop after vaccination given to prevent a viral disease. When an antigen hits the surface of a platelet, it is destroyed. This leads to sudden hemorrhages.
- Thrombocytopenia in infants. It manifests itself and occurs when platelets in newborns have individual antigens that are not contained in the woman’s body.
- Post-transfusion, post-cytostatic pathology. It appears after a blood transfusion procedure; it can be characterized by the disintegration and destruction of platelets in the blood. The blood mass of a stranger is not immediately perceived by the body. Antibodies are produced to it, and the concentration of platelets decreases for the next ten days after the procedure.
- Decreased platelets due to medications. Selected medications promote the production of antibodies. This leads to the breakdown of platelets in the blood. EDTA-dependent thrombocytopenia, an isolated pathology, develops.
Sometimes medications, viral diseases, blood transfusions, and genetic predisposition lead to the occurrence of pathology. An experienced doctor will be able to identify the disease and establish the correct diagnosis and clinical recommendations.
With this type of pathology, platelets become active while in the vascular bed. This promotes blood clotting. A severe blood defect develops as a result of high cell production, which depletes the capacity of the bone marrow. The following phenomena lead to the disease:
- DIC syndrome, or essential pathology. Occurs when internal organs and their tissues are damaged, followed by blood clotting and depletion of body functions. Platelets are rapidly activated in large numbers from an organ or tissue that has been damaged. This action forms blood clots that block blood flow to vessels, arteries, and internal organs of the body. This phenomenon activates an anticoagulant reaction, which is aimed at restoring the usual course. Against this background, the blood gradually loses its function of coagulation, which leads to heavy external and internal bleeding. During treatment, splenectomy occurs - removal of the spleen and formed tumors. This pathology causes sudden death of a person.
- Thrombotic purpura TTP. This type of disease occurs when there is insufficient content of the coagulating component in the blood. This is explained by the high concentration of prostacyclin, a substance that prevents coagulation, the formation of blood clots, and blockage of veins and arteries. In this case, platelets are destroyed.
- Heparin-induced thrombocytopenia. It appears as a result of the use of heparin, a blood thinning drug that prevents blood clots in the blood arteries. Accompanied by necrosis on the skin, idiopathic urticaria is possible. Tachycardia, chest pain, and fever are observed.