What kind of disease is this?
Kawasaki syndrome is a generalized inflammation of blood vessels with an autoimmune, i.e., arising due to one’s own immunity, nature. It is sometimes also called mucocutaneous lymph node syndrome or periarteritis nodosa.
The essence of the disease is damage to arteries and veins of medium and smaller diameter, which leads to the development of aneurysms, stenoses, and hemorrhages.
The disease was described in a monograph by Tomisaku Kawasaki in 1967, and the name was later given in honor of him.
He identified a group of sick children with the same symptoms:
- skin rash;
- long fever;
- bilateral conjunctivitis;
- enlarged cervical lymph nodes;
- swelling.
At first, the pathology was called “cutaneous mucocutaneous lymphatic syndrome,” but in 1970, lesions of the coronary vessels were also identified.
The peak incidence of Kawasaki syndrome occurs between 12 and 24 months of life, but manifestations have also been recorded before the age of 5 years. In Russia and the CIS countries, the pathology is very rare, most often found in Japan.
In adults, Kawasaki syndrome is recorded in isolated cases, therefore the disease relates to pediatrics and is considered exclusively for children. In adulthood, the course is similar, its severity depends on the primary infection.
It has been established that the main link in pathogenesis is the reaction of antibodies to endothelial cells and viruses. Antibodies attack blood vessels and cause inflammatory processes in the middle layer of the wall, causing the development of smooth muscle necrosis.
This process leads to the formation of aneurysms and ruptures, which can be accompanied by heart attacks and strokes. Most often the cardiac, subcutaneous, renal, axillary, and periovarian arteries are affected.
Kawasaki disease is always accompanied by fever - a temperature of about 40 degrees can remain throughout the course of the disease, so the body experiences severe exhaustion. The arteries of the eye also become severely inflamed, which leads to conjunctivitis. The peculiarity of its course is always a bilateral manifestation.
Constant bleeding due to rupture of aneurysms can provoke the collateral development of disseminated intravascular coagulation syndrome with the formation of a large number of blood clots and subsequent massive hemorrhage. The rheumatological prognosis in this case will be disappointing.
Forecast
With early treatment, rapid recovery from acute symptoms can be expected, and the risk of coronary artery aneurysms is significantly reduced. If left untreated, acute symptoms of Kawasaki disease are self-limiting (i.e., the patient gets better over time), but the risk of coronary artery disease increases significantly. Overall, about 2% of patients die from complications of vasculitis.
Symptoms may recur soon after initial treatment with IVIG. This usually requires readmission and re-treatment. Treatment with IVIG can cause allergic and non-allergic acute reactions, aseptic meningitis (inflammation of the meninges), hypervolemia (increased volume of circulating blood and plasma) and, rarely, other serious reactions.
Overall, life-threatening complications resulting from treatment for Kawasaki syndrome are extremely rare, especially compared to the risks of no treatment.
Possible causes of pathology
The cause of Kawasaki syndrome is not fully established. The high prevalence of the disease in Japan and its rare occurrence outside the Asian region suggests a possible genetic predisposition.
The principle of inheritance of predisposition is also not fully understood. Statistically, approximately 10% of people with a family history of Kawasaki disease are also diagnosed with the disease.
Rheumatology is a branch of medicine that studies connective tissue and highlights the obligatory influence of infection of a viral or bacterial nature.
Pathogens:
- Epstein-Barr virus.
- Parvovirus.
- Rickettsia.
- Herpes.
- Spirochetes.
- Staphylococci.
- Streptococci.
Kawasaki syndrome itself is not contagious to other people, but the bacteria or virus that causes its manifestation can be transmitted. Therefore, when communicating with a child, you should use precautions: gloves, gauze mask.
Symptoms and signs
The disease has a complete and incomplete form. What they have in common is a persistent fever, with the baby’s body temperature at 39-40 degrees, which lasts more than 5 days.
To accurately determine the variety, look at the following mandatory characteristics:
- Bilateral conjunctivitis.
- Changes in the mucous membranes of the nasopharynx, mouth and tongue (“strawberry”, pronounced color, tongue), cracked lips, flushing of the cheeks, redness of the throat.
- Local erythema on the palms and soles, dense swelling, peeling of the skin on the fingers.
- Bright red urticaria, without crusts or blisters.
- Swelling of the lymph nodes in the neck, without discharge of pus.
If all the signs are present, doctors diagnose the full form of the disease; if 2-3 from the list are absent, they diagnose an incomplete form.
Here's what they look like in the photo:
Other symptoms may be present, but they are not necessary to make an accurate diagnosis.
It can be divided into the following types:
- Skin manifestations, lesions of the musculoskeletal system.
- Manifestations on mucous membranes.
- Damage to the heart and blood vessels.
Manifestations on the skin and joints
On the surface of the body, the disease is expressed by a macular rash and blisters.
They appear due to the destruction of blood vessels. They are usually located on the torso or limbs, and can occur in the groin area and armpits - places of greatest skin friction.
Over time, erythema forms on the surface of the skin - severe redness, which is marked by pain. Frequent places of occurrence are the plantar surface of the hands and feet. Strong compaction limits the motor activity of the fingers.
Vascular aneurysms and their destruction affect the joints. Intra-articular bleeding, arthralgia, and arthritis occur in a third of cases. Joint syndrome lasts up to one month, after which stable remission follows with restoration of motor activity.
Manifestations on mucous membranes
The mucous membranes of the eyes and oral cavity are often damaged. In the eyes, this is expressed by conjunctival bleeding, conjunctivitis develops. They are constantly red, streaks of blood are clearly visible.
Language undergoes special changes. Due to bursting vessels, a strawberry or crimson color of the papillary surface of the tongue may appear, which is shown in the photo below:
There is bleeding on the mucous membranes of the cheeks and gums, there are symptoms of inflammation in the pharynx - redness, enlargement of the tonsils, and the possible development of purulent sore throat. Lips crack and bleed.
Cardiovascular symptoms
Kawasaki syndrome is dangerous due to damage to the heart: aneurysms form in the coronary arteries, blood supply deteriorates, and myocardial ischemia occurs.
Myocarditis often manifests itself with tachycardia, pain in the heart, and arrhythmic disorders. In the absence of therapy, acute heart failure may develop with a high probability of death.
Less common: pericarditis, aortic and mitral insufficiency. There may be a defect in the triscupid valve, problems with the lungs due to cardiac dysfunction.
general information
Kawasaki disease (syndrome) is an acute multisystem inflammatory disease of the blood vessels (vasculitis), most often affecting infants and young children. The illness may be characterized by high fever, inflammation of the mucous membranes of the mouth and throat, a reddish skin rash, and swollen lymph nodes (lymphadenopathy).
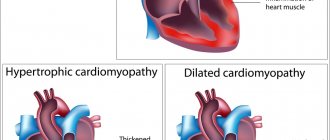
In addition, people with Kawasaki disease may develop inflammation of the arteries that carry blood to the heart muscle (coronary arteritis) associated with a widening or bulging (aneurysm) in the walls of the affected coronary arteries, inflammation of the heart muscle (myocarditis), and/or other symptoms and complications.
Kawasaki syndrome is the leading cause of acquired heart disease in children. Although the cause of the disease is unknown, it is widely believed that it is caused by an infection or an abnormal immune response to an infection.
Stages of the disease
Kawasaki syndrome in children occurs in 3 stages:
- Acute, during the first 10 days.
- Subacute, within 2-3 weeks.
- The recovery period ranges from one month to two years.
The acute stage begins with a sharp rise in temperature (hyperthermia) to 39-40 degrees, with an intermittent character. The high temperature persists throughout the acute period.
Against the background of fever, the cervical and thoracic lymph nodes become enlarged, and there are symptoms of general intoxication syndrome - vomiting, weakness, diarrhea, pain in the liver. During the acute period, conjunctivitis occurs.
The subacute stage is characterized by the appearance of erythema and rashes. Necrosis of the medial layer leads to the formation of aneurysms, and developing bleeding causes thrombosis. This stage is dangerous for the development of damage to the cardiovascular system. The rash on the skin goes away towards the end, the skin begins to peel off, and the manifestation of conjunctivitis subsides.
The recovery stage is characterized by gradual restoration of blood vessels. The duration depends on the massiveness of the lesion and the number of aneurysms. The speed of recovery depends on how quickly treatment was started.
How is diagnosis carried out?
In addition to a routine examination, which is often sufficient to diagnose pathology, tests and instrumental studies are prescribed.
Analyzes
Help in determining pathology helps:
- Blood and urine tests.
- Cerebrospinal fluid examination.
The disease itself does not have any specific markers either in clinical or biochemical blood tests. Kawasaki disease can be diagnosed by summing up factors.
A general blood test will show anemia, thrombocytosis, and an increase in ESR. Biochemistry will show a large number of immunoglobulins and seromucoids. Protein and leukocytes are found in the urine.
The study of cerebrospinal fluid allows us to determine the functional state of the brain and exclude the development of meningitis. This is important because if meningitis is not diagnosed in a timely manner, there is a high risk of irreversible damage to the spinal cord and brain, followed by death.
Additionally, a coagulogram is performed, which serves as a differential examination method to exclude DIC syndrome.
Research
To determine the condition of organs, and especially the heart, the following is carried out:
- ECG.
- EchoCG.
- Chest X-ray;
- Angiography.
The ECG shows tachycardia, initial signs of ischemia, and arrhythmia. It is important at this stage to exclude acute heart failure. EchoCG allows you to find out the condition of the pericardium and heart walls, and the density of the valves.
Diagnosis of cardiac lesions occupies one of the main places in the treatment of this disease, since early therapy helps prevent unpleasant consequences.
Angiography allows you to assess the condition of the coronary vessels, detect aneurysms and thromboses. Additionally, an ultrasound of the kidneys may be prescribed - this is a measure to prevent kidney failure due to damage to the arteries.
Treatment methods
Kawasaki syndrome does not require possible surgical treatment or specific therapy.
Treatment with medications is aimed at eliminating symptoms and, in some cases, suppressing autoimmune processes.
Immunoglobulins
The main method is the introduction of immunoglobulins, which prevent the process of destruction of blood vessels. The main indicator of dose sufficiency is a decrease in temperature in the first few hours after administration. If it is not noted, then repeat the injection until the result is obtained.
Immunoglobulins show the best results in the first 10 days of development, as they help prevent vascular damage.
Aspirin
The second drug is acetylsalicylic acid, or aspirin.
The drug belongs to the group of non-steroidal anti-inflammatory drugs and prevents platelet aggregation. A special advantage is its low toxicity for children.
When the temperature drops, the dose is reduced to the prophylactic level, with the introduction of other anticoagulants.
Aspirin thins the blood, which helps prevent blood clots.
At the same time, treatment for the main infectious complication is being carried out - antibiotics, antiviral drugs. Bacteriophages show good efficiency during the recovery stage, but before that they are able to provoke an immune response and aggravate the situation.
Corticosteroids can be used to suppress autoimmune processes, but their use in the treatment of Kawasaki syndrome is controversial.
Some researchers point to the possible harm of corticosteroids due to their ability to cause the development of aneurysms and negative effects on the blood coagulation system.
Aspirin
A large dosage of the drug is indicated in the first five days to prevent the formation of blood clots.
Aspirin is also an effective anti-inflammatory drug.
The substance thins the blood, reduces the level of inflammation, and lowers temperature.
In the next 2-3 months, the drug is prescribed for preventive purposes.
A runny nose is a typical manifestation of a cold. Green snot in a newborn is not a very good sign, since this color of sputum may indicate a microbial or purulent infection.
You can read about the advisability of using Terzhinan during breastfeeding in this topic.
Possible complications
The main possible consequence of Kawasaki syndrome in young children is myocardial infarction. Multiple aneurysms in the coronary arteries lead to heart damage and ischemia. Preventing these pathologies is the main goal, since acute heart failure almost always leads to death.
Thrombosis can lead to disorders in the brain and kidneys.
Strokes and kidney failure are also quite common complications. To prevent them, anticoagulant therapy is carried out.
Constant bleeding and a weakened immune system can lead to septic shock. It carries complications for the heart and lungs and is a precursor to the development of DIC syndrome. Preventing the latter is also a separate task for doctors.
Prognosis for recovery
In the vast majority of cases, the prognosis is positive. The general course of treatment lasts on average 3 months. The mortality rate from Kawasaki disease is about 1-3%, mainly from vascular thrombosis and subsequent rupture or myocardial infarction.
About 20% of patients who have suffered from the disease acquire irreversible changes in the walls of the coronary vessels, which in the future becomes the cause of atherosclerosis, cardiac ischemia and an increased risk of myocardial infarction.
Smoking and hypertension contribute to this . All patients must be under constant supervision of a cardiologist throughout their lives and undergo a complete examination of the heart and coronary system at least once every 5 years.
Is it possible to correct facial asymmetry in a baby? Find out the answer right now.