Budd-Chiari syndrome – a pathology characterized by impaired venous outflow from liver tissue and the development of stagnant processes. The disease is rarely reported - in 1 in 100,000 people. Women get sick more often than men, and the age group 30-50 years old suffers. Budd-Chiari syndrome is an extremely dangerous condition; liver thrombosis can cause coma or death.
Budd-Chiari disease and syndrome are conditions that occur when blood circulation in the liver is impaired, differing in development and symptoms. A syndrome is only a disorder of blood flow caused by extravascular causes. Budd-Chiari disease is often a secondary vascular lesion against the background of concomitant pathology. Despite the different etiologies, both conditions have similar symptoms, differing only in the speed of their development.
general information
Budd-Chiari syndrome or veno-occlusive liver disease is characterized by obstruction of the hepatic veins and retention of blood in the liver.
After blood enters the liver, it returns to the systemic circulation through the hepatic veins and then into the inferior vena cava, a large vessel that returns blood back to the heart. In veno-occlusive diseases, this blood circulation is partially blocked. The immediate result is liver congestion —the retention of blood flowing into the liver. The liver becomes noticeably painful, increases in volume and causes discomfort.
This condition causes fluid to accumulate in the abdominal cavity - ascites , one of the most common symptoms of Budd-Chiari syndrome.
If the obstruction is severe and affects the vessels that carry blood from the rest of the lower half of the body to the heart, the inferior vena cava, peripheral edema will occur.
Another less noticeable, but no less serious symptom is portal hypertension. It is characterized by increased pressure in the portal veins due to blockage of blood that should flow from the liver. Blocked veins cause other branch veins to dilate— varicose veins . Retained blood can return to the heart through the gastroesophageal veins. They are fragile and cannot cope with high blood pressure and rupture, causing gastrointestinal bleeding from varicose veins.
The condition occurs primarily in people with thrombotic diathesis, including myeloproliferative disorders:
- primary polycythemia (polycythemia vera);
- paroxysmal nocturnal hemoglobinuria (PNH);
- tumors;
- chronic inflammatory diseases;
- coagulation disorders;
- infections.
, drug treatment may be prescribed for symptomatic treatment . If drug therapy alone is used, it will lead to death in 83% of cases. Therapy includes administration of drugs to control ascites, anticoagulant, antithrombotic and angioplasty therapy.
Surgical therapy combined with drug therapy increases patient survival. It consists of surgical decompression or performing a transjugular intrahepatic portosystemic shunt (TIPS). If decompensated cirrhosis occurs, liver transplantation is possible.
The prognosis is negative for patients who are not treated.
As a result of progressive liver failure within 3 months to 3 years from the moment of diagnosis, a person dies. Survival rate 5 years after portosystemic bypass is 38-87%. After liver transplantation, the 5-year survival rate is 70%.
Budd-Chiari syndrome. Treatment
Clinicians need to identify and initiate aggressive and specific therapy aimed at correcting or relieving vascular obstructions. Drug therapy can be initiated for a short period of time and may be of symptomatic benefit. But if doctors use only one drug strategy, it will be associated with a high mortality rate within two years (80-85%).
Anticoagulants
Anticoagulation is necessary in some patients, especially those with hematologic diseases that cause Budd-Chiari syndrome. Prothrombin time and activated partial thromboplastin time should be monitored and maintained within the therapeutic range.
Thrombolytic therapy
This therapy has been used in several cases. Thrombolytic agents include streptokinase, urokinase, recombinant tissue plasminogen activator (RT-PA), and other agents.
Treatment of varicose veins
Gastroscopy may be a useful method in the treatment of varicose veins of the stomach and esophagus. Non-selective beta blockers (eg, propranolol, nadolol) can be used for the primary prevention of variceal bleeding.
Diet
A low sodium diet may be necessary to control ascites.
Paracentesis
Symptomatic treatment of Budd-Chiari syndrome includes diuretics and therapeutic paracentesis.
Liver transplantation
Liver transplantation should be offered to those patients who have decompensated cirrhosis.
Causes
Most patients with the syndrome have thrombotic disorders. The causes of Budd-Chiari syndrome are as follows:
- Hematological disorders: polycythemia vera, paroxysmal nocturnal hemoglobinuria;
- pathological myeloproliferative conditions, antiphospholipid syndrome;
- essential thrombocytosis.
- deficiency of C and S protein;
- hydatid disease (cystic echinococcosis);
- Behçet's disease;
- hepatocellular carcinoma (liver cancer);
Use of oral contraceptives, pregnancy, and the puerperium have also been associated with Budd-Chiari syndrome .
Signs and symptoms
The clinical presentation of Budd-Chiari syndrome depends on how quickly the hepatic vein occlusion expands and whether a collateral venous network has been developed to decompress the hepatic sinusoids.
The syndrome can be classified as fulminant, acute, subacute or chronic .
In patients with the fulminant form of the syndrome, hepatic encephalopathy eight weeks after the development of jaundice. Patients with the acute form have short-term symptoms, intractable ascites and liver necrosis without the formation of venous collaterals (bypass tracts).
The subacute form is the most common and has a more insidious course. Hepatic ascites and necrosis may be minimal because the hepatic sinusoids are decompressed by the portal venous circulation. When Budd-Chiari syndrome is acute, thrombosis of all major hepatic veins is common compared with the subacute form, in which it is present in only one third of patients.
The chronic form is a complication of liver cirrhosis.
Abdominal pain, hepatomegaly (enlarged liver), and ascites are present in almost all patients with Budd-Chiari syndrome. However, asymptomatic patients have also been described. Nausea, vomiting and mild jaundice most often occur in fulminant and acute forms, while splenomegaly (enlarged spleen) and esogastric varices may be found in chronic forms. When the inferior vena cava is blocked, dilated venous collaterals are present on the flanks adjacent to the swelling of the legs.
Budd-Chiari syndrome. Photo
Venous dilatation of veins in Budd-Chiari syndrome
Manifestations of Budd-Chiari syndrome
Ulcerative colitis in Budd-Chiari syndrome
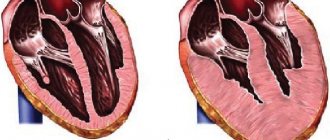
Normal hepatic veins (left) versus occluded veins (right)
Diagnostics
Signs that lead a doctor to suspect that a patient has Budd-Chiari syndrome are hepatomegaly, ascites, and high levels of liver enzymes found in blood tests. However, in order to resolve all doubts and find out the reasons that caused suspicious signs and symptoms, it is necessary to conduct the following studies:
- Doppler ultrasound of the liver , with a sensitivity and specificity of more than 85%, is the preferred method for examining the liver when Budd-Chiari syndrome is suspected. Necrotic areas of the liver and blood clots are observed.
- Magnetic resonance imaging (MRI) helps to highlight the venous circulation of the liver. It has a sensitivity and specificity of 90%. It is useful for examining the inferior vena cava and allows one to differentiate between acute, subacute and chronic forms of the syndrome.
- Computed tomography (CT) may be useful in determining the anatomy of the venous circulation and in transjugular intrahepatic portosystemic shunting.
- Liver venography may show blood clots in the hepatic veins.
- Echocardiography may be necessary in some patients to evaluate tricuspid regurgitation, constrictive pericarditis, or right atrial myxoma.
- A liver biopsy may be required to confirm the diagnosis and detect the development of cirrhosis.
Differential diagnosis:
- constrictive pericarditis;
- right-sided heart failure;
- metastatic liver disease;
- alcoholic liver disease;
- granulomatous liver disease.
Forecast
Factors associated with a favorable prognosis are young age at diagnosis, absence of large amounts of ascites, and low serum creatinine levels. Identifying the cause of Budd-Chiari syndrome using radioimaging (ultrasound, CT, MRI, etc.) has the greatest impact on the prognosis.
Drug and surgical treatment can prolong the life of patients up to a rough 8 years, after which liver transplantation is recommended.
Budd-Chiari syndrome. Epidemiology
Budd-Chiari syndrome is extremely rare and the exact incidence is unknown, although in one study, Dr. Rajani estimated the incidence to be about 1 case per million population per year in Sweden. Congenital membranous forms of Budd-Chiari syndrome are most common in Asia.
This syndrome predominantly occurs in women with hematological diseases.
The average age of diagnosis is 30–40 years, although the condition can also occur in children and the elderly.