Heart failure is a complex disorder that is accompanied by a decrease in myocardial contractility, pumping function and quality of blood flow throughout the body.
The disease is extremely dangerous, because the tissues experience ischemia, dystrophic as well as compensatory changes begin, which put an end to the normal functioning of the body in general. In addition to the heart itself, the liver, kidneys, brain, muscles, and lungs are affected.
Symptoms are not typical enough in the early stages, but pathology can be detected through preventive examinations. At a minimum, echo and electrocardiography are required.
The therapy is conservative, except for cases when medications alone cannot help the case. These are mainly congenital and acquired malformations of the heart and blood vessels; the issue of therapy is decided at the discretion of a specialist or group of doctors.
In any case, you need to act quickly. The disease tends to progress rapidly.
Development mechanism
It is difficult to say exactly how and why cardiac dysfunction is formed, because there are a huge number of pathogenetic factors that cause the disorder. Generally speaking, we can imagine an average picture.
The heart is affected by a negative factor. Most often we are talking about consistently high blood pressure, in which rapid depletion of the walls of a muscular organ is observed, or a heart attack (as a result of which cells die and are replaced by scar tissue).
Read more about post-infarction cardiosclerosis and methods of its treatment in this article.
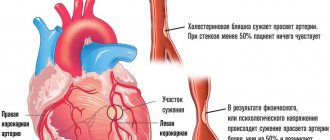
Also, chronic ischemic processes (for example, coronary insufficiency, in which the organ does not receive enough useful compounds and oxygen), atherosclerosis, in which the arteries supplying the heart become clogged and the intensity of trophism (nutrition) decreases, are considered as the primary mechanism, the “trigger” for the onset of pathology. .
Finally, a factor in the development of heart failure may lie in structural changes: against the background of congenital or acquired defects.
In any case, further transformation of the myocardium occurs. Typically, functional cells die and are replaced by scar tissue. The organ cannot contract with sufficient speed and force.
Pumping function decreases. The beats are sluggish, unable to adequately pump blood throughout the body.
The heart itself also suffers, since not enough necessary substances are supplied through the coronary arteries. The circle closes, it can only be broken by prescribing treatment, and then not in all cases. Until a certain point.
The progression of the pathological process, its speed, depends on the specific cause of the onset of the disorder. In some cases the count lasts for months, in others for many years.
It is contraindicated to hesitate in any situation; at the first symptoms you should consult a doctor.
If a disorder was discovered through a routine examination, it is recommended to continue the examination to establish an accurate diagnosis and determine the origin of the disorder.
Chronic heart failure
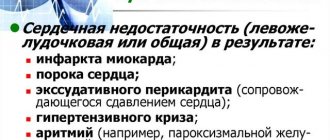
Chronic heart failure develops gradually due to compensatory mechanisms. It begins with an increase in the rate of heart contractions and an increase in their strength, arterioles and capillaries dilate, which facilitates emptying of the chambers and improves tissue perfusion. As the underlying disease progresses and compensatory mechanisms are exhausted, cardiac output steadily decreases. The ventricles cannot empty completely and become overfilled with blood during diastole. The heart muscle strives to push the blood accumulated in the ventricles into the arterial system and ensure a sufficient level of blood circulation, compensatory myocardial hypertrophy is formed. However, over time the myocardium weakens. Dystrophic and sclerotic processes occur in it, associated with a lack of blood supply and oxygen, nutrients and energy. The stage of decompensation begins. At this stage, the body uses neurohumoral mechanisms to maintain hemodynamics. Maintaining a stable level of blood pressure with a significantly reduced cardiac output is ensured by activating the mechanisms of the sympathetic-adrenal system. In this case, spasm of the renal vessels (vasoconstriction) occurs and renal ischemia develops, which is accompanied by a decrease in their excretory function and retention of interstitial fluid. The secretion of antidiuretic hormone by the pituitary gland increases, increasing water retention in the body. Due to this, the volume of circulating blood increases, the pressure in the veins and capillaries increases, and the leakage of fluid into the interstitial space increases.
Chronic heart failure, according to various authors, is observed in 0.5–2% of the population. The incidence increases with age; after 75 years, the pathology occurs in 10% of people.
Heart failure is a serious medical and social problem, as it is accompanied by high rates of disability and mortality.
Symptoms
External manifestations of heart failure are characterized by abnormalities in the lungs, central nervous system, and cardiovascular structures. The clinical picture directly depends on the stage of the disease. There are three main stages in total.
First stage
Latent or hidden. The pathological process develops, but the patient is unable to detect it.
There are no symptoms of heart failure and are detected only during critical physical exertion.
The average person does not achieve in everyday life even half of the mechanical activity indicator required to identify a problem, therefore the violation is often hidden and does not make itself felt.
Paradoxically, it is athletes and outdoor enthusiasts who are the first to discover the problem. They are not able to do their job well.
There is severe shortness of breath, an increase in heart rate to critical levels, and loss of consciousness is possible at the peak of an attack of failure.
At this stage, treatment makes sense. There is a possibility of complete recovery without consequences for the patient’s body. After correction of the condition, there are no contraindications for sports or active recreation.
Second stage (A)
The clinical picture is present with intense physical activity, but the threshold is much lower than in the early stage.
The clinical picture develops rapidly after a provoking factor (jogging, lifting a load to the floor), but also quickly disappears.
Typical signs of heart failure are chest pain, nausea, shortness of breath and a feeling of shortness of breath, increased heart rate. A cough without sputum production is detected. It occurs regularly and goes away quickly. This is a typical symptom of stagnation in the small (pulmonary) circle.
Read more about coughing in heart failure and how to distinguish it from an infectious one here.
Manifestations develop against a background of relative well-being at rest. At this stage, there is the possibility of a complete cure, because there are no critical changes in the myocardium yet.
Sports and intense physical activity are excluded. Light therapeutic exercises are possible. The issue is decided at the discretion of the doctors.
Second stage (B)
Symptoms of heart failure at the subcompensated stage are already noticeable even to the naked eye.
It is difficult to help radically, but it is still possible, but it will require a lot of effort on the part of doctors and the patient himself.
The blood flow in the small and large circles is disrupted, that is, the entire cardiovascular system suffers at once, this is dangerous because it can lead to cardiac arrest, a major heart attack, or stroke.
Among the clinical signs:
- Chest pain. Moderate to low intensity. Pressing, burning. Bursting. This type of discomfort directly indicates ischemic processes and insufficient quality trophism.
- Dyspnea. The problem is observed even at rest. The person is unable to walk normally, walking becomes unbearable. Not to mention climbing stairs or anything else. The question is often raised in the disability group.
- Increased liver size. Subjectively, it feels like a fullness in the right side, under the ribs. Pain syndrome is possible. Weak, aching.
- Cough. Unproductive, present almost constantly or occurs frequently, regularly. At first there is no sputum, but as it progresses there are episodes of hemoptysis. The separation of liquid connective tissue directly indicates stagnant processes in the small circle. This is an extremely alarming sign and will intensify as the disease progresses.
- Gurgling rales in the lungs when auscultated with a stethoscope. They can be noticeable without a special device.
- Swelling of the limbs. The legs are mostly affected (more details in this article). Then the hands and face are involved in the process.
Due to liver problems, the volume of the abdomen increases. The so-called ascites begins. Accumulation of fluid in the peritoneum, which can also be attributed to edema.
- Impaired consciousness. Due to poor oxygen supply to the brain, there is a high risk of fainting. This is also an alarming sign, because the body is no longer able to compensate for the disorder. The next stage is a stroke, usually extensive.
All these are symptoms of congestive heart failure, the chronic type. The acute version is accompanied by severe chest pain, shortness of breath, and disturbances in the functioning of internal organs.
This is a critical, emergency condition that can lead to the patient's immediate death. In the future, several minutes or, at most, hours, if medical assistance is not provided.
Third stage
Terminal or final. It develops after a few years, if we consider classic cases. In fact, it depends on the individual characteristics of the patient’s body and the reasons for the formation of the disease.
The clinical picture of the decompensated stage remains identical, but the intensity of the symptoms increases significantly. So, shortness of breath reaches a critical level. The patient cannot even take care of himself at home. Getting out of bed is already an achievement.
The issue of disability is resolved unambiguously; the person is completely disabled.
Massive catastrophic changes in internal organs are detected. Hence the symptoms from other systems: liver, brain, kidneys, etc.
In extremely rare cases, this moment is absent, then there is a chance of recovery through radical measures, through a heart transplant. Although they are not great. Otherwise, therapy does not make much sense. The mortality rate is close to 100%.
Signs of heart failure
Severe heart failure is accompanied by:
- gas exchange disorder;
- swelling;
- stagnant changes in internal organs.
Gas exchange disorder
Slowing down the speed of blood flow in the microvasculature doubles the absorption of oxygen by tissues. As a result, the difference between the oxygen saturation of arterial and venous blood increases, which contributes to the development of acidosis. Under-oxidized metabolites accumulate in the blood, activating the basal metabolic rate. As a result, a vicious circle is formed, the body requires more oxygen, but the circulatory system cannot provide these needs. A gas exchange disorder leads to the appearance of symptoms of heart failure such as shortness of breath and cyanosis.
For severe heart failure, shortness of breath and cyanosis occur
When blood stagnates in the pulmonary circulation system and its oxygenation (oxygen saturation) deteriorates, central cyanosis occurs. Increased utilization of oxygen in body tissues and slower blood flow cause peripheral cyanosis (acrocyanosis).
Edema
The development of edema due to heart failure is caused by:
- slowing down blood flow and increasing capillary pressure, which contributes to increased extravasation of plasma into the interstitial space;
- violation of water-salt metabolism, leading to retention of sodium and water in the body;
- a protein metabolism disorder that disrupts plasma osmotic pressure;
- decreased liver inactivation of antidiuretic hormone and aldosterone.
In the initial stage of heart failure, edema is hidden and manifests itself as pathological weight gain and decreased diuresis. Later they become visible. First, the lower limbs or the sacral area swell (in bedridden patients). Subsequently, fluid accumulates in the body cavities, which leads to the development of hydropericardium, hydrothorax and/or ascites. This condition is called hydrocele.
Heart failure is almost always accompanied by edema
Stagnant changes in internal organs
Hemodynamic disturbances in the pulmonary circulation lead to the development of congestion in the lungs. Against this background, the mobility of the pulmonary edges is limited, the respiratory excursion of the chest is reduced, and lung rigidity is formed. Patients develop hemoptysis, cardiogenic pneumosclerosis, and congestive bronchitis.
Congestion in the systemic circulation begins with an increase in the size of the liver (hepatomegaly). Subsequently, hepatocytes die and are replaced by connective tissue, i.e., cardiac fibrosis of the liver is formed.
In chronic heart failure, the cavities of the atria and ventricles gradually expand, which leads to relative insufficiency of the atrioventricular valves. Clinically, this is manifested by expansion of the borders of the heart, tachycardia, and swelling of the neck veins.
Signs of congestive gastritis are loss of appetite, nausea, vomiting, flatulence, tendency to constipation, weight loss.
With long-term chronic heart failure, patients develop cardiac cachexia - an extreme degree of exhaustion.
Congestion in the kidneys causes the development of the following symptoms of heart failure:
- hematuria (blood in the urine);
- proteinuria (protein in urine);
- cylindruria (casts in urine);
- increase in relative density of urine;
- oliguria (decreased amount of urine output);
Heart failure has a pronounced negative impact on the functions of the central nervous system. This leads to the development:
- depressive states;
- increased fatigue;
- sleep disorders;
- decreased physical and mental performance;
- increased irritability.
Clinical manifestations of heart failure are also determined by its type.
Signs of acute heart failure
Acute heart failure may be caused by decreased pumping function of the right ventricle, left ventricle, or left atrium.
Acute left ventricular failure develops as a complication of myocardial infarction, aortic disease, or hypertensive crisis. A decrease in the contractile activity of the left ventricular myocardium leads to an increase in pressure in the veins, capillaries and arterioles of the lungs, and an increase in the permeability of their walls. This causes blood plasma to sweat and the development of pulmonary edema.
Clinical manifestations of acute heart failure are similar to acute vascular failure, which is why it is sometimes called acute collapse.
Clinically, acute left ventricular failure is manifested by symptoms of cardiac asthma or alveolar pulmonary edema.
The development of an attack of cardiac asthma usually occurs at night. The patient wakes up in fear from sudden suffocation. Trying to alleviate his condition, he takes a forced position: sitting, with his legs down (orthopneic position). Upon examination, notice the following signs:
- pale skin;
- acrocyanosis;
- cold sweat;
- severe shortness of breath;
- in the lungs there is harsh breathing with isolated moist wheezing;
- low blood pressure;
- muffled heart sounds;
- the appearance of a gallop rhythm;
- expansion of the borders of the heart to the left;
- the pulse is arrhythmic, frequent, weak filling.
To alleviate the condition of acute heart failure, patients take the orthopneic position
With further increase in stagnation in the pulmonary circulation, alveolar pulmonary edema develops. Its symptoms:
- sudden suffocation;
- cough with pink, foamy sputum (due to blood);
- bubbling breathing with a lot of moist wheezing (a symptom of a “boiling samovar”);
- facial cyanosis;
- cold sweat;
- swelling of the neck veins;
- a sharp decrease in blood pressure;
- arrhythmic, thread-like pulse.
If the patient is not provided with urgent medical care, death will occur due to increasing cardiac and respiratory failure.
With mitral stenosis, acute left atrial insufficiency occurs. Clinically, this condition manifests itself in exactly the same way as acute left ventricular heart failure.
Acute right ventricular failure usually develops as a result of thromboembolism of the pulmonary artery (PE) or its major branches. The patient develops stagnation in the systemic circulation, which manifests itself:
- pain in the right hypochondrium;
- swelling of the lower extremities;
- swelling and pulsation of the veins of the neck;
- pressure or pain in the heart area;
- cyanosis;
- shortness of breath;
- expansion of the borders of the heart to the right;
- increased central venous pressure;
- a sharp decrease in blood pressure;
- thread-like pulse (frequent, weak filling).
Signs of chronic heart failure
Chronic heart failure develops in the right and left atrial, right and left ventricular types.
Chronic heart failure, according to various authors, is observed in 0.5–2% of the population. The incidence increases with age; after 75 years, the pathology occurs in 10% of people.
Chronic left ventricular failure develops as a complication of coronary heart disease, arterial hypertension, mitral valve insufficiency, aortic disease and is associated with stagnation of blood in the pulmonary circulation. It is characterized by gas and vascular changes in the lungs. Clinically manifested:
- increased fatigue;
- dry cough (rarely with hemoptysis);
- attacks of palpitations;
- cyanosis;
- attacks of suffocation, which often occur at night;
- shortness of breath.
In chronic left atrial insufficiency in patients with mitral valve stenosis, congestion in the pulmonary circulation system is even more pronounced. The initial signs of heart failure in this case are cough with hemoptysis, severe shortness of breath and cyanosis. Gradually, sclerotic processes begin in the vessels of the small circle and in the lungs. This leads to the creation of an additional obstacle to blood flow in the pulmonary circle and further increases the pressure in the pulmonary artery basin. As a result, the load on the right ventricle increases, causing the gradual formation of its failure.
Chronic left ventricular failure may manifest as a dry cough, sometimes with hemoptysis
Chronic right ventricular failure usually accompanies emphysema, pneumosclerosis, mitral heart defects and is characterized by the appearance of signs of blood stagnation in the systemic circulatory system. Patients complain of shortness of breath during exercise, enlargement and distension of the abdomen, a decrease in the amount of urine discharge, the appearance of edema of the lower extremities, heaviness and pain in the right hypochondrium. Upon examination, the following is revealed:
- cyanosis of the skin and mucous membranes;
- swelling of peripheral and cervical veins;
- hepatomegaly (enlarged liver);
- ascites.
Failure of only one part of the heart cannot remain isolated for a long time. In the future, it necessarily turns into general chronic heart failure with the development of venous stagnation in both the pulmonary and systemic circulation.
Characteristic signs of left ventricular failure
If you classify symptoms in detail, you need to start from the type of manifestation. As a rule, the onset of a pathological process does not affect all chambers of the organ. At least not right away. It takes time.
When the left parts of the cardiac structures are affected, predominantly disorders of the systemic circulation are observed. That is, both the organ itself and other systems suffer.
Typical clinical signs:
- Chest pain. They do not start immediately, but after some time. At the initial stage there are none.
- Arrhythmias. According to the type of sinus tachycardia. When the frequency of contractions increases significantly. As it progresses, fibrillation and extrasystole are detected.
- Headache, spatial disorientation, neurological dysfunction. Due to poor blood circulation in the brain. The list of symptoms is varied. These are mainly disorders of the sensory organs, and problems with thinking are possible.
- Pain in the right side. Enlarged liver. Accumulation of fluid in the abdominal cavity (ascites). Also yellowing of the skin (not always, relatively rarely), changes in biochemical blood parameters.
- Lower back pain. Increase in the amount of daily urine or its decrease. If there are disturbances in the filtering function of a paired organ of the excretory system, one is replaced by another.
- First, polyuria, when the volume of urine increases significantly, then the reverse process.
- Instability of blood pressure. In the initial stages of heart failure, an increase in the indicator is observed. Then it falls, even in patients with hypertension. This is a negative sign.
Symptoms are determined not only and not so much by the heart itself, but by disruptions in the functioning of other organs and systems. Read more about left ventricular heart failure here.
What is cardiovascular failure?
Cardiovascular failure is characterized by the fact that a negative process , which appears in it due to a dysfunction of the heart in the area of circulatory support, and, in addition, difficulty regulating blood flow to the main circulatory organ. Doctors distinguish several types of cardiovascular failure: it can be acute, chronic, or spread only to 1 half of the heart, left or right.
By this concept, experts also understand such conditions of the human body in which serious disturbances in the heart cycle , which subsequently leads to a decrease in the volume of the organ and a slowdown in its work. In the future, such a patient develops a general disease of the body, since the heart, which does not cope well with the function of providing oxygen and nutrition to all cells of the body, becomes the reason that starving cells are unable to fully function, and malfunctions begin to appear in the body’s functioning.
Typical manifestations of right ventricular failure
The disease begins with dysfunction of the small circle. Hence the pulmonary problems.
The list of symptoms is appropriate:
- Dyspnea. The intensity of this depends on the phase of the pathological process. First after strong physical exertion, and closer to the final stage of the disease at rest. A person becomes unable to work and cannot even take care of himself in everyday life.
- Cough. No sputum production. But this is also temporary. Then the blood leaves, which is provoked by stagnation in the small circle. The volumes can be significant.
- Increased pressure in the veins. It is especially noticeable in the example of the cervical vessels, which become inflated and protrude above the surface of the skin.
Heart failure is manifested by both disorders of the greater and lesser circles. However, not at one moment. The order is noted. Apart from acute cases, which are minimal.
Read more about right ventricular HF in this article.
Acute heart failure
Acute heart failure most often develops as a complication of severe forms of arrhythmia (paroxysmal tachycardia, ventricular fibrillation), acute myocarditis or myocardial infarction. The ability of the myocardium to effectively contract is sharply reduced, which leads to a drop in cardiac output, and a significantly smaller volume of blood enters the arterial system than normal.
Acute heart failure may be caused by decreased pumping function of the right ventricle, left ventricle, or left atrium. Acute left ventricular failure develops as a complication of myocardial infarction, aortic disease, or hypertensive crisis. A decrease in the contractile activity of the left ventricular myocardium leads to an increase in pressure in the veins, capillaries and arterioles of the lungs, and an increase in the permeability of their walls. This causes blood plasma to sweat and the development of pulmonary edema.
Clinical manifestations of acute heart failure are similar to acute vascular failure, which is why it is sometimes called acute collapse.
Causes
Development factors are diverse. They are well known to doctors:
- Arterial hypertension. Moreover, the current one has been going on for a long time. Increase in pressure.
- Previous myocardial infarction. The probability of violation is especially high in the first six months or a little more.
- Inflammatory, including autoimmune or infectious processes in cardiac structures. For example, myocarditis or others.
- Congenital or acquired heart defects. Aortic, mitral stenosis, also vascular abnormalities (coarctation of the aorta). There are many of them.
- Diseases of the endocrine system. Diabetes mellitus, low production of thyroid hormones (thyroid gland substances).
- Rarely - heart tumors. Insufficiency is also possible against the background of cancer pathologies of any localization at advanced stages.
Patients prone to smoking and alcohol abuse are in the high-risk category. Experienced drug addicts. Quitting a bad habit can make a big difference.
Causes of heart failure
The main causes of heart failure are:
- coronary heart disease and myocardial infarction;
- dilated cardiomyopathy;
- rheumatic heart defects.
In elderly patients, the causes of heart failure are often type II diabetes mellitus and arterial hypertension.
Type 2 diabetes can lead to heart failure
There are a number of factors that can reduce the compensatory mechanisms of the myocardium and provoke the development of heart failure. These include:
- pulmonary embolism (PE);
- severe arrhythmia;
- psycho-emotional or physical stress;
- progressive coronary heart disease;
- hypertensive crises;
- acute and chronic renal failure;
- severe anemia;
- pneumonia;
- severe ARVI;
- hyperthyroidism;
- long-term use of certain medications (adrenaline, ephedrine, corticosteroids, estrogens, non-steroidal anti-inflammatory drugs);
- infective endocarditis;
- rheumatism;
- myocarditis;
- a sharp increase in the volume of circulating blood due to incorrect calculation of the volume of intravenously administered fluid;
- alcoholism;
- rapid and significant weight gain.
Eliminating risk factors can prevent the development of heart failure or slow its progression.
Diagnostics
The examination is carried out by cardiology specialists. You need to act quickly so as not to miss the right moment to correct the condition. The list of events is approximately the same.
- Oral questioning of the patient. To create a complete clinical picture and put forward hypotheses regarding the diagnosis.
- Anamnesis collection. Past illnesses, lifestyle, habits, family history and other factors are subject to clarification.
- Blood pressure measurement. Also heart rate.
- Daily assessment of the same indicators using Holter monitoring. Gives a lot of information.
- Electrocardiography. To determine the functional state of the heart. Requires careful decoding. In the hands of a competent doctor it is a valuable source of useful information.
- Echocardiography. Makes it possible to visualize tissues of cardiac and surrounding structures. Diagnostics cannot do without this. Makes it possible to assess the degree of organic changes.
- Specialized tests. Used for early detection of cardiac failure. They are physical in nature and include loads (squats). Therefore, they are contraindicated at advanced stages, starting from the second. Complications are likely.
- Biochemical and standard clinical blood tests.
- Ultrasound of the liver, kidneys. To assess the degree of involvement of these organs in the pathological process.
- MRI of the heart and brain if necessary. Rarely required.
- Duplex scanning of cerebral structures. To understand how well they are supplied with nutrients and oxygen.
- Chest X-ray. As part of the diagnosis of lung function disorders.
This is not an exhaustive list. The disease is multifaceted, therefore, at the discretion of the specialist, the list can be changed in one direction or another.
What types are there
Depending on the speed of development of the disease, the pathology is:
- Spicy. Its appearance occurs over several minutes or hours. In this case, pulmonary edema, cardiogenic shock, and cardiac asthma are observed. Usually this condition is caused by myocardial infarction, rupture of the walls of the left ventricle, acute mitral or aortic valve insufficiency.
- Chronic. Pathology takes weeks, months, years to form. The problem arises with heart defects, arterial hypertension, chronic respiratory failure, and prolonged anemia.
Chronic heart failure is divided into several classes:
- First. The patient suffers from shortness of breath while climbing stairs. Physical activity is not affected.
- Second. When a person walks quickly or climbs to the first floor, breathing becomes difficult. Normal loads cause manifestations of insufficiency.
- Third. Light loads and even walking are accompanied by deterioration in well-being.
- Fourth. Even at rest, a person feels shortness of breath and other symptoms, and the slightest stress seriously worsens the condition of the heart.
Chronic failure is considered the most common pathology among disorders of the cardiovascular system.
Depending on the location of the lesion, the following is observed:
- Left ventricular failure. Its development is associated with overload of the left ventricle due to deterioration of myocardial contractility. Overload is observed when the aorta narrows, and contractile dysfunction occurs during a heart attack. In this case, stagnant processes develop in the pulmonary circulation.
- Right ventricular. It is associated with right ventricular overload due to pulmonary hypertension. The last stage is dystrophic processes. The patient suffers from edema, cachexia, and skin changes.
- Mixed. In this case, lesions of the right and left ventricles are combined.
Depending on the characteristics of the origin, the pathological process is:
- Myocardial. In this case, the disorders are associated with direct damage to the walls of the heart, which impair energy metabolism. The condition is characterized by weakening of the systole and diastole of the heart.
- Reloading. It is caused by excessive stress on the organ. This occurs in cases of defects and diseases that interfere with normal blood flow.
- Combined. Myocardial damage is combined with increased load on the heart.
Also read: Diffuse small focal cardiosclerosis - mortality rate
Treatment methods
The therapy is conservative. Medicines from several pharmaceutical groups are used:
- Cardiac glycosides. Allows you to normalize myocardial contractility. At the same time, they reduce the muscle organ’s need for oxygen, enhance metabolic processes, increasing, figuratively speaking, efficiency when using available resources. Digoxin, tincture of lily of the valley and others are actively prescribed. According to indications.
- Antihypertensive medications. ACE inhibitors (Perindopril), beta blockers (Anaprilin, Carvedilol), calcium antagonists (Diltiazem, Verapamil), centrally acting agents (Moxonidine) and others. If you have high blood pressure.
- Diuretics. Diuretics when the situation requires it. For example, when the heart and kidneys fail and swelling begins.
Removing excess fluid allows you to reduce the load on all organs. This is a necessary part of treatment. But you cannot consume such medications for a long time.
Loop diuretics (Furosemide, Lasix) are used as emergency medications.
In other situations, it is sufficient to prescribe thiazide or potassium-sparing tablets (Veroshpiron, Spironolactone, Hydrochlorothiazide)
- Means for normalizing metabolic processes in the heart, cardioprotectors. Mildronate, Riboxin.
Surgical therapy is required if there are structural or anatomical disorders. For example, prosthetics of valves, blood vessels, artificial dilatation of arteries when they are narrowed, and other options.
The last resort is a heart transplant. The operation is complex, but has extremely high survival rates. About 10% of all patients die. However, the problem is the lack of donors.
In the future, as an auxiliary measure, it is recommended to change lifestyle: normalize body weight, adjust the diet under the supervision of a nutritionist, give up alcohol and tobacco products, and limit physical activity. If possible, you should also avoid stressful situations.
Attention:
Changing your diet should be carried out under the supervision of a doctor. Heart failure is demanding in terms of microelements and essential substances. You can only make things worse on your own.
Treatment of heart failure
In case of heart failure, therapy is aimed primarily at the underlying disease (myocarditis, rheumatism, hypertension, coronary heart disease). Indications for surgery may include adhesive pericarditis, cardiac aneurysm, and heart defects.
Strict bed rest and emotional rest are prescribed only to patients with acute and severe chronic heart failure. In all other cases, physical activity that does not cause deterioration in well-being is recommended.
Heart failure is a serious medical and social problem, as it is accompanied by high rates of disability and mortality.
In the treatment of heart failure, a properly organized diet plays an important role. Dishes should be easily digestible. The diet should include fresh fruits and vegetables as a source of vitamins and microelements. The amount of table salt is limited to 1-2 g per day, and liquid intake to 500-600 ml.
The diet of patients with heart failure should include fresh vegetables and fruits
Pharmacotherapy, which includes the following groups of drugs, can improve the quality of life and prolong it:
- cardiac glycosides – enhance the contractile and pumping function of the myocardium, stimulate diuresis, and increase the level of exercise tolerance;
- ACE inhibitors (angiotensin-converting enzyme) and vasodilators - reduce vascular tone, expand the lumen of blood vessels, thereby reducing vascular resistance and increasing cardiac output;
- nitrates - dilate the coronary arteries, increase cardiac output and improve blood filling of the ventricles;
- diuretics – remove excess fluid from the body, thereby reducing swelling;
- β-blockers - increase cardiac output, improve the filling of the heart chambers with blood, reduce the heart rate;
- anticoagulants - reduce the risk of blood clots in blood vessels and, accordingly, thromboembolic complications;
- agents that improve metabolic processes in the heart muscle (potassium supplements, vitamins).
If cardiac asthma or pulmonary edema (acute left ventricular failure) develops, the patient requires emergency hospitalization. Prescribed drugs that increase cardiac output, diuretics, nitrates. Oxygen therapy is mandatory.
Removal of fluid from body cavities (abdominal, pleural, pericardial) is carried out by puncture.
Possible consequences
The main complications are cardiac arrest, massive heart attack, stroke. The end result is the death of a person or at least severe disability.
Heart failure is a dangerous and complex pathology. She does not tolerate delays or frivolous attitudes. If you do not react in time, there will be no chance of recovery. Therefore, it is necessary to contact a cardiologist or at least a therapist once every six months to undergo preventive examinations.
Bibliography:
- Russian Cardiological Society. Clinical recommendations. Chronic heart failure (CHF).
- Monthly scientific and practical journal Cardiology. Volume 58.
- Republican Center for Health Development of the Ministry of Health of the Republic of Kazakhstan. Chronic heart failure Clinical protocols of the Ministry of Health of the Republic of Kazakhstan.
Prevention
The recommendations are classic.
- Visit a cardiologist regularly, undergo examinations every six months to a year. Especially if there is a predisposition to pathologies. There is a chance to identify deviations at the first stage.
- Stop smoking, alcohol, psychoactive substances and uncontrolled use of drugs. Especially anti-inflammatory ones.
- Normalize the level of physical activity. Excess and deficiency are equally harmful. It is better to limit yourself to walking for 1-2 hours a day.
- Have a full rest. Sleep at least 7 hours per night.
- Learn ways to relax and avoid stress. If possible.
Chronic heart failure in most cases develops over many years and does not make itself felt for a long period of time. High-quality treatment in the early stages guarantees a favorable outcome.
Causes of pathology in women
Heart failure in women develops under the influence of various factors. It can result from pathologies of the heart system, blood vessels, and other painful conditions that do not have a direct connection with the myocardium. Here is a list of the most significant reasons for the development of the syndrome in women:
- Pathologies of the cardiovascular system.
- Heredity.
- Diabetic disease.
- High blood pressure.
- Anemia.
- Thyroid diseases.
- Complications after infections that occur with fever.
- Sedentary lifestyle.
- Bad habits: smoking, alcohol, drugs.
- Problems with the environmental situation in the region of residence.
- Regular stressful situations.
- Excessive physical activity.
- Lack of sleep.
- Frequent overwork.
- Excess body weight.
Cardiovascular pathologies that provoke the formation of the syndrome:
- Cardiac ischemia (angina pectoris, myocardial infarction, arrhythmia).
- Congenital anomalies of the myocardium (aortic valve insufficiency).
- Cardiomyopathy (change in the structure and size of the myocardium).
Any changes require diagnosis and treatment. If they are not treated in time, HF can cause death. In women, pathology usually develops somewhat later than in men. The reason is a failure of hormones in the body during menopause.
On a note! In women after 50, the risk of developing vascular sclerosis, diabetic disease or hypertension sharply increases.
It is against the background of these pathologies that HF is formed. This is not a separate diagnosis, but a syndrome that develops due to some diagnosis.