The mitral configuration of the heart is one of the variants of the pathological configuration. Often occurs when patients are diagnosed with mitral stenosis. This deviation is detected during an X-ray examination.
In this case, the doctor must take into account that in the pictures the shape of the heart is a variable value. The main factors determining it are the position of the patient’s body in space, the height of the dome and the bluntness of the diaphragm angle in the intercostal space.
Important! The contours of the heart have gender and age differences. However, a normal cardiac shadow on an x-ray of the intercostal space has an elongated oval shape, located obliquely in relation to the spine of the human body.
What is the configuration of the heart, its indicators are normal
The configuration of the heart is the shape, contours, showing the expansion or contraction of the atria, ventricles, and vascular bundle. It includes the borders (upper, left and right), waist (narrowing at the junction of the bundle of blood vessels to the left ventricle), angles between the diaphragm (reflecting the inclination of the axis) and the arcs of the chambers of the heart. If the configuration is normal, this means that they correspond to the parameters (see table) of healthy people:
- relative dullness of the heart (its actual size) in the chest and absolute (the part that is not covered by the lungs and is directly adjacent to the ribs);
- length (length) and width (diameter);
- waist (retraction of the contour, narrowing of the diameter);
- there are angles between arcs.
| Contour type and main parameters | How was she educated? | Upper | Left | Right |
| Relative Dullness | Real contours | Bottom of 3rd ribs on the left edge of the sternum | The fifth intercostal space is 1.5 cm to the right from the conditional line drawn from the middle of the left clavicle | The fourth intercostal space is 1 cm to the right from the edge of the sternum |
| Absolute | Right ventricle | Bottom of 4th ribs on the left edge of the sternum | 2.5-3.2 cm to the right of the line from the middle of the left clavicle | Fourth intercostal space along the left edge of the sternum |
| Width of the bundle of large vessels (vascular) | Aorta, pulmonary artery, veins | The space between the 2nd and 3rd ribs does not extend beyond the borders of the sternum (approximately 4.5-5.5 cm) | ||
| Right contour (arcs) | Superior vena cava, right atrium | The edge of the sternum to the 3rd rib and the third or fourth space between the ribs 1 cm to the right | ||
| Right atriovasal angle | Between the superior vena cava and the atrium | 3-4 intercostal space | ||
| Cardio-phrenic angle right | Diaphragm, right atrium | 5th intercostal space | ||
| Left contour (arches) near the left edge of the sternum | Aorta | 1st intercostal space | ||
| Pulmonary artery | 2nd intercostal space | |||
| Left atrium | Level 3 ribs | |||
| Left ventricle | Inferior to the 3rd rib, just behind the left atrial appendage | |||
| Waist | Bundle of blood vessels, left ventricle (left), right atrium (right) | Level 3 ribs | ||
| Length | Heart length | From the apex to the right cardiophrenic angle the length should be between 11.5-12.7 cm | ||
| Diameter | Width of relative cardiac dullness | From the right border to the midline and from the left (the most protruding part) to the middle, normally 11-13 cm | ||
If the patient has diseases of the heart and/or large vessels, especially valve defects, then the load on its parts changes. Then the atria and ventricles enlarge, which is manifested by a shift in the boundaries of relative and absolute dullness, changes in size, smoothing of angles, and disappearance of the waist.
Determination of heart configuration by percussion
To determine the configuration of the heart, you first need to find the boundaries of dullness. They are so named because they can be examined during a medical examination. To do this, use the percussion (tapping) method. Above the lungs, the sound is clear, since they are filled with air, and as soon as the finger reaches the contour of the heart, dullness appears (relative dullness), and then a completely dull sound (absolute).
First, the true border of the heart is found in the chest. To do this, the finger of the left hand moves from the outside to the center. Since the organ’s entire surface is not adjacent to the chest, part of it is covered by the lungs, and a small area remains open, when tapping it can be identified by a dull (dull) sound. This zone (absolute dullness) reflects the size of the right ventricle. It is found by moving from the center to the edges.
When the boundaries of cardiac dullness change
An increase in the relative dullness of the heart is a ghost of expansion of its cavities (ventricles and atria). Occurs with valve defects, high blood pressure, weakening of the heart muscle or its hypertension (thickening). The absolute dullness of the heart can also change normally - for example, with bloating or pregnancy, the diaphragm rises upward and brings the heart closer to the ribs.
Expansion may be affected by:
- compaction of lung tissue (pneumosclerosis);
- adhesions in the chest;
- dilatation of the right ventricle.
Emphysema (increased airiness), an asthma attack, a low position of the diaphragm with weakness of the respiratory muscles can reduce the area.
X-ray configuration
If the boundaries of dullness (relative and absolute) can be found only by tapping, then measurements of length, width, finding the waist, angles and arcs of the configuration occur only on a chest x-ray. In the conclusion, the radiologist indicates the conformity of the configuration to a certain type and measures the angles, length and diameter.
It is important to understand that X-ray diagnostics will only show an expansion of the heart shadow or its displacement, an unusual shape, but to determine the cause, an ultrasound (echocardiography) will often be required. Only the latter method will help to study the movement of blood through the valves, the contractility of the heart muscle and its thickness.
Expert opinion
Alena Ariko
Expert in Cardiology
An atypical configuration of the heart is not always a sign of illness. For example, young women may have a cardiac shadow shape that is close to the mitral shadow, while older overweight patients may have an aortic shadow shape. Therefore, a diagnosis is never made based on X-ray findings alone.
Types of heart configuration
The following types of heart configurations have been identified:
- normal - the right angle between the vascular bundle is approximately in the middle, the second and third arches are almost equal (2 cm each);
- aortic – the waist is rarely emphasized;
- mitral - expansion mainly to the left, partially to the right, no waist;
- close to geometric figures: trapezoid, ball, triangle;
- “bullish” with a significant increase in all cameras.
Diagnostics
To correctly diagnose aortic insufficiency, a specialist needs to evaluate the results of the following studies:
- chest x-rays;
- electrocardiograms;
- phonocardiography;
- echocardiography;
- dopplerography.
To diagnose aortic stenosis, you need to perform:
- electrocardiogram;
- X-ray;
- transthoracic echocardiography;
- transesophageal echocardiography;
- Dopplerography;
- catheterization of cardiac chambers.
Waist Heart
The cardiac waist is the junction of the vascular bundle (arteries and veins entering and exiting the heart) into the left ventricle. Its apex is the left atrium, so when it enlarges, the waist disappears. With the expansion of the left ventricle, the waist will be well defined, “emphasized”.
Diameter of the heart
To measure the diameter of the heart, the midline of the body is visually determined, and from it the distances to the right and left edges of the relative dullness of the heart are measured. In a healthy person of average build, the right size does not exceed 4 cm, and the left - 9 cm; for thin people, a decrease of 1 cm is allowed.
The right diameter is larger than normal when:
- expansion of the right chambers (atrium and/or ventricle);
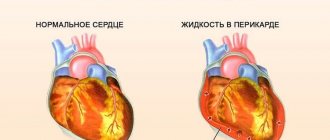
- accumulation of fluid in the pericardial sac (exudative pericarditis);
- displacement of the heart shadow to the right due to the large left ventricle.
The left size increases with diseases of the left chambers of the heart, less often it is shifted by the dilated right ventricle.
Normal dimensions of the vascular bundle
The vascular bundle is formed by the aorta or superior vena cava on the right and the pulmonary artery on the left; its size normally does not exceed 5-6 cm. It is covered by the sternum and does not protrude beyond its edges. If its width is greater, then this may be a sign of an aortic aneurysm or atherosclerosis.
Right heart contour
The right contour of the heart includes only 2 arches. The first is the superior vena cava or the ascending aorta (they are very close), and the second is always represented by the right atrium. Between these arches there is an angle called the right atriovasal.
Its location determines the configuration of the heart:
- normally it is approximately in the middle (between equal arcs);
- with mitral it is displaced upward;
- with aortic it moves down;
- with trapezoidal, triangular, spherical it disappears.
Left outline
The left contour includes the arcs:
- the first is part of the descending aorta;
- the second is the pulmonary artery;
- third - left atrium;
- the fourth is the left ventricle.
With a mitral configuration, they are all present, but shifted to the left. With aortic, the first and second arches, as well as the third and fourth, merge, the angle (left atriovasal) between the second and third is sharply expressed. If the patient has a trapezoid or a ball, then there is only the first arch, the angle, and the other three are connected into one large line .
Treatment
In most clinical situations, patients diagnosed with aortic regurgitation progress slowly. If such a patient receives adequate therapy in a timely manner, the further development of the pathology can be stopped.
If stenosis is diagnosed, then treatment tactics depend on the degree of narrowing of the lumen. For minor stenosis, pharmacological agents are prescribed that improve blood supply to the myocardium, eliminate oxygen starvation of tissues, and normalize heart rate and blood pressure.
Conservative treatment
The following groups of drugs can be prescribed as symptomatic therapy:
- calcium channel blockers (Verapamil);
- diuretics (Furosemide, Torasemide);
- beta blockers (Propranolol);
- antianginal drugs (Titrong, Sustak);
- vasodilators (Hydralazine);
- antibacterial drugs (Bcillin).
Surgery
Surgeon intervention is indicated in situations of aortic insufficiency when the LV can no longer cope with the incoming blood volume. For congenital aortic valve disease, surgery is performed no earlier than the patient reaches 30 years of age. In the event of an increase in negative symptoms or a sharp deterioration in health, intervention is performed earlier. In the case of an acquired defect, the age at which surgery is necessary is determined by the severity of hemodynamic disturbances and the patient’s condition. Most often, this tactic is used in patients 55-65 years old.
Indications for surgical intervention:
- impaired LV function;
- LV enlargement more than 6 centimeters;
- presence of negative symptoms;
- regurgitation of blood in diastole – more than 25-30% of the total volume;
- asymptomatic, but the volume of regurgitation is 50%.
Operation fails:
- if the patient’s age is over 69-70 years;
- the volume of regurgitation exceeds 65%;
- the presence of severe somatic pathologies.
Types of surgical intervention: intra-aortic balloon counterpulsation and artificial valve implantation. Indications for surgical intervention for stenosis include a decrease in the patient’s ability to work, quality of life, and moderate and severe stenosis (hole diameter below 1.5 cm²).
Types of operations:
- balloon aortic valvuloplasty;
- aortic valve replacement.
Traditional methods of treatment
As an addition to the main therapy, it is possible to use medicinal herbs. To strengthen and restore normal functioning of the cardiovascular system, it is recommended to use plants that contain bioflavonoids. These include:
- pine bark;
- nuts;
- grape:
- red wine;
- red clover;
- dog-rose fruit;
- buckwheat;
- hawthorn;
- spiraea;
- sea cabbage.
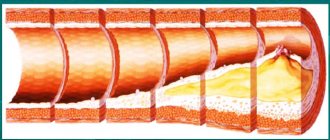
Attention! For atherosclerosis, it is recommended to use a combination of flower honey with fresh onion juice, sea cabbage, garlic, gooseberries, currants, blueberries, strawberries, chokeberries.
Means for strengthening blood vessels: recipes
To strengthen the vascular wall and normalize vascular tone, you can use the following mixtures and decoctions:
- Garlic tincture. Take 3 heads of garlic, peel them, pour in 500 ml of vodka. Leave to infuse in a dark, dry place for three weeks, strain. Drink 20 drops three times a day before meals, dilute with water. The course of therapy is two months.
- Grind 4 kg of celery, several heads of garlic, 7 lemons, 300 g of horseradish. Stir and leave in a warm place for 24 hours. Place in a cool and dark room for three days. Drink the resulting juice on an empty stomach, one teaspoon three times a day. The product is not recommended for use by patients diagnosed with gastritis or peptic ulcer.
- Tincture of golden mustache. The plant contains quercetin, which is an antioxidant. To prepare the tincture, you need to take 30 parts of the plant and add 1.5 liters of alcohol. Leave to infuse for two weeks. Before use, one spoon of tincture is mixed with a spoon of vegetable oil and drunk on an empty stomach, two hours before meals. The treatment course is 10 days, followed by a five-day break.
Special pathological forms of the heart
Special pathological forms of the heart include pulmonary and bovine.
Pulmonary heart
With cor pulmonale, the load on the right side increases, which leads to dilation of the atrium and ventricle. The X-ray shows an expansion of the shadow to the right (2nd arc) and a displacement of the left contour due to the large right ventricle, a mitral configuration appears.
Chronic diseases of the bronchi and lungs, which last for several years, are accompanied by cor pulmonale in 25% of cases. It can also occur acutely when the chest and diaphragm are damaged within a few hours.
If the patient is severely obese, then excess fat raises the diaphragmatic dome upward, which makes breathing difficult and causes changes in the heart shadow. Subacute cor pulmonale (develops up to 3-7 days) occurs when a pulmonary artery is blocked by a blood clot, severe pneumonia, tumor metastases, poliomyelitis, muscle weakness (myasthenia gravis).
Bull's heart
Enlargement of the chambers of the heart (dilated cardiomyopathy) or thickening of the heart muscle (hypertrophic cardiomegaly) leads to the fact that the cardiac shadow increases in all directions and a “large” or “bull” heart is formed.
Its configuration will be close to trapezoidal or spherical, less often the waist will be preserved.
The causes of large heart syndrome may be:
- atherosclerosis, angina pectoris, heart attack and its complications: aneurysm, post-infarction cardiosclerosis;
- vices;
- hypertonic disease;
- inflammation of the myocardium, immune or due to rheumatism, bacterial, viral, fungal infections;
- cardiomyopathy due to alcoholism, contact with chemicals, metals, industrial dust;
- severe hypovitaminosis, nutritional deficiency, especially lack of protein, when the heart muscle is weakened and stretched.
The expansion of the chambers of the heart leads to poor circulation, stagnation of blood in the lungs, edema, and enlargement of the liver.
We recommend reading the article about x-rays of the heart. From it you will learn what an x-ray of the heart shows, why x-rays are needed in three projections, with contrast of the esophagus, as well as how to prepare for x-rays of the heart and what the results will tell you. And here is more information about the structure of the human heart.
The configuration of the heart can be normal: 2 arches on the right, 4 on the left, there is a waist. With defects of the heart, large vessels, diseases of the lungs, myocardium, a mitral, aortic, trapezoidal shape appears, and pulmonary and “bull” hearts can be detected on an x-ray. Just a change in configuration does not indicate the presence of a disease.
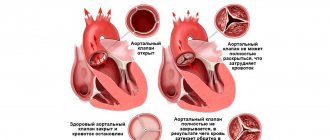
General characteristics of aortic valve disease
Aortic heart disease (ICD-10 code – I35) is a disease accompanied by disturbances in the structure of the valve leaflets and their functioning. There are several types of pathological process that cause different symptoms and complications.
The clinical picture is as follows:
- Pain in the region of the heart.
- Pale or cyanotic skin.
- Dyspnea.
- Cough.
- Attacks of dizziness.
- General weakness.
- Loss of consciousness.
- Swelling of the lower extremities.
- Pulsation of blood vessels.
- Increased heart rate.
- Blood pressure abnormalities.
Often in the early stages the defect does not manifest itself at all, and this can last for a long time.
The heart is one of the main organs of the body; it pumps blood in the body. His illness affects the entire body as a whole.
Change in the vascular bundle
The cardiac contours, which are determined in the second intercostal space on all sides, correspond to the size of the vascular bundle. In a healthy person, its right part runs along the right border of the sternum. At the end of the vascular bundle, the aorta is formed. The left border runs along the left edge of the sternum. Here, at the end of the vascular bundle, the pulmonary artery is formed.
Other reasons for changes in the vascular bundle are associated with diseases that are accompanied by the appearance of additional tissue. This could be, for example, goiter, enlarged lymph nodes, the presence of primary tumors or metastases. Dilation of the vascular bundle appears with atherosclerosis of the aorta, aortic aneurysm, dilation of the pulmonary artery, and increased blood pressure.
Why does stenosis develop?
The left atrioventricular orifice is narrowed due to:
- Long-term and severe overload of the atrium and ventricle;
- Rheumatism (current or previously suffered). But about 20 percent of patients with confirmed mitral valve pathology may not have rheumatic fever;
- Congenital pathology - narrowing of the left atrioventricular orifice. This disease can develop against the background of other, less serious heart defects;
In case of inflammation of the endocardium, mitral stenosis usually does not appear. However, some patients who have received improper treatment for infective endocarditis develop signs of mild stenosis with minor hemodynamic disturbances in the heart.
Causes of the disease
Aortic defects can be congenital or acquired. Among the causes of congenital defects, the leading ones are genetic, exogenous, and maternal pathologies. If a severe combined heart defect is detected in newborns, then surgery is performed from the age of six months, and some babies require surgery immediately after birth.
The causes of acquired defects can be different.
Provokes pathology:
- infectious or rheumatic endocarditis,
- atherosclerotic changes,
- visceral syphilis,
- injuries,
- damage resulting from surgical interventions,
- dissecting aneurysm,
- hypertension.
These factors lead to various heart defects. An organically damaged valve ceases to perform its normal function, which causes cardiovascular failure. As a result of the worsening of the pathology, patients stop performing physical work; upon passing the commission, they are given a disability group.
Types of pathology
The types of violations are as follows:
- stenosis (narrowing) of the aortic valve - the defect consists of narrowing of the aortic orifice compared to the norm,
- aortic insufficiency - incomplete closure of the aortic opening,
- combined pathology or combined defect, in which both stenosis and aortic insufficiency occur.
Heart defects occur both from birth, they are called congenital, and they can also be acquired, developing throughout life due to various pathologies. In each case, the severity of the heart defect is different, which is reflected in the functioning of the organ.