DIC syndrome in medicine refers to disseminated intravascular coagulation. Previously, the term “thrombohemorrhagic syndrome” was used. It is a complex of changes in the vascular network, a set of biochemical substances and cells that ensure the coagulation process.
Not being a separate disease, DIC syndrome becomes a threatening serious complication. The severity may exceed the danger of the disease itself or proceed unnoticed, detected only by laboratory indicators.
Clinically expressed by a changing or constant picture of microthrombosis of the vascular bed, hemorrhagic rashes and associated impaired microcirculation.
What is the essence of the appearance of DIC syndrome?
The main “culprits” in the pathophysiology of DIC are factors accumulated in the blood that actively influence the clotting mechanism or platelet aggregation. They are released from the cellular space in large quantities, for example, during massive injuries, extensive operations, during childbirth and during massage of the uterus, manual separation of the placenta, and acute myocardial infarction.
Cell death is caused by mechanical crushing and necrosis. At the same time, tissue thromboplastin is released from them. Under normal conditions, it provides tissue protection and prevents blood loss.
A similar ability has been proven for bacterial enzymes (staphylocoagulase), antibody complexes that arise against the background of infectious diseases, autoimmune processes, and vasculitis.
A provoking effect in DIC syndrome can be an uncontrollable stressful situation, since the increased release of catecholamine hormones (adrenaline, norepinephrine) and their accompanying substances, kinins, also activates intravascular coagulation.
In the pathogenesis (mechanism of formation) of the syndrome, there are three possible ways of activating coagulation inside blood vessels:
- external - substances with thromboplastin action come from tissues;
- internal - activation factors are located inside the vessel and are represented by immune complexes of antibodies, tissue thromboplastin, protease enzymes of leukocytes, tumor decay products during malignant degeneration, which damage the inner lining of the arteries;
- platelet - platelets, when in contact with damaged endothelium or foreign agents, stick together and release catecholamines and thrombin into the blood.
Equally important is the pathophysiological mechanism of decreased activity with subsequent depletion of the anticoagulant system: the content of the main natural anticoagulants - antithrombin III, plasminogen, protein C - decreases. If in a healthy person the level of antithrombin III fluctuates between 60-120%, then at the time of surgery it decreases by 1/5 Part. This serves as a serious provocation for the development of a backlash.
The severity of DIC syndrome is determined by the underlying disease, the degree of trauma of the surgical intervention, and the resulting tissue damage.
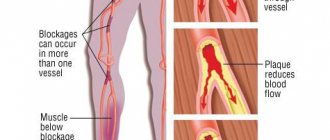
The result of biochemical changes is the formation of tiny blood clots in capillaries and vessels, which block blood circulation in target organs (brain, kidneys, adrenal glands, liver, intestines and stomach). Destructive processes, dystrophy and functional failure appear in them. Taking into account the simultaneous damage to several organs, it is called “multiorgan”.
Next, the process of activation of local fibrinolysis begins in areas of microthrombosis. Increased consumption of fibrinolysin and platelets leads to a change from hypercoagulation to increased bleeding, which is manifested by bleeding.
A serious stage of pathogenesis is considered to be the manifestation of impaired barrier protection of the damaged mucous membrane of the intestines and stomach. It leads to severe sepsis and intoxication of the body.
Causes and dangers of DIC syndrome
Disseminated intravascular coagulation occurs with accelerated formation of blood clots in response to shock, massive trauma, severe infection, and obstetric pathology.
It is characterized by bleeding due to the massive consumption of factors responsible for stopping it. May be asymptomatic or lead to acute respiratory and renal failure. To make a diagnosis, you need to take into account the symptoms and conduct blood tests. Treatment involves the administration of anticoagulants, antiplatelet agents, transfusion of blood or its components, and plasmapheresis. Read more in this article.
What is DIC syndrome?
Due to the influence of pathological factors, loose thrombotic masses, microthrombi, and accumulations of platelets are formed in small vessels.
They disrupt blood circulation, microcirculation, lead to oxygen starvation, and dysfunction of internal organs. Most dystrophy and cell destruction affect the parenchyma of the kidneys, lungs, liver and adrenal glands.
This is explained by the developed microcirculatory vascular network in them.
The danger of thrombohemorrhagic syndrome lies in the fact that the main supply of coagulation factors and blood platelets is usually spent on the formation of clots inside the vessels. Therefore, the risk of severe bleeding, which is very difficult to stop, increases. The development of DIC syndrome can be caused by various pathologies in which the fluidity of blood and its movement in the capillaries are disrupted.
According to clinical manifestations, the disease can have a latent, protracted course, and also manifest itself with lightning-fast reactions leading to death. Damage to internal organs can be local and minor, or widespread blood coagulation occurs in all small vessels with an extremely severe course.
We recommend reading the article about Raynaud's syndrome. From it you will learn about the causes of the development of Raynaud's symptom, stages, methods of diagnosis and treatment of Raynaud's syndrome.
And here is more information about the drug Warfarin.
Causes of occurrence in adults and children
DIC syndrome is provoked by conditions in which there is destruction of the inner layer of blood vessels, blood cells, and tissue damage. This causes activation of blood clotting, disruption of blood flow in small capillaries, venules and arterioles. The reasons for this condition may be:
- infections of a viral or bacterial nature, complicated by sepsis;
- state of shock;
- toxicosis of the second half of pregnancy (preeclampsia);
- previous placental abruption;
- fetal death;
- uterine atony with profuse bleeding;
- C-section;
- metastases in malignant neoplasms;
- amniotic fluid embolism;
- prolonged compression of the limbs;
- major trauma, burns or surgery, especially under artificial circulation;
- atherosclerotic vascular lesions;
- blood transfusion, organ transplantation;
- bleeding;
- installation of prosthetic blood vessels or heart valves;
- abortions, childbirth;
- long-term presence of the catheter in the vessel;
- intravascular destruction of red blood cells during poisoning with hemolytic poisons (lead, mercury, acetic acid, snake bite);
- leukemia;
- radiation sickness;
- intensive antitumor therapy.
Forms of manifestation
Based on the rate of increase in microcirculation disorders and their complications, DIC syndrome is divided into acute, subacute and chronic.
Spicy
Occurs in patients with massive intake of substances into the blood that increase the formation of blood clots. It happens in severe, critical conditions (polytrauma, difficult childbirth, surgery, tissue compression). A feature of this form is the rapid change of phases of the disease, the absence of protective reactions of the body that prevent massive coagulation.
Subacute
It takes weeks (up to 1 month) to develop. The course is more favorable than that of the acute form, the insufficiency of the function of internal organs is less pronounced or moderate, bleeding is weak or moderate. Diagnosed with tumors of the blood, lungs, kidneys, rejection of transplanted tissues, and the use of hormonal contraceptives.
If they are accompanied by blood loss, blood transfusion, administration of hemostatic agents, stress, then it can develop into an acute process.
Chronic
Lasts several months. Organ dysfunction develops slowly and is usually characterized by chewed lesions. It is caused by chronic inflammation of the lungs, liver, tumors, autoimmune diseases, leukemia, and widespread atherosclerosis. To identify clinical signs, as a rule, it is not enough. It is necessary to confirm DIC syndrome with laboratory diagnostics.
Classification
Several types of the disease are known. Clinical variants of the course may manifest themselves depending on:
- prevalence of damage - limited (one organ) and generalized (several systems or the whole body);
- degrees of compensation - compensated (there are no symptoms, blood clots are destroyed by activation of fibrinolysis, coagulation factors are synthesized or released from reserves), subcompensated (there are moderate bleedings), decompensated (a cascade of reactions of resorption of blood clots is triggered, coagulation is impaired, severe bleeding).
Stages of progression
The peculiarity of the disease is the sequential change of symptoms. In the classic version, DIC syndrome has the following stages of progression:
- Increased blood clotting and cell connection. Caused by the release of thromboplastin from destroyed tissues or substances similar to it. They activate thrombus formation processes. Lasts from ten minutes to several months.
- Coagulation disorder due to a lack of fibrinogen, platelets, coagulation factors, since they were intensively consumed in the first phase, and new ones have not yet been formed.
- Critical phase of low clotting capacity. There is no fibrinogen in the blood, red blood cells are destroyed, and coagulation properties may be completely absent.
- Recovery or development of complications. There are either residual signs of dystrophy and destruction, followed by recovery, or acute organ failure increases.
Symptoms of blood clotting pathology
Clinical manifestations of thrombohemorrhagic syndrome consist of signs of the underlying disease, of which it is a complication, and the symptom complex of DIC syndrome.
State of shock
Associated with blood clotting, stopping microcirculation, oxygen starvation of tissues. During the formation of blood clots and their destruction, many toxic compounds enter the bloodstream, leading to disruption of systemic circulation. Most often, it is difficult to determine which changes arose due to microthrombosis and which were its cause. Manifestations of shock include:
- a sharp drop in blood pressure and a decrease in central venous pressure;
- acute microcirculation disorders;
- low functional activity of internal organs.
Complications may include renal, hepatic, respiratory failure, or combinations thereof. DIC against the background of shock always has a severe course, and over a long period - catastrophic .
In the first phase, excessive blood clotting is obvious, it can even be visual when a blood clot forms even before the analysis, immediately after collecting the material. In the second phase, against the background of excessive coagulation, insufficient coagulation also appears. At this time, some tests show an increased, and others a sharply reduced, ability to form blood clots.
Hemorrhagic syndrome
Increased bleeding most often appears during the acute course of the disease. Excessive blood loss can occur against the background of normal or slightly reduced fibrinogen concentrations. Local bleeding can be both a manifestation of DIC syndrome and diseases of the organs themselves (stomach ulcer, kidney infarction, uterine atony). Common signs of hemorrhage are:
- bleeding into the skin, bruises, hematomas;
- nasal, pulmonary, renal blood loss;
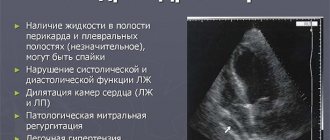
- hemorrhage in brain tissue, adrenal glands, pericardial sac;
- permeation of plasma and red blood cells into the chest and abdominal cavity.
Acute renal failure
Urine production decreases to the point of its absence. Protein and red blood cells are found in the urine. The balance of salts, acids and alkalis in the blood is disturbed, urea, creatinine and residual nitrogen increase. The most severe impairment of kidney function occurs when combined with liver or pulmonary failure, hemolysis of red blood cells.
Target organ damage
The progression of DIC syndrome leads to a generalized disorder - multiple organ failure. Its symptoms:
- destruction of liver cells with jaundice and pain in the right hypochondrium;
- erosions, ulcers and bleeding on the gastric mucosa;
- ulcerative defects in the intestines;
- stopping the movements of the intestinal wall, the penetration of toxins into the blood (weakening of intestinal motility or obstruction;
- blockage of cerebral vessels - dizziness, headache, impaired consciousness, and there may be hemorrhagic strokes;
- pituitary and adrenal insufficiency - severe vascular collapse, diarrhea, dehydration.
Diagnosis of DIC syndrome
To make a diagnosis, the presence of bruises on the skin, bleeding from several organs and the following laboratory signs (based on a blood test) are taken into account:
- destroyed red blood cells;
- decrease in platelets and fibrinogen;
- increase in the level of fibrin destruction products;
- low activity of antithrombin 3;
- prolongation of thrombin time and activated thromboplastin time;
- clots do not form or disintegrate quickly.
In doubtful cases, determination of D-dimer, paracoagulation tests, and soluble fibrin complexes are prescribed.
Treatment of the disease
If there are no clinical manifestations of DIC syndrome, then its laboratory signs are corrected by influencing the underlying condition. In the acute course of the disease, it is necessary to urgently eliminate the cause of its appearance, including surgically. For drug therapy the following is used:
- anticoagulants (Heparin, Clexane);
- antiplatelet agents (Curantil, Pentilin);
- transfusion of frozen plasma, platelets or red blood cells, cryoprecipitate.
Plasmapheresis
In case of severe bleeding, Contrical and aminocaproic acid are administered, and a hemostatic sponge is applied topically. In addition to this, oxygen therapy, plasmapheresis, corticosteroid hormones, angioprotectors, hemodialysis for renal failure, and anti-shock measures are recommended.
Prognosis for patients
The severity of the patient's condition is determined by underlying diseases, the degree of blood clotting disorders and the time of initiation of therapy.
In the first and second phases of the process there are chances of recovery, in the third they are doubtful, and then they are unfavorable. In the acute course, death is associated with shock, blood loss, respiratory and renal failure.
Watch the video about DIC syndrome:
Prevention
It is possible to prevent the development of DIC syndrome only by eliminating the severe pathologies against which it occurs. For this use:
- adequate treatment of underlying diseases;
- less traumatic surgical interventions;
- early elimination of signs of shock;
- for patients at risk of thrombosis (elderly, pregnant women, with diabetes mellitus, tumors), hormonal therapy for contraception, aminocaproic acid is not recommended;
- if blood loss is less than a liter, then albumin, plasma and plasma substitutes are administered, but not whole blood;
- For infections and purulent inflammations, antibiotics are supplemented with agents with an anticoagulant effect.
We recommend reading the article about sympathoadrenaline crisis. From it you will learn about the causes of the crisis, characteristic symptoms and signs, as well as the treatment of sympathoadrenaline crisis.
Read more about drug treatment for stroke here.
DIC syndrome occurs in emergency conditions and requires urgent identification. The acute form is especially dangerous, accompanied by massive thrombus formation.
After the first phase of hypercoagulation, patients experience a high consumption of coagulation factors and increased bleeding. If treatment is not started, the outcome may be shock, blood loss and poor outcome.
For treatment, complex drug therapy is prescribed.
Source: https://CardioBook.ru/dvs-sindrom/
Phases and stages of intravascular changes
DIC syndrome is characterized by the creation of “vicious circle” conditions:
- on the one hand, everything is available in excess for hypercoagulation;
- on the other hand, control over the balance of the synthesis of anticoagulant factors is lost; antithrombin reserves are not enough to counteract the powerful coagulation system.
A modern approach to the prevention and treatment of DIC requires knowledge of the phase of the pathology.
I - maximum hypercoagulation, lasting from several minutes (with a fulminant form) to months (with a latent course associated with chronic heart and kidney failure). Coagulation becomes uncontrollable, microthrombi “clog” all vessels.
II - hypocoagulation, caused by depletion of coagulation factors and a sharp activation of fibrinolysis. In the capillaries, there is a separation of sticky platelets and plasma (sludge phenomenon), and the patient develops a clinical picture of hemorrhagic shock.
III - activation of local fibrinolysis, loose blood clots are half destroyed, fibrinolysin and platelets are consumed.
IV - phase of generalized fibrinolysis, the blood in the capillaries stops clotting, bleeding affects the parenchymal organs, a small petechial rash forms on the skin, the same changes are found in the kidneys, liver, intestines, blood appears in the urine, “black” loose stools, plasma effusion occurs in the cavities. The stage is considered terminal, recovery is impossible.
Different authors classify the stages of DIC syndrome in their own way, although there are few differences in the essence of the changes occurring in them; they correspond to the phases of the pathological process
- Stage I is called hypercoagulable, it does not cause controversy among anyone;
- Stage II is called hypocoagulation and consumption coagulopathy;
- Stage III is associated with a decrease in all possible procoagulants in the blood to complete absence, one of the names is “generalized activation of fibrinolysis”;
- Some scientists consider stage IV to be restorative, apparently as applied to cases of cure, while others are more pessimistic and call it “complete non-coagulation” and “terminal”.
What causes such a complex pathology?
The causes of DIC are determined by the degree of influence of a combination of individual factors in various diseases affecting the blood coagulation system.
Depending on the leading etiological factor, DIC syndrome has a connection with the type of pathology and is identified in various specialized areas of medicine.
The main place belongs to the role of infection. Highlight:
- infectious lesion (DIC syndrome in children with bacterial and viral diseases);
- septic (in the practice of gynecologists as a complication of abortion).
Traumatic injuries cause tissue destruction when:
- long-term compression syndrome (a person is under a rubble);
- burns;
- frostbite;
- massive combined fractures with tissue crushing;
- long-term traumatic operations;
- transfusion of incompatible blood.
In hematology and oncology, DIC syndrome is associated with:
- the need for frequent blood transfusion therapy (except for injuries, complicates blood diseases), especially when using canned drugs;
- radiation sickness;
- hemoblastoses;
- chemotherapy with cytostatics.
In the practice of a therapist and surgeon, DIC syndrome develops against the background of:
- acute toxic liver dystrophy due to poisoning with household and industrial poisons;
- severe pancreatitis with necrosis of pancreatic tissue;
- widespread myocardial infarction;
- organ rejection after transplantation;
- consequences of treatment with Ristomycin, hormones, administration of Adrenaline;
- the use of cleansing plasmapheresis for renal failure;
- systemic lupus erythematosus and vasculitis.
DIC syndrome in obstetrics and gynecology is caused by:
- amniotic fluid embolism;
- early abruption and placenta previa;
- uterine atony and massage;
- intrauterine death and decay of fetal tissue;
- eclampsia in pregnant women.
Pregnancy itself is at risk for DIC syndrome
Any state of shock in the absence or unsuccessful assistance turns into DIC syndrome with a fatal outcome.
The syndrome is expected after heart surgery using a heart-lung machine as a reaction to contact with installed prosthetic parts of blood vessels and heart valves.
Clinicians attach importance to the participation of disseminated intravascular coagulation in the process of microcirculation disturbance without connection with the vessel wall. A similar type of DIC syndrome occurs when:
- increase in protein content in the blood (myeloma);
- inflammatory processes accompanied by hyperfibrinogenemia;
- an increase in the content of red blood cells (cor pulmonale, blood thickening during diuretic therapy, erythremia).
Varieties
There is a classification of the disease depending on the stage of its progression:
- hypercoagulation – increased ability of blood to clot;
- transitional – the simultaneous presence of blood clots and extensive bleeding in the patient;
- hypocoagulation – reduced coagulation;
- outcome stage. There are several options for ending the disease - death or recovery.
In some situations, phases may reappear.
According to the clinical course, this disorder is divided into:
- acute DIC syndrome – characterized by lightning-fast development of the disease. Time ranges from several hours to days;
- subacute – development occurs over the course of a week;
- chronic disseminated intravascular coagulation syndrome – a protracted course that can last for months or years;
- wavy - periods of increased hemorrhage alternate with periods of blood clot formation.
In addition, the syndrome can be localized - affecting only one organ, or local - several organs and systems, or the entire body, are exposed to the pathological process. Any changes in blood clotting can be detected using a coagulogram.
Features of DIC syndrome in newborns
Older children are susceptible to the same pathological factors as adults. But the development of disseminated intravascular coagulation in newborns is determined by their physiological characteristics. They most often have a lightning-fast form of flow. It is impossible to apply any treatment in such cases.
We recommend reading the article: Causes of low platelets in the blood
DIC syndrome accounts for up to half of the deaths of children immediately after birth. The development of pathology occurs in the fetus due to:
- violation of the integrity of the placenta;
- death of one of the twins during multiple pregnancy;
- intrauterine infection;
- preeclampsia and eclampsia;
- uterine ruptures;
- hydatidiform mole.
Premature babies most often suffer from DIC syndrome. Their general hypoxia contributes to:
- underdevelopment of the system for removing waste from the body;
- inadequate supply of blood vessels;
- disruption of the synthesis of coagulation factors and proteolytic enzymes in the liver.
Due to the low content of procoagulants and anticoagulants, such children are prone to increased bleeding and thrombosis in the first hours of life.
Symptoms
The clinical picture of the condition is determined by the current stage of the pathology. The primary signs can be:
- Hypercoagulation stage. The symptoms of the leading disease become the main ones. Signs of impaired blood microcirculation are added - the appearance of a characteristic “marble” mesh on the skin, a decrease in body temperature, blue discoloration of the tips of the fingers and toes, an increase in the volume of the liver/spleen. The development of tachycardia, a drop in blood pressure, and a decrease in urination cannot be ruled out.
- Stage of thrombocytopathy and coagulopathy. Petechiae form on the surface of the skin, the surface of the mucous membranes becomes pale. Bleeding develops in the area where medications are injected. Vital organs - lungs, kidneys, brain - are involved in the pathological process. Internal hemorrhages cannot be ruled out.
- Recovery stage. In the case of treatment adequate to the condition, a decrease in pathological symptoms is observed. The affected organs are restored and begin to function normally.
Read also Why the bleeding does not stop after tooth extraction
Features of DIC syndrome in newborns
DIC syndrome in an infant can develop due to many diseases. The condition typically has a lightning-fast course, which practically excludes the possibility of using any treatment.
Clinical picture
Symptoms of DIC syndrome in terms of severity depend on the form of the course. There are options:
- acute - occurs for all the reasons already listed;
- chronic - accompanies chronic infectious diseases (hepatitis, tuberculosis, AIDS), complicates protracted septic endocarditis, immune pathology, tumors, rheumatism.
Some authors distinguish a subacute course of the syndrome in protracted diseases.
An increased tendency to thrombus formation is determined by the symptoms of parietal and valvular thrombi (rheumatic defects), and the increased incidence of vascular embolization.
In practice, when trying to take blood from a vein, they often find rapid thrombosis inside the needle, a clot in the test tube.
A characteristic combination of petechiae and hematomas
Bleeding manifests itself as:
- bruises on the skin at the slightest injury, from compression with a tourniquet;
- petechial rash;
- hematomas at injection sites;
- nosebleeds;
- bloody black stool;
- increased bleeding of gums.
Heavy uterine bleeding is caused by DIC syndrome during pregnancy and childbirth.
Thrombosis in small vessels disrupts microcirculation in tissues and contributes to organ ischemia. A function failure results in the following picture:
- “shock” kidney with acute failure;
- stroke with changes in consciousness, focal symptoms and paralysis;
- liver failure;
- severe shortness of breath and chest pain due to infarctions in the lung tissue.
The skin and muscle tissue are less sensitive to impaired microcirculation. Insufficient blood supply manifests itself:
- marbled skin look;
- bedsores at pressure points;
- areas of dystrophy are determined in the myocardium.
Etiology
The frequency of DIC syndrome in different types of pathology is heterogeneous: in some diseases and influences it occurs without fail and is an integral part of the pathological process, in others it occurs more or less often. Knowledge of the situations in which DIC occurs is necessary for its prediction, early diagnosis, prevention and treatment.
Most often, the occurrence of DIC is caused by the following pathological processes and effects:
- Causes of DIC syndrome
- infections, especially generalized ones, and septic conditions
- all types of shock: anaphylactic, septic, traumatic, cardiogenic, burn, hemorrhagic and others
- acute intravascular hemolysis during transfusions of incompatible blood, crises of hemolytic anemia, poisoning with certain hemolytic poisons
- tumors, especially disseminated forms of cancer, acute leukemia, blast crises of chronic leukemia, thrombocytosis, paraproteinemic hemoblastoses
- traumatic surgical interventions. The risk of developing disseminated intravascular coagulation increases with the increase in the volume and traumatic nature of the operation, when the latter is combined with other “dangerous disseminated intravascular coagulation” factors (the presence of a malignant tumor, cardiovascular pathology, etc.)
- obstetric and gynecological pathology: premature detachment, placenta previa and rupture, atonic uterine bleeding, manual examination and massage of the uterus, antenatal fetal death, stimulation of labor and fetal-destroying operations, cesarean section, hydatidiform mole, criminal abortion, severe late toxicosis of pregnancy, eclampsia
- injuries; fractures of tubular bones, burns, frostbite, electrical trauma, long-term compression syndrome and others
- transplantation of organs and tissues, vascular and valve prosthetics, the use of devices in which contact with blood is carried out and its subsequent return to the body
- acute and subacute inflammatory-necrotic and destructive processes in the lungs, liver, pancreas, kidneys and other organs
- cardiovascular pathology: congenital “blue” defects, large-focal myocardial infarction, congestive heart failure, progressive atherosclerosis, giant angiomas, pulmonary embolism
- immune and immunocomplex diseases: SLE, Henoch-Schönlein hemorrhagic vasculitis, acute diffuse glomerulonephritis, rheumatoid arthritis with visceral lesions
- severe allergic reactions of drug origin
- thrombotic thrombocytopenic purpura (Moshkovich's disease)
- massive blood transfusions and blood reinfusions
- poisoning with hemocoagulating snake venoms
- syndrome of increased blood viscosity with polyglobules of various origins
- Iatrogenic medicinal forms during treatment with drugs that cause platelet aggregation, provoke blood clotting and reduce its anticoagulant and fibrinolytic potential
Relationship between clinical manifestations and the stage of the process
Based on clinical manifestations, it is possible to assume the stage of a bleeding disorder.
- The first stage is characterized by the predominance of symptoms of the underlying disease, the appearance of hemorrhagic rashes on the skin, and signs of incipient general thrombus formation.
- In the second stage, bleeding and impaired functions of internal organs come to the fore.
- With the development of the third stage, a clinic of failure of several organs at once (multiple organ) joins. The patient has acute vascular, cardiac, respiratory, renal and liver failure, and intestinal paresis. Metabolism changes towards hyperkalemia and decreased protein content. Hemorrhages in the brain, lungs, kidneys, and mesentery are possible.
Further, if the outcome is favorable, the coagulation system is restored. If vital functions are significantly impaired, then it is impossible to correct the situation, the outcome is fatal.
Diagnostics
Diagnosis of DIC requires a thorough history to identify the underlying cause of the disease. Most often, doctors are aware of the possibility, but there are cases when there is no time to wait for test results and it is necessary to urgently begin treatment.
Such a diagnosis of DIC syndrome is called “situational”, and the doctor should focus only on clinical signs and the exclusion of other causes of thrombosis and hemorrhage.
The type of bleeding is distinguished by the combined manifestation of a petechial rash and hematomas. Small hemorrhages are formed when pinching, at the site of the removed tonometer cuff or tourniquet.
Hemorrhages above the right knee occurred after applying a tourniquet in this place and are associated with local hypocoagulation
In the differential diagnosis of DIC syndrome, hemophilia should be excluded - an adult man most often knows about his illness, a newborn boy has subperiosteal hematomas on the skull, the blood does not clot after ligation of the umbilical cord and bleeding continues. Special tests confirm the diagnosis.
Laboratory testing determines the state of hyper- or hypocoagulation of the blood. To do this, study the level:
- platelets,
- antithrombin III,
- plasminogen.
Treatment
Treatment of DIC depends on measures taken to treat the underlying disease. For example, without high doses of antibiotics it is impossible to eliminate the manifestations of the syndrome in sepsis. Taking into account changes in the coagulation process and in organs, drugs with anti-directional action are prescribed.
Emergency care consists of anti-shock measures: the administration of glucocorticoids, for pain, narcotic analgesics will be needed, and Dopamine to support blood pressure.
In the first 40 minutes, at least 1 liter of plasma must be administered
Heparin is able to break the resulting vicious circle in the pathology of DIC, but it requires the presence of antithrombin. Therefore, Heparin injections are used in treatment along with fresh frozen plasma transfusion. It compensates for the lack of antithrombin III and plasminogen.
Heparin is injected subcutaneously into the abdomen, and plasma is injected intravenously.
Trental and Curantil are advisable to use in cases of confirmed hypercoagulation, but maintaining normal platelet levels (or a slight decrease).
In this pathology, hemorrhagic phenomena are not a contraindication for the use of Heparin and antiplatelet drugs.
Plasmapheresis aims to remove fibrin breakdown products and relieve microcirculation disorders. During one procedure, up to 2 liters of plasma are removed. It is replaced by a simultaneous infusion of saline, albumin, and fresh frozen donor plasma.
In case of hypocoagulation, Contrikal is prescribed instead of Heparin. If the patient has no urine output, hyperkalemia, and edema appear, then one should think about acute renal failure. In such cases, urgent hemodialysis is indicated.
Renal and liver failure can be compensated by a combination of plasmapheresis and repeated plasma transfusions. Blood transfusion is carried out only against the background of a sharp decrease in hemoglobin levels (2 times).
Nicotinic acid is used to activate fibrinolysis
If treatment of DIC syndrome is started in the first or second stage and is carried out adequately, then the prognosis for recovery is favorable. In more severe stages, death is almost inevitable.
Complications and prognosis
Among the complications caused by DIC syndrome, it is worth highlighting.
- Impaired blood microcirculation up to the development of complete/partial blockade. Lung and kidney tissues are most often affected. As a result of thrombosis of small vessels of the brain, the development of ischemic stroke cannot be ruled out.
- Hemocoagulative shock. One of the most severe complications of the pathology. Has a bad prognosis.
- Hemorrhagic syndrome. Characterized by hemorrhages, different types of bleeding.
- Posthemorrhagic decrease in hemoglobin level. Anemia develops due to blood loss.
Read also: HELLP syndrome in obstetrics
The prognosis of the syndrome is variable and depends on several factors:
- leading disease;
- severity of hemostasis disorders;
- time of therapy started.
Acute DIC syndrome can lead to the death of the patient due to significant blood loss, the development of shock, disruption of the respiratory system and numerous internal hemorrhages.
Who needs prevention?
Elderly people suffering from combined diseases (atherosclerosis + diabetes mellitus + hypertension + kidney disease) are at increased risk of developing DIC syndrome. They often already have impaired intravascular coagulation, but it occurs latently.
Patients with detected erythrocytosis and decreased antithrombin III should take anticoagulants on a continuous basis. It is especially important to prevent disruption of the coagulation balance during pregnancy and before the necessary surgical intervention.
In their lecture propaganda, doctors should take into account the lack of knowledge of the population on the characteristics of DIC syndrome.
Causes
There are many causes of DIC.
Labor accompanied by complications:
- placental abruption;
- premature birth;
- stillbirth;
- amniotic fluid embolism.
The mechanism of development of DIC syndrome is due to contact of placental tissue with a provoking tissue factor. Against the background of exposure to gram-negative microorganisms, an infectious process occurs.
Formation of tumors - mucinous adenocarcinoma in the pancreas, prostate adenocarcinoma, acute promyelocytic leukemia. In these cases, DIC is caused by the release of tissue factor by malignant cells.
Traumatic brain injury , burn, frostbite, history of a gunshot wound.
Complications of surgical treatment of the prostate gland.
Poisonous snake bite . Enzymes contained in creeping saliva penetrate into the blood, activating blood clotting factors.
Formation of an aneurysm in the aorta or cavernous hemangioma, which damages the vascular walls.
Slowly progressive and latent forms of DIC syndrome are more often found against the background of a tumor process, the presence of an aneurysm or cavernous hemangioma.