Aortic insufficiency is a pathology in which the aortic valve leaflets do not close completely, as a result of which the return flow of blood into the left ventricle of the heart from the aorta is disrupted.
This disease causes many unpleasant symptoms - chest pain, dizziness, shortness of breath, irregular heartbeat and more.
Description of the disease
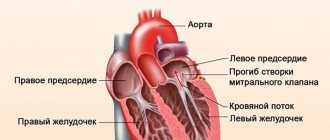
The aortic valve is a valve in the aorta, which consists of 3 leaflets. Designed to separate the aorta and left ventricle. In a normal state, when blood flows from this ventricle into the aortic cavity, the valve closes tightly, creating pressure, which ensures the flow of blood through the thin arteries to all organs of the body, without the possibility of reverse outflow .
If the structure of this valve is damaged, it closes only partially, which leads to the backflow of blood into the left ventricle. In this case, the organs no longer receive the necessary amount of blood for normal functioning, and the heart has to contract more intensely to compensate for the lack of blood.
As a result of these processes, aortic insufficiency is formed.
According to statistics, this aortic valve insufficiency is observed in approximately 15% of people with any heart defects and often accompanies diseases such as mitral valve stenosis and insufficiency. As an independent disease, this pathology occurs in 5% of patients with heart defects. Most often it affects males, as a result of exposure to internal or external factors.
Useful video about aortic valve insufficiency:
Reasons for the development of the disorder
Knowing about the factors causing the problem, you can draw conclusions and partially influence your own destiny in the medical aspect.
So they call it:
- Syphilis, long lasting. Contrary to what you might think, this is not a skin lesion. Against the background of a long course, terminal changes in internal organs occur, up to complete failure. What actually happens to the heart: the cardiac structures are destroyed.
- AIDS. Explains common infectious diseases. They involve the involvement of entire body systems in the process. Without specialized long-term treatment, ensuring a normal or at least acceptable standard of living is impossible. Not only common colds and pneumonia are common, but also myocarditis in different variations. Since the immune system is not active enough, recovery is unlikely. But destruction of the atria with a sudden stop in the activity of the muscular organ is the most common outcome. In such conditions, death is inevitable, a matter of time. No one will undertake the operation; the patient simply will not endure it due to the body’s lack of resistance to external and even internal factors.
- Atherosclerosis of the aorta. The disease is common and dangerous. In the early stages, stenosis or narrowing of the lumen occurs, but this is an uncommon clinical variant. Deposition of lipid structures on the walls of the vessel is likely. Since this is the largest artery, it is quite clear how such a disease itself can end. When valve insufficiency occurs, the risks become many times higher. There are frequent cases of petrification, the deposition of calcium salts in cholesterol plaques. Usually with a long course of the process or in older people. Young people are not immune either.
- Infectious myocarditis. Partially about them was said. This is an inflammatory process in the muscle layer of the heart. The treatment is antibacterial; if necessary, prosthetics of cardiac structures are performed in advanced cases.
- Rheumatoid arthritis and other autoimmune processes, such as lupus or inflammation of the walls of blood vessels, so-called vasculitis. Despite their great destructive potential, these are very rare causes. They account for up to 5% of the total mass of pathological abnormalities in the valves.
- Rheumatism. A classic disease associated with a high risk of failure. Treatment is difficult because the process has an unknown nature, etiology and is difficult to correct. Medicines are used, and their combinations are selected experimentally; it is not known how the body will react. Meanwhile, time passes. The prognosis is especially unfavorable if the problem is detected late, when the pathology reaches stage 3.
- Long-term arterial hypertension. The option is relatively rare; in such a situation, dysfunction is a tertiary consequence. The immediate precursor is left ventricular hypertrophy and general hemodynamic impairment.
Against the background of long-term pathologies of the described kind, aortic valve insufficiency of the 2nd degree is diagnosed. No, the disease does not skip over the previous period, it is simply difficult to identify it in the early phase.
Causes and risk factors
Aortic insufficiency occurs when the aortic valve is damaged. The reasons that lead to its damage may be the following:
- Congenital defects . Congenital defects of the aortic valve occur during pregnancy if the pregnant woman's body is exposed to harmful factors - for example, a large dose of x-ray radiation, or during long-term infectious diseases. Defects can also form if a close relative has a similar pathology.
- Endocarditis is an infectious disease in which the inner layers of the heart become inflamed.
- Rheumatism is a widespread inflammatory disease that affects many systems and organs, in particular the heart. This reason is the most common. Almost 80% of all patients with aortic insufficiency suffer from rheumatism.
- Aortic dissection is a pathology characterized by a sharp expansion of the inner layer of the aorta with its detachment from the middle layer. This problem appears as a complication of atherosclerosis, or with a sharp increase in pressure. An extremely dangerous condition that threatens aortic rupture and death of the patient.
- Syphilis . Because of this sexually transmitted disease, many organs and systems can be affected. If syphilis is advanced, pathological nodules form in organs, including the aorta, which prevent the normal functioning of the aortic valve.
- Trauma . Aortic regurgitation can occur as a result of trauma to the chest when the aortic valve cusps rupture.
- Atherosclerosis of the aorta . Atherosclerosis develops when large amounts of cholesterol accumulate on the walls of the aorta.
- Elderly age . Over the years, the aortic valve gradually wears out, which often leads to problems with its functioning.
- Arterial hypertension . High blood pressure can cause enlargement of the aorta and left ventricle of the heart.
- Ventricular aneurysm . Often occurs after a heart attack. The walls of the left ventricle bulge, preventing the aortic valve from functioning normally.
Other causes of the disease, which are much less common, can be: connective tissue diseases, rheumatoid arthritis, ankylosing spondylitis, diseases of the immune system, long-term radiation therapy for the formation of tumors in the chest area.
Classification of the disease
Aortic insufficiency is divided into 3 degrees. They differ in the divergence of the valve flaps. At first glance, it looks simple. This:
- Sinuses of Valsalva - they are located behind the aortic sinuses, just behind the valves, which are often called semilunar sinuses. The coronary arteries begin from this place.
- The fibrous ring is highly durable and clearly separates the beginning of the aorta and the left atrium.
- There are three semilunar valves; they continue the endocardial layer of the heart.
The doors are arranged in a circular line. When the valve closes in a healthy person, there is completely no gap between the valves. The degree and severity of aortic valve insufficiency depends on the size of the convergence gap.
First degree
The first degree is characterized by mild symptoms. The discrepancy between the valves is no more than 5 mm. It feels no different from the normal state.
Aortic valve insufficiency of the 1st degree manifests itself with mild symptoms. With regurgitation, the blood volume is no more than 15%. Compensation occurs due to increased impulses of the left ventricle.
Patients may not even notice pathological manifestations. When the disease is in the compensation stage, therapy may not be carried out; preventive actions are limited. Patients are prescribed observation by a cardiologist, as well as regular ultrasound checks.
Second degree
Aortic valve insufficiency, which belongs to the 2nd degree, has symptoms with a more pronounced manifestation, while the divergence of the valves is 5-10 mm. If this process occurs in a child, then the signs are subtle.
If, when aortic insufficiency occurs, the volume of blood returning is 15-30%, then the pathology is classified as a second-degree disease. Symptoms are not severe, but shortness of breath and rapid heartbeat may occur.
To compensate for the defect, the muscles and valve of the left atrium are used. In most cases, patients complain of shortness of breath with light exertion, increased fatigue, strong heartbeat and pain.
During examinations using modern equipment, increased heartbeat is detected, the apical impulse moves slightly downward, and the boundaries of cardiac dullness expand (to the left by 10-20 mm). When using X-ray examination, downward enlargement of the left atrium is visible.
Using auscultation, you can clearly hear murmurs along the sternum on the left side - these are signs of an aortic diastolic murmur. Also, with the second degree of insufficiency, systolic murmur appears. As for the pulse, it is increased and pronounced.
Third degree
The third degree of insufficiency, also called severe, has a discrepancy of more than 10 mm. Patients require serious treatment. More often, surgery is prescribed followed by drug therapy.
When the pathology is at stage 3, the aorta loses more than 50% of the blood. To compensate for the loss, the heart organ increases its rhythm.
Basically, patients often complain of:
- shortness of breath at rest or with minimal exertion;
- pain in the cardiac region;
- increased fatigue;
- constant weakness;
- tachycardia.
Research reveals a strong increase in the size of the borders of cardiac dullness down and to the left. Displacement also occurs in the right direction. As for the apical impulse, it is intensified (spread out).
In patients with the third degree of insufficiency, the epigastric region pulsates. This indicates that the pathology involved the right chambers of the heart.
During the examination, a pronounced systolic, diastolic and Flint murmur appears. They can be heard in the area of the second intercostal space on the right side. They have a distinct character.
Two methods of classification are being considered: by the length of the regurgitant blood stream, that is, returning from the aorta to the left ventricle, and by the amount of returned blood. The second classification is used more often during examinations and conversations with patients, as it is more understandable.
- The disease of the first severity is characterized by a volume of regurgitant blood of no more than 15%. If the disease is at the stage of compensation, then treatment is not prescribed. The patient is prescribed constant monitoring by a cardiologist and regular ultrasound scans.
- Aortic insufficiency with a volume of returned blood from 15 to 30% is called grade 2 and, as a rule, is not accompanied by severe symptoms. At the compensation stage, no treatment is carried out.
- At grade 3, the volume of blood that the aorta does not receive reaches 50%. It is characterized by all the symptoms described above, which excludes physical activity and significantly affects lifestyle. The treatment is therapeutic. Constant monitoring is necessary, since such an increase in the volume of regurgitant blood impairs hemodynamics.
- At grade 4, aortic valve insufficiency exceeds 50%, that is, half of the blood returns to the ventricle. The disease is characterized by severe shortness of breath, tachycardia, and pulmonary edema. Both medical and surgical treatment are undertaken.
To assess the severity of hemodynamic disorders and the body’s compensatory capabilities, a clinical classification is used that distinguishes 5 stages of aortic insufficiency:
- I - stage of full compensation. Initial (auscultatory) signs of aortic insufficiency in the absence of subjective complaints.
- II - stage of hidden heart failure. Characterized by a moderate decrease in exercise tolerance. According to the ECG, signs of hypertrophy and volume overload of the left ventricle are revealed.
- III - stage of subcompensation of aortic insufficiency. Anginal pain and forced limitation of physical activity are typical. ECG and radiographs show left ventricular hypertrophy and signs of secondary coronary insufficiency.
- IV - stage of decompensation of aortic insufficiency. Severe shortness of breath and attacks of cardiac asthma occur at the slightest exertion, and an enlarged liver is detected.
- V - terminal stage of aortic insufficiency. It is characterized by progressive total heart failure, deep degenerative processes in all vital organs.
Types and forms of the disease
Aortic insufficiency is divided into several types and forms. Depending on the period of formation of the pathology, the disease can be:
- congenital - occurs due to poor genetics or the adverse effects of harmful factors on a pregnant woman;
- acquired - appears as a result of various diseases, tumors or injuries.
The acquired form, in turn, is divided into functional and organic.
- functional - formed when the aorta or left ventricle expands;
- organic – occurs due to damage to the valve tissue.
Lifestyle
To improve your quality of life if you have aortic valve regurgitation, your doctor may—in addition to other treatments—may recommend:
- Monitor increases in blood pressure.
Reduces blood pressure, reduces the load on the aortic valve. - Eat less salt.
Reducing your salt intake helps you keep your blood pressure within a normal range, which is very important if you have aortic valve regurgitation. - Visit your dentist regularly.
Follow your care instructions. - Maintain a healthy weight.
Maintain your weight within the range recommended by your doctor. Excess weight puts extra work on your heart. - Exercise.
Perform the exercise as recommended by your doctor. He or she may recommend a program of specific intensity depending on the severity of your aortic valve regurgitation. Exercise alone will not improve your condition, but it can help lower your blood pressure. Exercise also helps maintain overall fitness, which will aid in recovery if you need heart surgery. - Visit your doctor regularly.
Set up a regular schedule for visiting your cardiologist or your primary care physician.
If you are a woman of childbearing age with aortic valve regurgitation, discuss pregnancy and family planning with your doctor because your heart will work harder during pregnancy. How much extra work your heart can do with aortic valve regurgitation depends on the degree of regurgitation and how well your heart contracts. If you become pregnant, you will need care from your cardiologist and obstetrician during pregnancy, labor, and postpartum.
1, 2, 3, 4 and 5 degrees
Depending on the clinical picture of the disease, aortic insufficiency occurs in several stages:
- First stage . It is characterized by the absence of symptoms, a slight enlargement of the heart walls on the left side, with a moderate increase in the size of the left ventricular cavity.
- Second stage . The period of latent decompensation, when pronounced symptoms are not yet observed, but the walls and cavity of the left ventricle are already quite enlarged in size.
- Third stage. The formation of coronary insufficiency, when partial reflux of blood from the aorta back into the ventricle already occurs. Characterized by frequent pain in the heart area.
- Fourth stage. The left ventricle contracts weakly, which leads to congestion in the blood vessels. Symptoms such as shortness of breath, lack of air, swelling of the lungs, heart failure are observed.
- Fifth stage . It is considered the pre-mortem stage, when it is almost impossible to save the patient’s life. The heart contracts very weakly, resulting in blood stagnation in the internal organs.
Hemodynamic disorders in aortic insufficiency
Hemodynamic disorders in aortic regurgitation are determined by the volume of diastolic regurgitation of blood through the valve defect from the aorta back to the left ventricle (LV). In this case, the volume of blood returning to the LV can reach more than half of the cardiac output.
Thus, with aortic insufficiency, the left ventricle fills during diastole both as a result of the flow of blood from the left atrium and as a result of aortic reflux, which is accompanied by an increase in diastolic volume and pressure in the LV cavity. The volume of regurgitation can reach up to 75% of the stroke volume, and the end-diastolic volume of the left ventricle increases to 440 ml (with a norm of 60 to 130 ml).
The expansion of the cavity of the left ventricle helps to stretch the muscle fibers. To expel the increased blood volume, the force of ventricular contraction increases, which, if the myocardium is in satisfactory condition, leads to an increase in systolic output and compensation for altered intracardiac hemodynamics. However, long-term operation of the left ventricle in the hyperfunction mode is invariably accompanied by hypertrophy and then dystrophy of cardiomyocytes: a short period of tonogenic dilatation of the LV with an increase in blood outflow is replaced by a period of myogenic dilatation with an increase in blood inflow. The final result is the formation of mitralization of the defect - relative mitral valve insufficiency, caused by LV dilatation, dysfunction of the papillary muscles and expansion of the fibrous ring of the mitral valve.
In conditions of compensation for aortic insufficiency, the function of the left atrium remains unimpaired. With the development of decompensation, there is an increase in diastolic pressure in the left atrium, which leads to its hyperfunction, and then to hypertrophy and dilatation. Stagnation of blood in the vascular system of the pulmonary circulation is accompanied by an increase in pressure in the pulmonary artery with subsequent hyperfunction and hypertrophy of the right ventricular myocardium. This explains the development of right ventricular failure in aortic disease.
Danger and complications
If treatment is not started in a timely manner, or the disease occurs in an acute form, the pathology can lead to the development of the following complications:
- bacterial endocarditis is a disease in which an inflammatory process develops in the heart valves as a result of the impact of pathogenic microorganisms on the damaged valve structures;
- myocardial infarction;
- pulmonary edema;
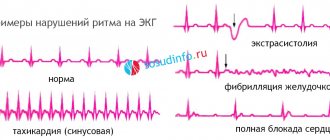
- heart rhythm disturbances - ventricular or atrial extrasystole, atrial fibrillation; ventricular fibrillation;
- thromboembolism – the formation of blood clots in the brain, lungs, intestines and other organs, which can lead to strokes and heart attacks.
When treating aortic insufficiency surgically, there is a risk of developing complications such as implant destruction, blood clots, endocarditis. Surgical patients often have to take medications for life to prevent complications.
Complications
Aortic valve insufficiency—or any heart valve problem—puts you at risk for endocarditis. Endocarditis is an infection of the inner lining of the heart, the endocardium. Typically, this infection affects one of the heart valves, especially if it is already damaged. If the aortic valve is incompetent, it is more susceptible to infection than a healthy valve. You may develop endocarditis when bacteria from another part of your body travels through the bloodstream and travels to your heart.
When aortic valve regurgitation is of moderate severity, it may not pose a serious threat to your health. But when it is severe aortic valve regurgitation, it can lead to heart failure. Heart failure is a serious condition in which your heart is unable to pump enough blood to meet your body's needs.
Symptoms
Symptoms of the disease depend on its stage. In the initial stages, the patient may not experience any discomfort , since only the left ventricle is subjected to stress - a fairly powerful part of the heart that can withstand disruptions in the circulatory system for a very long time.
As the pathology develops, the following symptoms begin to appear:
- Pulsating sensations in the head, neck, increased heartbeat , especially when lying down. These signs arise due to the fact that a larger volume of blood enters the aorta than usual - the blood that returned to the aorta through a loosely closed valve is added to the normal amount.
- Pain in the area of the heart . They can be compressive or squeezing and appear due to impaired blood flow through the arteries.
- Cardiopalmus . It is formed as a result of a lack of blood in the organs, as a result of which the heart is forced to work at an accelerated rhythm to compensate for the required volume of blood.
- Dizziness, fainting, severe headaches, vision problems, ringing in the ears . Characteristic of stages 3 and 4, when blood circulation in the brain is disrupted.
- Weakness in the body, increased fatigue, shortness of breath, heart rhythm disturbances, increased sweating . At the beginning of the disease, these symptoms occur only during physical exertion, later they begin to bother the patient even in a calm state. The appearance of these signs is associated with impaired blood flow to the organs.
The acute form of the disease can lead to overload of the left ventricle and the formation of pulmonary edema, coupled with a sharp decrease in blood pressure. If surgical care is not provided during this period, the patient may die.
Treatment
The therapy is strictly surgical, but few people will undertake to prescribe surgery right away. This is unprofessional; first you need to familiarize yourself with the dynamics of the process.
If there are indications for surgical supervision, the patient is briefly prepared for a difficult intervention.
As a preliminary measure, a reduction in blood pressure, elimination of arrhythmia and restoration of at least minimal myocardial contractility to an acceptable level are indicated.
The following drugs are prescribed:
- ACE inhibitors, beta blockers and calcium antagonists. Diverse in character.
- Antiarrhythmic. Amiodarone is the most common. Also some analogues.
- In the absence of contraindications - cardiac glycosides. But with great caution.
- Antithrombic agents. If there is a violation of blood flow. Aspirin Cardio as the main one, simple acetylsalicylic acid should not be taken, it has a large number of side effects.
- Trace elements and minerals. Magnesium and potassium (Asparkam and the like).
- Acute attacks are relieved with Nitroglycerin.
Traditional recipes are contraindicated. This is a waste of precious time, energy and false hopes for a panacea.
Even surgical treatment does not completely restore the function of the valve, although it allows a long, high-quality life with minor restrictions.
Surgical intervention is aimed at restoring the anatomical integrity of the structure, but this is unlikely.
Mostly prosthetics are used, that is, replacing the septum with an artificial, synthetic one (made from materials that do not provoke rejection).
The technique is risky, but it has no analogues. It is better to start treatment before the development of organic disorders of the heart, since cardiac transformations are already irreversible.
During preparation or during the period of dynamic observation, it makes sense to give up smoking, alcohol, limit salt (no more than 7 grams per day), get full sleep (8 hours per night), eat wisely (less fatty, fried, canned and processed foods, more vitamins and healthy protein). Physical activity is minimal.
Diagnostics
To make a diagnosis, the doctor examines the patient’s complaints, his lifestyle, anamnesis, then the following examinations are carried out:
- Physical examination . Allows you to identify such signs of aortic insufficiency as: pulsation of the arteries, dilated pupils, dilation of the heart to the left side, enlargement of the aorta in its initial section, low blood pressure.
- Urine and blood analysis . With its help, you can determine the presence of concomitant disorders and inflammatory processes in the body.
- Biochemical blood test . Shows the level of cholesterol, protein, sugar, uric acid. Necessary to detect organ damage.
- ECG to determine heart rate and heart size. Find out everything about deciphering the ECG of the heart.
- Echocardiography . Allows you to determine the diameter of the aorta and pathologies in the structure of the aortic valve.
- Radiography . Shows the location, shape and size of the heart.
- Phonocardiogram to study heart murmurs.
- CT, MRI, CCG - to study blood flow.
Diagnostic tests
Common tests to diagnose aortic valve regurgitation include:
- Echocardiogram.
This test uses sound waves to produce an image of your heart. In echocardiography, sound waves are sent to your heart from a wand-like device (transducer) placed on your chest. Sound waves bounce off your heart and are reflected back through your chest wall and processed electronically to provide video images of your heart. An echocardiogram allows your doctor to take a close look at your aortic valve. A certain type of echocardiography, Doppler echocardiography, may be used. This allows measurements of the volume of blood that flows in the opposite direction through the aortic valve. This volume is expressed in cubic centimeters per beat. - Chest X-ray.
Using a chest X-ray, your doctor can examine the shape and size of your heart to determine whether your left ventricle is enlarged, a possible sign of damage to the aortic valve. - Electrocardiogram (ECG).
In this test, wires (electrodes) are attached to your skin to measure electrical impulses from your heart. The pulses are reflected as waves displayed on a monitor or printed on paper. An ECG can provide information about whether the left ventricle is enlarged, a problem that can occur with aortic valve insufficiency. - Transesophageal echocardiography.
This type of echocardiography allows you to take a closer look at your aortic valve. A “sensor tube” is inserted through your esophagus and goes into your stomach and is closer to your heart. In traditional echocardiography, a device called a transducer moves on your chest to produce the sound waves needed to create a picture of your beating heart. In transesophageal echocardiography, a small probe is attached to the end of a tube and passed through the esophagus. This is done to better visualize the image of your aortic valve and the bleeding through it, since the sensor is closer to the valve itself. - Exercises, tests.
Various types of exercise tests to assess activity tolerance and test your heart's response to exercise (sports). - Cardiac catheterization.
Your doctor may order this procedure if noninvasive tests have not provided enough information to firmly diagnose the type and severity of your heart disease. The doctor threads a thin tube (catheter) through a blood vessel in your arm or groin and into your heart. A contrast agent is injected through a catheter in your heart, making details visible on an X-ray. Cardiac catheterization can show if blood is flowing back from the aorta in the heart into the left ventricle. Some catheters are equipped with special sensors that can measure pressure within the chambers of the heart. Pressure may be increased in the left ventricle with aortic valve insufficiency.
ECG
These tests help doctors diagnose aortic valve regurgitation, determine how severe the problem is, and decide whether your aortic valve needs replacement.
Treatment methods
In the initial stages, when the pathology is mild, patients are prescribed regular visits to a cardiologist, an ECG examination and an echocardiogram. A moderate form of aortic insufficiency is treated with medication , the goal of therapy is to reduce the likelihood of damage to the aortic valve and the walls of the left ventricle.
First of all, drugs are prescribed that eliminate the cause of the pathology. For example, if the cause is rheumatism, antibiotics may be indicated. The following are prescribed as additional means:
- diuretics;
- ACE inhibitors – Lisinopril, Elanopril, Captopril;
- beta blockers - Anaprilin, Tranzikor, Atenolol;
- angiotensin receptor blockers - Naviten, Valsartan, Losartan;
- calcium blockers – Nifedipine, Corinfar;
- drugs to eliminate complications resulting from aortic insufficiency.
In severe forms, surgery may be prescribed . There are several types of surgery for aortic insufficiency:
- aortic valve plastic surgery;
- aortic valve replacement;
- implantation;
- Heart transplantation is performed for severe heart damage.
If an aortic valve has been implanted, patients are prescribed lifelong use of anticoagulants - Aspirin, Warfarin . If the valve was replaced with a prosthesis made of biological materials, anticoagulants will need to be taken in short courses (up to 3 months). Plastic surgery does not require taking these medications.
To prevent relapses, antibiotic therapy, strengthening the immune system, and timely treatment of infectious diseases may be prescribed.
Treatments and drugs
Treatment for aortic valve insufficiency depends on how severe the symptoms of the disease are and how the damaged valve affects the functioning of the heart.
Observation
Individuals with mild aortic valve regurgitation do not require treatment. However, even if you do not have signs and symptoms of aortic valve insufficiency, it is worth seeing your doctor regularly. Regular monitoring by a doctor will help to identify the progression of the disease and recommend the correct treatment.
Medicines
Medicines cannot eliminate aortic valve insufficiency. However, there are a number of drugs that help reduce the symptoms of the disease. Control your blood pressure and your weight.
Surgery
As aortic regurgitation progresses, valve replacement surgery may be required. The heart is usually good at fighting problems caused by a leaky aortic valve, the problem is that if the valve is not fixed or replaced in due time, the strength of your heart can decrease so much that it permanently weakens. You can avoid this by having surgery at the appropriate time.
Overall cardiac function and the amount of regurgitation helps determine when surgery is necessary. Surgical procedures include:
- Aortic valve plastic surgery.
Aortic valve repair is performed to preserve the valve and improve its function. Sometimes surgeons can modify the original valve (valvuloplasty) to eliminate the backflow of blood. You will not need long-term drug therapy to prevent blood clots (anticoagulant therapy) after valvuloplasty. - Valve replacement surgery.
In many cases, the aortic valve must be replaced to correct aortic valve regurgitation. Your surgeon removes your aortic valve and replaces it with a mechanical valve or a biologic valve. Mechanical valves, made of metal, are durable, but they carry the risk of blood clots forming on or near the valve. If you have a mechanical aortic valve, you will need to take anticoagulant medications such as warfarin (Coumadin) for life to prevent blood clots. Biological valves, made from pig, cow or human cadaveric donor tissue, often need to be replaced. Sometimes another type of biological valve can be used, which is your own pulmonary artery valve (autograft).
Aortic valve
Traditionally, aortic valve replacement surgery is performed on an open-heart procedure. A less invasive approach is transcatheter aortic valve implantation—installation of a new valve using a catheter through the femoral artery in your leg (transfemoral) or the left ventricle of your heart (transapical). Currently, this procedure is generally limited to those individuals who have aortic valve stenosis or aortic valve regurgitation, and carries a high risk of surgical complications. In the future, transcatheter aortic valve implantation may be an option for the treatment of aortic regurgitation.
Aortic valve insufficiency can be corrected with surgery and you will usually be back to your normal life within a few months. The prognosis after surgery is good.
Forecasts and preventive measures
The prognosis for aortic insufficiency depends on the severity of the disease, as well as on what disease caused the development of the pathology. The survival rate of patients with severe aortic insufficiency without symptoms of decompensation is approximately 5-10 years .
The stage of decompensation does not give such a comforting prognosis - drug therapy is ineffective and most patients, without timely surgical intervention, die within the next 2-3 years.
Measures to prevent this disease are:
- prevention of diseases that cause damage to the aortic valve - rheumatism, endocarditis;
- hardening of the body;
- timely treatment of chronic inflammatory diseases.
Aortic valve insufficiency is an extremely serious disease that should not be left to chance . Folk remedies won't help matters here. Without proper drug treatment and constant monitoring by doctors, the disease can lead to severe complications, including death.
How does valvular insufficiency manifest?
Symptoms of incomplete closure of the aortic valve begin to appear if the reverse flow of ejected blood reaches 15–30% of the volume of the ventricular cavity. Before this, people feel good, even play sports. Patients complain about:
- heartbeat;
- headaches with dizziness;
- moderate shortness of breath;
- feeling of pulsation of blood vessels in the body;
- angina pain in the heart area;
- tendency to faint.
With decompensation of the cardiac adaptation mechanisms, the following appears:
- dyspnea;
- swelling in the limbs;
- heaviness in the hypochondrium on the right (due to stagnation of blood in the liver).
During the examination, the doctor notes:
- pale skin (reflex spasm of peripheral small capillaries);
- pronounced pulsation of the cervical arteries and tongue;
- change in pupil diameter in accordance with the pulse;
- In children and adolescents, the chest protrudes due to strong heartbeats into the non-ossified sternum and ribs.
Intensified beats are felt by the doctor when palpating the heart area. Auscultation reveals a typical systolic murmur.
Blood pressure measurement shows an increase in the upper number and a decrease in the lower one, for example, 160/50 mmHg. Art.
Aortic valve stenosis
Aortic stenosis is a very common pathology: it is found in every 10th person over 65 years of age.
This heart defect is the most common and is observed in almost every tenth patient over 65 years of age. With aortic valve stenosis, a narrowing of the lumen of the aortic mouth is observed, and such a structural disorder leads to the fact that during contraction of the left ventricle, blood does not have time to completely enter the artery. This leads to an increase in the size of the heart, increased pressure in its chambers, fainting and heart failure.
Causes
Aortic valve stenosis can be congenital or acquired.
Congenital aortic stenosis can manifest itself with the following defects:
- there is a cushion of muscle fibers above the aortic valve;
- the valve does not consist of three valves, but of one or two;
- There is a membrane with a hole under the valve.
Such a congenital defect may not make itself felt until 6-10 years of age, but as the child grows, the symptoms of this defect in the development of the heart become more and more pronounced.
Acquired aortic stenosis can be caused by:
- infectious diseases (syphilis, pneumonia, tonsillitis, pharyngitis): such diseases can be complicated by infective endocarditis, accompanied by the appearance of colonies of pathogenic microorganisms on the valve leaflets and the inner lining of the heart; over time, they become covered with a membrane of blood protein and are overgrown with connective tissue, such changes lead to deformities valves and narrowing of the aortic mouth;
- autoimmune diseases (scleroderma, lupus erythematosus, rheumatism): such diseases lead to the proliferation of connective tissue on the valve leaflets, fusion of their pockets and deformation of the aortic mouth;
- age-related changes (atherosclerosis, deposition of calcium salts on the edges of the valve leaflets): such conditions lead to the deposition of calcium salts on the valve leaflets and the growth of fatty plaques on them, which deform it and partially block the lumen of the aortic mouth.
Classification
Normally, the area of the aortic valve opening is 2.5 square meters. cm, and the severity of aortic valve stenosis is determined by its area:
- with a mild degree - about 1.5 square meters. cm;
- with a moderate degree - 1.5-1 sq. cm;
- in severe cases - less than 1 sq. cm.
Depending on the severity of aortic valve stenosis, the severity of its symptoms is determined.
Symptoms
This heart defect is characterized by a long asymptomatic course, and deformation of the aortic mouth, in most cases, is detected during examination for other pathologies or during a preventive examination. Over time, the narrowing of the lumen between the valve and the aorta becomes more pronounced, and the patient has the following complaints:
- shortness of breath after physical activity and when lying down;
- feeling of heaviness in the chest;
- heartache;
- episodes of weakness and dizziness, which can lead to fainting;
- increased fatigue;
- episodes of coughing at night;
- swelling of the lower extremities.
When examining a patient, a doctor may identify the following symptoms:
- pronounced pallor;
- weak pulse filling;
- bradycardia;
- when listening to the heart between contractions of the ventricles, the noise of turbulence of the blood flow in the aortic valve is determined;
- the sound of the aortic valve closing is unclear.
To assess the condition of the heart and make a final diagnosis, the patient is prescribed a comprehensive cardiac examination, which will reveal the degree of deformation of the aortic mouth and the severity of hemodynamic disturbances.
Diagnostics
The patient may be prescribed the following instrumental examination methods:
- ECG;
- radiography;
- transthoracic and transesophageal echocardiography;
- dopplerography;
- cardiac catheterization (not always prescribed).
Drug treatment
If the aortic duct is slightly narrowed, the doctor may prescribe a set of medications that will help improve the enrichment of the heart muscle with oxygen, normalize heart rate and blood pressure.
The complex of drug therapy may include:
- antiangial drugs (Nitrong, Trinitrolong, Sustak): help improve myocardial oxygen saturation, eliminate the feeling of heaviness in the chest and heart pain;
- diuretics (Torasemide, Britomar, Furosemide): prescribed when blood stagnation is detected in the pulmonary vessels to reduce the volume of circulating blood;
- antibiotics (Bicillin-3, Vancomycin): used when necessary to prevent infective endocarditis (during exacerbation of tonsillitis, pyelonephritis, before tooth extraction, abortion, etc.).
The duration of administration, dosing and selection of drugs should be carried out only by a doctor, since even minor violations in dosing can lead to a deterioration in health.
Surgery
Surgical treatment for aortic valve stenosis is indicated when there is a significant deterioration in health, which is expressed in increasing shortness of breath and weakness. Surgeries are prescribed for moderate or severe stenosis, when the lumen area of the aortic valve is less than 1.5 square meters. see. Contraindications to such surgical interventions may include severe concomitant pathologies and the patient’s age over 70 years.
Operation options:
- Aortic balloon valvuloplasty: This minimally invasive operation can be performed in children, patients under 25 years of age, and older patients if there are contraindications to valve replacement or before valve replacement. The only drawback of this surgical technique is the possibility of repeated narrowing of the aortic lumen.
- Valve implantation: this operation is indicated for frequent fainting, significant weakness and increased fatigue, impaired contraction of the left ventricle and significant impairment of the passage of blood through the aortic lumen. This surgical intervention allows you to completely eliminate the manifestations of the disease, significantly improve your well-being and prolong the patient’s life. Artificial valves made of metal and silicone or bioprostheses from one’s own pulmonary artery, taken from the heart of a donor (deceased person) or animal (bull, pig), can be used as prostheses. The recovery period after such an operation can take about 1.5-2 months.
Aortic defects are common heart pathologies that require special attention and timely treatment. Timely prescribed drug therapy or surgery can significantly improve the quality and life expectancy of the patient and prevent the development of many serious complications. Remember this and do not neglect your doctor’s recommendations!
Features of the disease in children
Many children do not notice problems for a long time and do not complain about illness. Most of the time they do well, but it doesn't last long. Many are still able to engage in sports training. But the first thing that torments them is shortness of breath and increased heart rate. If these symptoms occur, it is important to immediately contact a specialist.
At first, unpleasant sensations are noticed with moderate loads. In the future, aortic valve insufficiency occurs even in a calm state. Worried about shortness of breath, strong pulsation of the arteries located in the neck. Treatment must be of high quality and timely.
Symptoms of the disease may appear as murmurs in the area of the largest artery. As for physical development, in children it does not change with insufficiency, but there is a noticeable pallor of the facial skin.
When examining the echocardiogram, aortic valve insufficiency is expressed as a moderate increase in the lumen at the mouth of the artery. There are also noises in the area of the left side of the chest, which indicates the progress of the discrepancy between the lobes of the semilunar valves (more than 10 mm). Strong shocks are explained by the increased work of the left ventricle and atrium in compensation mode.