What it is?
Blasts are immature blood cells that are produced in the bone marrow. They are subsequently converted into red blood cells, white blood cells and platelets. Blast cells are the precursors of mature blood cells.
In a healthy person, blasts in the bone marrow make up no more than 5% of the cells. In infectious diseases, their concentration can increase up to 10%. However, normally immature cells should not enter the bloodstream. They can only be located within the bone marrow.
In severe hematological pathologies, the patient develops blasts in the blood. What does it mean? This analysis result indicates oncological diseases of the hematopoietic system. With these pathologies, an excessive amount of immature elements is formed in the bone marrow. Excess blasts are released into the bloodstream. Their presence in the analysis is an alarming sign.
In the initial stage of blood cancer, the bone marrow may contain about 40% blast cells. Subsequently, a malignant tumor is formed from these immature elements.
Leukocyte formula (with microscopy of a blood smear to detect pathological changes)
Leukocyte formula is the percentage of various forms of leukocytes in the blood serum and the calculation of their number per unit volume. If atypical forms of cells are present, the blood is examined under a microscope.
Unlike red blood cells, the population of which is homogeneous, leukocytes are divided into 5 types, differing in appearance and functions: neutrophils, lymphocytes, monocytes, eosinophils, basophils.
The ratio of different forms of leukocytes in the blood, differentiated leukocyte count, leukocytogram, leukogram, blood formula, leukocyte formula count.
SynonymsEnglish
Leukocyte differential count, Peripheral differential, WBC differential.
*10^9/l (10 in st. 9/l).
What biomaterial can be used for research?
Venous, capillary blood.
How to properly prepare for research?
- Eliminate alcohol from your diet the day before donating blood.
- Do not eat food 2-3 hours before the test (you can drink clean still water).
- Avoid physical and emotional stress and do not smoke 30 minutes before the test.
MORE ABOUT: Anti-wrinkle relief ointment - composition and indications for use
General information about the study
White blood cells, like other blood cells, are produced in the bone marrow. Their main function is to fight infection and respond to tissue damage.
Unlike red blood cells, the population of which is homogeneous, leukocytes are divided into 5 types, differing in appearance and functions: neutrophils, lymphocytes, monocytes, eosinophils, basophils.
White blood cells are formed from stem cells in the bone marrow. They do not live long, so they are constantly renewed. White blood cell production in the bone marrow increases in response to any tissue damage, as part of the normal inflammatory response.
Different types of leukocytes have slightly different functions, but they are capable of coordinated interactions by “communicating” using certain substances - cytokines.
For a long time, the leukocyte formula was calculated manually, but modern analyzers make it possible to carry out the study much more accurately in automatic mode (the doctor looks at 100-200 cells, the analyzer looks at several thousand).
If the analyzer detects atypical forms of cells or detects significant deviations from reference values, then the leukocyte formula is supplemented by a microscopic examination of a blood smear, which makes it possible to diagnose certain diseases, such as, for example, infectious mononucleosis, determine the severity of the infectious process, and describe the type of atypical cells identified in leukemia .
Neutrophils, the most numerous of the white blood cells, are the first to fight infection and are the first to appear at the site of tissue damage. Neutrophils have a nucleus divided into several segments, which is why they are also called segmented neutrophils or polymorphonuclear leukocytes.
At the site of infection, neutrophils surround bacteria and eliminate them by phagocytosis.
Lymphocytes are one of the most important parts of the immune system; they are of great importance in destroying viruses and fighting chronic infection. There are two types of lymphocytes - T and B (the leukocyte formula does not count the types of leukocytes separately).
B-lymphocytes produce antibodies - special proteins that bind to foreign proteins (antigens) found on the surface of viruses, bacteria, fungi, and protozoa.
Surrounded by antibodies, cells containing antigens are accessible to neutrophils and monocytes, which kill them. T lymphocytes are able to destroy infected cells and prevent the spread of infection. They also recognize and destroy cancer cells.
There are not very many monocytes in the body, but they perform an extremely important function. After a short circulation in the bloodstream (20-40 hours), they move into tissues, where they turn into macrophages.
Macrophages are capable of destroying cells, just like neutrophils, and keeping foreign proteins on their surface, to which lymphocytes react. They play a role in maintaining inflammation in some chronic inflammatory diseases such as rheumatoid arthritis.
There are small amounts of eosinophils in the blood; they are also capable of phagocytosis, but they mainly play a different role - they fight parasites, and also take an active part in allergic reactions.
There are also few basophils in the blood. They travel to tissues where they become mast cells. When they are activated, they release histamine, which causes allergy symptoms (itching, burning, redness).
What is the research used for?
- To assess the body's ability to resist infection.
- To determine the severity of allergies, as well as the presence of parasites in the body.
- To identify the adverse effects of certain medications.
- To assess the immune response to viral infections.
- For differential diagnosis of leukemia and to assess the effectiveness of their treatment.
- To monitor the effects of chemotherapy on the body.
When is the study scheduled?
- Together with a general blood test during routine medical examinations and preparation for surgery.
- In case of an infectious disease (or suspicion of it).
- If there is a suspicion of inflammation, an allergic disease or parasite infection.
- When prescribing certain medications.
- For leukemia.
- When monitoring various diseases.
What do the results mean?
The leukocyte formula is usually interpreted depending on the total number of leukocytes. If it deviates from the norm, then focusing on the percentage of cells in the leukocyte formula can lead to erroneous conclusions.
In these situations, the assessment is made based on the absolute number of each type of cell (per liter - 10 12 / l - or microliter - 10 9 / l). An increase or decrease in the number of any cell population is referred to as “neutrophilia” and “neutropenia”, “lymphocytosis” and “lymphopenia”, “monocytosis” and “monocytopenia”, etc.
Blood analysis
How to detect the presence of blasts in the bloodstream? This can be done using a general blood test. This study shows the number of mature and immature cells.
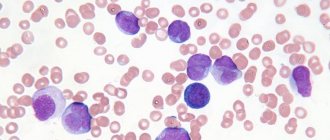
For the sample, blood is taken from a finger or from a vein. The biomaterial is studied under a light microscope. This device has a special grid for counting blood cells. With its help, the concentration of blasts is determined. In the analysis transcript, the number of immature cells is indicated as a percentage.
What is acute leukemia?
Acute leukemia is a consequence of a disruption in the functioning of hematopoiesis in the initial stages. In a normal state, blast cells turn into functional blood cells and fulfill their mission. Each such little body immediately after “birth” has its own line of development. For example: for erythrocytes one type of such cells is “produced”, and for leukocytes – another, and so on.
When the hematopoietic system fails and the creation of healthy base cells is disrupted, the corpuscles behave differently. They do not turn into “working” cells - they only consume useful substances and multiply. Over time, they replace healthy cells and penetrate the bones, destroying them without supplying useful substances. The number of useful cells sharply decreases, hemoglobin, platelets and leukocytes drop.
This disease is lymphoblastic and myeloblastic - depending on what type of cells became the “culprit” of the disease. They are divided into other, smaller categories, depending on the purpose of the damaged blast elements.
Acute lymphoblastic leukemia
They can be designated, for example: acute B-lymphoblastic leukemia, which implies a failure in the creation of blasts at the level of “production” of elements such as B-lymphocytes, or acute monoblastic leukemia, which arose due to problems in the creation of monocytes. Depending on the degree of complexity and type of leukemia, the prognosis for a patient’s cure varies.
Indications for the study
In what cases do doctors prescribe a blast test? This test is indicated if the patient has the following symptoms:
- swollen lymph nodes;
- causeless increase in temperature;
- enlarged liver and spleen;
- weakness;
- severe inflammation of the tonsils;
- red dots on the skin;
- increased bleeding.
Very often, patients mistake these manifestations for signs of tonsillitis and other infectious diseases. However, such symptoms may indicate the presence of severe bone marrow pathology. For the purpose of differential diagnosis, doctors prescribe an analysis for the presence of blasts in the blood.
Prolymphocytic form of chronic lymphocytic leukemia
The prolymphocytic form of chronic lymphocytic leukemia is distinguished primarily by the morphology of lymphocytes, which in bone marrow smears (sometimes in blood), prints and histological preparations of lymph nodes and spleen have a large, clear nucleolus; chromatin condensation in the nucleus, as shown by electron microscopy, is moderate and mainly along the periphery. These cells have no cytochemical features.
Immunological characteristics reveal either the B- or T-cell nature of lymphocytic leukemia, but more often the first. Unlike the B-lymphocytes of typical chronic lymphocytic leukemia, in this form of the disease an abundance of immunoglobulins M or G is found on the surface of leukemic lymphocytes.
Clinical features of this form of lymphocytic leukemia are the rapid development of the process, significant splenomegaly and a slight increase in peripheral lymph nodes.
Apparently, this form of chronic lymphocytic leukemia should be distinguished by a combination of clinical and morphological characteristics, and not only by the characteristics of lymphocytes. There are cases of the disease with the prolymphocytic characteristics of leukemic lymphocytes, but with a tumor form of chronic lymphocytic leukemia, which clinically proceed more favorably than the prolymphocytic form.
Preparing for analysis
A sample for blast cells is usually taken in the morning, on an empty stomach. The analysis results are most often ready the next day.
What rules must be followed before taking biomaterial for blasts? This study does not require complex preparation. You must adhere to the following recommendations:
- stop eating 8 hours before the test;
- do not drink alcohol on the eve of the study;
- Avoid smoking 2 hours before taking blood.
It is also recommended to stop taking medications 3 days before the test. If the patient cannot interrupt the course of drug treatment, then you need to tell the doctor about all the medications you are taking.
Norms of blast cells in a blood test, diagnosis and interpretation of results
Blood test for RFMK transcript
Having received the results of a general analysis, the attending physician will never evaluate only one of its parameters, without paying attention to the others.
To ensure that the balance of the quantitative content of all blood cells in addition to normoblasts is not artificially disrupted, you should adhere to certain preparation rules for several days before diagnosis.
A week before the procedure, you need to inform the specialist about the list of medications you are taking so that he can assess the degree of their effect on the composition of the blood. If certain medications cause undesirable changes, their use may be temporarily suspended. In 3–4 days, harmful foods and drinks are removed from the diet, especially fast food, alcohol, marinades, fatty and fried foods.
It is also necessary to stop sports activities for 1-2 days; running and swimming are no exception. You should visit a medical facility on an empty stomach. Smoking is prohibited before diagnosis. If the patient hastily came to the clinic, he definitely needs to catch his breath before entering the office.
It is not recommended to abuse confectionery products on the eve of blood sampling - exceeding the daily dosage of sweets entails a false test result
Decoding
Normally, blasts should be absent from the analysis. In this case, the study results indicate that their rate is 0%. A healthy person can only have mature elements in their blood.
If even a small percentage of blasts is present in the analysis, then this is a dangerous sign. The test results must be shown to the doctor and treatment must begin immediately.
Is an elevated level always a sign of pathology?
Not at all. For example, normoblasts in a general blood test in absolutely healthy infants up to 3–4 months are a completely acceptable phenomenon associated with the active physiological formation of a small organism. In older children, blastocytes should be observed only in the bone marrow and not in the blood.
Under such circumstances, blast cells will indicate the presence of functional defense mechanisms. Moreover, people sometimes get disappointing results that are overshadowed by repeat diagnostic rates. Therefore, you should not worry when you see alarming numbers on the form; you need to calmly visit a specialist to confirm or refute them.
This study is carried out as a control of treatment, selection and dose adjustment for insulin therapy, to assess the degree of compensation for diabetes mellitus.
Serum fructosamine level (mmol/l):
- norm - 2-2.8;
- satisfactory compensation of diabetes - 2.8-3.2;
- decompensation - more than 3.7.
If glycated hemoglobin is a reliable average of blood sugar over the last 3 months, then fructosamine in the blood is over the last 3 weeks.
Reason for deviation: leukemia
The main reason for the appearance of blast cells in the sample is leukemia. This disease is otherwise called leukemia or blood cancer. The pathology is accompanied by uncontrolled division of immature cells in the bone marrow, which subsequently form a tumor.
Doctors distinguish two forms of leukemia:
- spicy;
- chronic.
In acute leukemia, a huge number of blast cells are found in the blood. Their concentration can be more than 20%. In the chronic form of blood cancer, the rate of immature elements usually does not exceed 5-10%.
Leukolysis
Leukolysis (Greek leukos white lysis destruction, dissolution, disintegration; synonyms leukocytolysis) - dissolution, disintegration, destruction of leukocytes. Leukolysis is caused by a wide variety of agents that can lead to cell death.
With leukolysis, the cell loses its normal structure, its contours become blurry, and often the cytoplasm is completely absent. When lymphocytes are lysed, half-destroyed clumpy nuclei with remnants of nucleoli (nucleoli) are usually preserved.
Leukolysis of neutrophils in most cases leads to the disintegration of the entire cell; sometimes you can see the destruction of the cytoplasm or only part of it without sudden changes in the structure of the nucleus; in other cases, only remnants of the kernel and grain are preserved.
When eosinophils disintegrate, remnants of characteristic granularity are found; when monocytes disintegrate, a reticular structure of the nucleus and a light gray cloud of cytoplasm are revealed.
In the stage preceding complete lysis, leukocytes undergo dystrophic changes. The nuclei become pyknotized or their structure becomes sparse (vague), karyorrhexis, vacuolization of the nucleus and cytoplasm can be observed.
Destroyed cells are detected in blood smears after they are prepared. In normal blood there are single cells destroyed as a result of natural death.
The lifespan of various leukocytes in the human body ranges from several to 100 or more days. Leukolysis in some diseases is obviously associated with changes in the physical, chemical and physiological properties of cell membranes.
Membrane permeability is influenced by lipids, which in the form of phospholipids and cholesterol are part of cell membranes; it is possible that membrane permeability is determined by the ratio of various lipid components.
Leukolysis can occur under the influence of toxic substances of various natures, chemical and physical agents, the action of ionizing radiation, leukocytolytic serum and others.
Lysed cells are found in the blood during typhoid and typhus, during infections, psittacosis, low-symptomatic infectious lymphocytosis, and acute leukemia.
Leukolysis acquires diagnostic significance in chronic lymphocytic leukemia, which is characterized by the so-called Gumprecht's shadow - lymphocyte nuclei destroyed during the preparation of a smear with remnants of nucleoli.
Their number can vary greatly, sometimes accounting for half of all blood leukocytes. However, lysed cells cannot serve as an indicator of the severity of the disease and prognosis.
Leukolysis is observed in the initial period of acute radiation injury. Chronic radiation sickness is accompanied by slight leukolysis
Leukolysis occurs in cases of incomplete phagocytosis, when microbes absorbed by leukocytes are not digested, remain and multiply in the cell.
Lymphadenitis caused by a banal infection may be accompanied by significant Leukolysis. Less commonly, Leukolysis is observed during phagocytosis of gonococci by leukocytes.
Other blood indicators
When studying the results of the analysis, the doctor must pay attention to other indicators of the clinical study. The presence of blast cells in the biomaterial is always considered in combination with other blood parameters. The presence of leukemia may be indicated by the following data:
- Leukocytosis. In approximately 15% of patients with acute leukemia, the white blood cell count is tens of times higher than normal.
- Low hemoglobin. Patients with blood cancer have severe anemia and a decreased number of red blood cells.
- Drop in platelet levels. For this reason, patients with leukemia experience increased bleeding.
- Decrease in reticulocytes. These cells are young forms of red blood cells. Their small quantity leads to anemia.
- Complete absence of eosinophils and basophils. This causes a sharp decrease in immunity.
The above signs, together with the appearance of blast cells in the blood, allow the doctor to diagnose leukemia.
Micromorphology
With leukolysis, the cell loses its normal structure, its contours become blurry, and often the cytoplasm is completely absent. When lymphocytes are lysed, half-destroyed clumpy nuclei with remnants of nucleoli (nucleoli) are usually preserved.
Leukolysis of neutrophils in most cases leads to the disintegration of the entire cell. Sometimes destruction of the cytoplasm or only part of it is observed without sudden changes in the structure of the nucleus; in other cases, only remnants of the kernel and grain are preserved.
When eosinophils disintegrate, remnants of characteristic granularity are found; when monocytes disintegrate, a reticular structure of the nucleus and a light gray cloud of cytoplasm are revealed.
In the stage preceding complete lysis, leukocytes undergo dystrophic changes. The nuclei become pyknotized or their structure becomes sparse (vague), karyorrhexis, vacuolization of the nucleus and cytoplasm can be observed.
Destroyed cells are detected in blood smears after they are prepared. In normal blood there are single cells destroyed as a result of natural death.
The lifespan of various leukocytes in the human body ranges from several to 100 or more days. Leukolysis in some diseases is obviously associated with changes in the physicochemical and physiological properties of cell membranes.
Membrane permeability is influenced by lipids, which in the form of phospholipids and cholesterol are part of cell membranes; it is possible that membrane permeability is determined by the ratio of various lipid components.
Bone marrow examination
If blasts are detected in a patient's blood, doctors usually prescribe a bone marrow puncture. The examination is carried out under local anesthesia. A special long needle is used to make a puncture in the sternum or spine and take a piece of bone marrow tissue for examination.
The punctate is examined using a microscope. The amount of mature and immature blood elements in the biomaterial is determined. An increase in blast cells up to 10% does not always indicate leukemia. This study result is possible in case of severe stress or an infectious disease. If the concentration of blasts exceeds 30%, then this is most often a sign of blood cancer. At the same time, the patient’s number of red blood cells, platelets and leukocytes in the puncture material decreases.
If leukemia is suspected, a cytochemical analysis of the punctate is also performed. It allows you to detect the level of enzymes in blast cells. These substances react with some dyes, which is what is used in laboratory research. Positive test results indicate leukemia. By measuring the level of each blast enzyme, the form of blood cancer can be determined.
Symptoms, course of chronic lymphocytic leukemia
Chronic lymphocytic leukemia usually occurs after age 50 and is twice as common in men. Its clinical picture is extremely diverse, which is explained by the staged course and the presence of various clinical and hematological variants of the disease. As with chronic myeloid leukemia, there are 3 periods of progression:
- I - initial;
- II - period of pronounced clinical and hematological manifestations;
- III - final (dystrophic) period.
MORE ABOUT: Puffiness under the eyes: causes and review of cosmetics
In most cases, the disease is characterized by a gradual onset and a long latent course. Patients are unaware of the existence of the disease for a number of years, despite the presence of characteristic blood changes.
Therefore, the disease is often discovered completely unexpectedly, thanks to a random blood test. In some cases, the initial period is characterized by an increase in certain groups of lymph nodes without subjective disturbances and with full preservation of the patient’s working capacity. In this case, the submandibular and cervical lymph nodes are most often affected.
The duration of the initial period ranges from several months to several years. The second period is characterized by a generalized enlargement of the lymph nodes of the spleen and liver.
General intoxication of the body gradually develops (fever, increased sweating, general weakness, anorexia, itching, etc.), associated with increased destruction of leukocytes and flooding of the body with products of nucleic compounds.
In this period, anemia usually occurs, which increases with exacerbation of the pathological process and is especially pronounced in the third period (final). The cause of anemia is lymphoid metaplasia of the bone marrow with inhibition of erythropoiesis.
Along with this, anemia can be caused by latent hemolysis associated with a shortening of the lifespan of red blood cells (as determined using radioactive chromium), or due to the appearance in the blood of autoantibodies produced by lymphatic tissue (immunohemolytic anemia).
When examining the patient, pallor of the skin and mucous membranes is noted. Sometimes nonspecific rashes appear on the skin in the form of urticaria, erythema and bullous formations resembling pemphigus.
Notice the enlarged lymph nodes in various areas of the body, sometimes reaching the size of a walnut and even a chicken egg. On palpation, the lymph nodes have a doughy consistency, are mobile, not fused to each other or to the skin, and are painless.
The liver and spleen are sometimes enlarged and dense to the touch, but do not reach such large sizes as in chronic myelosis. The same changes are found in the cardiovascular system as in myeloid leukemia (myocardial dystrophy).
Pneumonia is possible, which is often associated with specific lymphoid infiltrates in the lung tissue. The latter develop much more often in chronic lymphocytic leukemia than in myelosis, which is associated with the pronounced development of lymphatic tissue in the lungs.
Lesions of the gastrointestinal tract are very common, which is explained, on the one hand, by the development of specific infiltrates in the mucous and submucous membrane (especially the intestines), rich in lymphatic tissue, and on the other hand, by a violation of the trophism of the intestines due to compression of the veins of the portal system by enlarged lymph nodes.
Damage to the alimentary canal is manifested by dyspeptic symptoms (diarrhea or constipation). Changes in the kidneys are also possible in the form of pyelitis or irritation of the tubular apparatus with the appearance of proteinuria and cylindruria.
In the final stage of the disease, dystrophic changes in internal organs associated with severe hypoxia and intoxication rapidly progress. Violation of tissue trophism leads to the development of necrosis in various parts of the body with the addition of a secondary infection due to inhibition of granulopoiesis (angina, pleurisy, pneumonia, furunculosis, pyoderma, mycotic dermatitis).
A hemorrhagic diathesis appears, in the pathogenesis of which thrombocytopenia, deficiency of a number of blood coagulation factors, as well as impaired permeability of the vascular wall play a role. In the terminal period of the disease, cachexia reaches a high degree.
The blood picture in chronic lymphocytic leukemia is characterized by a significant increase in the number of leukocytes, mainly due to mature lymphocytes, among which there are young forms - pro-lymphocytes and lymphoblasts.
The content of the latter increases with the exacerbation of the process, reaching 50-70%. This disease is especially characterized by a large number of leukolysis cells (Botkin-Gumprecht bodies), which is explained by the low resistance of lymphoblasts.
When assessing the leukogram, the content of granulocytes is of particular importance, a sharp decrease in which indicates the particular severity of the pathological process.
Depending on the number of leukocytes, there are 3 forms of chronic lymphocytic leukemia:
- leukemic,
- subletcemic,
- aleukemic.
With the first, the number of leukocytes is over 50,000 in 1 μl of blood, and sometimes reaches 200,000-300,000 in 1 μl or more. In the subleukemic form, the number of leukocytes ranges from 20,000-40,000 per 1 μl, and in the aleukemic form it is normal or reduced.
Bone marrow puncture reveals hyperplasia of lymphoid elements, the number of which increases sharply as the disease progresses. In the final stage, total lymphoid metaplasia and almost complete disappearance of granulocytes and erythroid elements occur.
Prof. G.I. Burchinsky
“Symptoms and course of chronic lymphocytic leukemia” - an article from the section Diseases of the blood system
Treatment
What to do if a blood test shows the presence of blast cells? In these cases, the doctor usually prescribes a number of additional tests. The most informative of them is a bone marrow puncture. An excessively high number of blasts in the punctate is a sign of leukemia.
If the diagnosis of leukemia is confirmed, then it is necessary to begin treatment immediately. It is important to remember that in the early stages of blood cancer it is quite possible to achieve complete or partial remission. The following methods of treating leukemia are used today:
- Chemotherapy. The patient is prescribed cytostatics that suppress the growth of tumors in the bone marrow. This treatment can take quite a long time.
- Blood transfusion. The patient is given intravenous red blood cells and platelets obtained from a donor. This helps raise hemoglobin levels and reduce bleeding.
- Radiotherapy. This type of treatment is indicated for chronic leukemia. The patient is irradiated with enlarged lymph nodes and the spleen area.
- Antibacterial therapy. Patients with leukemia are very susceptible to infectious pathologies. In order to prevent such diseases, courses of antibiotics are prescribed.
- Bone marrow transplantation. This operation helps to completely get rid of leukemia. The difficulty of transplantation lies in the fact that a foreign hematopoietic organ does not always take root.
After complex therapy, a repeat bone marrow puncture is performed. If the concentration of blasts has decreased to 5%, then doctors talk about complete remission. If the rate of immature cells does not exceed 20%, then remission is considered partial. In any case, the patient must follow the doctor’s recommendations for life. Leukemia is a dangerous and serious disease. Even with complete remission, relapses of the pathology cannot be ruled out.
Blood picture in acute lymphocytic leukemia
In acute lymphocytic leukemia, blood test results differ from the chronic form of the disease. In 10% of patients, the indicators remain normal, which complicates the initial diagnosis of the disease. The remaining 90% experience the following changes:
- leukocytes may be normal, increased or decreased;
- an increased number of lymphocytes displaces other types of leukocytes;
- the presence of immature lymphocytes in the blood, which should not normally be present;
- a decrease in red blood cells and hemoglobin, which indicates anemia;
- decreased platelet count;
- increase in erythrocyte sedimentation rate (ESR).
If there is a decrease in the number of red blood cells and platelets, this indicates late stages of acute lymphocytic leukemia. Anemia and thrombocytopenia appear as a result of the displacement from the red bone marrow of all hematopoietic sprouts except the lymphocytic one.
The lymphocytes themselves do not have time to mature and enter the peripheral blood in the form of lymphoblasts or young immature cells. To determine the leukocyte formula, a blood smear is analyzed.
It is applied to laboratory glass and then painted with special dyes. The analysis is carried out visually under a microscope by counting the number of leukocytes of different types.
Not only their ratio is established, but also the presence of young and blast cells. In acute leukemia, both young cells and mature lymphocytes are present in the blood.
Another indicator that indicates the severity of the disease is the level of LDH, the enzyme lactate dehydrogenase. Normally, in males after 13 years of age it is 11.4 µkat/l, in females – 7.27.
Elevated levels of the enzyme in the blood are a diagnostic marker. LDH increases with organ damage. In particular, isoenzymes (varieties)
LDH-3 and LDH-4 are found in the tissues of the spleen. If malignant lymphocyte cells develop in it, the level of the enzyme increases. The higher its level in the blood, the more severe the disease. To carry out the analysis, blood is taken from a vein.