Metabolism of vitamin B12 in the body
Participation of vitamin B 12 in hematopoiesis
Vitamin B12 (cyanocobalamin) is one of the most important components of bioorganic reactions for the construction of DNA strands, as well as the synthesis and regeneration of myelin in the body.
There are two factors that contribute to the performance of specified functions by cyanocobalamin. The role of the external factor is performed by vitamin B12 itself as a component of food, the internal factor (Casla) is synthesized by the parietal cells of the stomach. Entering the stomach with food proteins, which are cleaved from the vitamin by gastric juice pepsin, the external factor binds to the carrier protein and is transported to the final section of the duodenum. Here both factors meet, form a complex and are absorbed in the final ileum with the participation of receptors on cells of the intestinal mucosa. Once in the blood, cobalamin forms a complex with another transport protein and is delivered to organs and tissues, where it is used in synthesis processes.
Vitamin B12 and folic acid deficiency: what is the danger
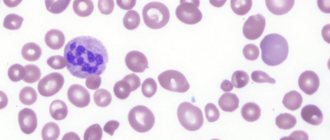
B12-deficiency anemia and its variant, accompanied by a lack of folic acid in the body, are megaloblastic anemias, which lead to disruption of the production of DNA responsible for cell proliferation. With anemia, the cells of the bone marrow, skin, and mucous membranes of the gastrointestinal tract suffer more than others.
The “damaged” cells include hematopoietic cells. They are also called hematopoietic cells. If this process is disrupted, the patient develops anemia. Often, in addition to anemia, which is accompanied by a drop in the level of red blood cells and hemoglobin in the blood, people develop a shortage of other blood cells: platelets, neutrophils, monocytes, reticulocytes.
All disorders of the hematopoietic system are closely related to each other. The explanation for this is as follows:
In order for the body to form active folic acid, vitamin B12 is required.
In turn, folic acid is needed for the production of thymidine, an important component of DNA. If there is not enough vitamin B12 in the body, then the synthesis of thymidine stops, which leads to the formation of defective DNA. It quickly breaks down, and cells of tissues and organs die.
If at least one of the links in this chain is disrupted, then blood cells and cells of the gastrointestinal tract will not be able to form normally.
Vitamin B12 is responsible for the breakdown and production of certain fatty acids. If there is a deficiency in the body, this leads to the accumulation of methylmalonic acid, which is harmful to neutrons. Its excess reduces the production of myelin, which is part of the myelin sheath that covers nerve fibers and is responsible for transmitting impulses through nerve cells.
Folic acid does not affect the breakdown of fatty acids; it is not required to ensure normal functioning of the nervous system. If a person suffering from vitamin B12 deficiency is prescribed folic acid, then for some time it will stimulate the production of red blood cells, but when too much of it accumulates in the body, this effect will end. Excess folic acid will stimulate vitamin B12 to start the process of erythropoiesis. Moreover, even that vitamin B12, which is designed to break down fatty acids, will have to work. Naturally, this will negatively affect the nerve fibers and the spinal cord (the processes of its degeneration will be launched), the functional sensitivity and motor function of the spinal cord will be impaired, and the development of combined sclerosis is possible.
So, a low level of vitamin B12 in the body leads to a disruption in the growth of blood cells and provokes the occurrence of anemia. Also, vitamin B12 deficiency negatively affects the functioning of the nervous system. Folic acid negatively affects the process of hemocytoblast division, but the human nervous system does not suffer.
Differences between B12 deficiency anemia, pernicious anemia and megaloblastic anemia
The term “pernicious” applies to B12 deficiency anemia resulting from autoimmune gastritis. In this case, the “aggression” of the body’s immune system, directed at itself, persists for life, the secretion of Castle factor by gastric glandulocytes is reduced, which impairs the absorption of cobalamin even when it is taken in excess from food. This variant of the disease requires repeated courses of therapy with cobalamin drugs.
Megaloblastic anemia is considered to be anemia in which the ancestor of the “red sprout” in the bone marrow becomes an unusually large abnormal cell. Its diameter is more than 15 microns, it has an unformed core. From the megaloblast a megalocyte is formed - a large erythrocyte with good hemoglobinization of the cytoplasm, but still having an immature nucleus; such an erythrocyte is prone to rapid death.
Diagnostics
When making this diagnosis of B12 deficiency anemia, the doctor first of all during diagnosis collects an anamnesis when and under what circumstances the pronounced symptoms of anemia appeared, with its weakness and manifestations of pathology in the digestive process.
It is also necessary to find out whether the patient has diseases that occur in a chronic stage, as well as to provide information about possible genetic hereditary congenital diseases.
After the medical history, the patient’s skin is examined and pronounced symptoms on the skin are determined.
The doctor also measures the blood pressure index (in anemia, the pressure is low), as well as the heart pulse (often the pulse is rapid).
After this examination, based on external signs, laboratory diagnostics (blood tests) are prescribed, as well as a list of instrumental studies:
- General blood analysis,
- Biochemical analysis of blood composition,
- Urine for general analysis,
- Bone marrow puncture,
- Electrocardiography (ECG),
- Ultrasound of the liver and spleen,
- Ultrasound of the intestines,
- Ultrasound of the stomach.
When deciphering the general analysis, the whole picture of the blood is visible, the indicators of each element in its composition. According to this analysis, in vitamin B12 deficiency anemia, a decrease in red blood cell molecules is seen, as well as a decreased synthesis of reticulocytes.
The level of red pigment (hemoglobin) is reduced, platelets are also reduced, which provokes hypoxia. Color increases with anemia and reaches more than 1.50 (with the norm being 0.860 - 1.050).
During the analysis, the presence of proteins in urine is observed, and possible detection of concomitant pathologies.
Biochemistry is the most valuable analysis for identifying deviations in the structure and composition of the blood.
Biochemistry reveals the following indicators for B12 deficiency anemia:
- The cholesterol index is often elevated in anemia,
- The presence of creatinine
- Glucose in the blood
- Uric acid,
- Electrolyte indicators of calcium, potassium and sodium molecules,
- Lactate dehydrogenase is an enzyme found in liver cells that promotes the absorption of iron by cells. Indicator of biological reactions for the synthesis of red blood cells and hemoglobin,
- B vitamins are reduced. The B12 index is low.
A blood hemogram shows the hematocrit number, the percentage of all types of leukocytes is determined by the leukocyte formula.
A myelogram, or bone marrow puncture indicators, determines the level of production of red blood cell molecules, as well as megaloblasts in the blood, which confirms the megaloblastic nature of hematopoiesis in the human body.
The instrumental technique determines deviations from standard indicators in the structure of internal organs, and also identifies violations in their functionality.
Pathogenesis of B12-deficiency anemia
Metabolism of cyanocobalamin in the body
Cyanocobalamin is a cofactor in important reactions associated with methionine resynthesis and folate regeneration. With a lack of cobalamin or folic acid, uridine is not integrated into the DNA chains of dividing and growing cells, which are the precursors of all hematopoiesis, and thymidine synthesis also suffers. The result of the violations: DNA division into fragments, cell mitosis stops. This is how megaloblasts arise. Large red blood cells, white blood cells and platelets are grouped in the bone marrow. They are characterized by rapid death. A small percentage of cells still enter the circulation and end up in the blood plasma, but have reduced functionality. In severe cases, the patient faces pancytopenia: a total deficiency of all blood cells.
Cobalamin is also a component of the synthesis reaction of succinyl-CoA from methylmalonyl-CoA. This reaction ensures the production of the required amount of myelin to cover each nerve fiber. Myelin is formed from a precursor - the amino acid homocysteine. This reaction to cobalamin deficiency explains the presence, in addition to megaloblastic anemia, of severe demyelinating lesions of the brain and peripheral nerves.
Causes of the disease
Autoimmune gastritis is the cause of pernicious anemia
1) Vitamin deficiency in food. The best sources of vitamin B12 are the liver and kidneys of cattle and pigs. In second place is red meat. Unfortunately, in our time, the frequency of consumption of benign meat products among the population is falling, and strict vegetarianism is also becoming popular. In this case, the internal reserves of cobalamin last for 2-3 years, after which nutritional deficiency of the vitamin threatens the development of anemia.
2) The presence of diseases and conditions that prevent the normal absorption of vitamins in the gastrointestinal tract. In the first place are pathologies that lead to the loss of the ability of the gastric mucosa to form Castle factor, without which the absorption of cobalamin does not occur. For example, autoimmune gastritis, gastrectomy, chronic alcoholism, which causes corrosive changes in the gastric mucosa. “Inertia” of the Castle factor, its low activity, genetically programmed, can also be observed.
In celiac disease, the absorption of cyanocobalamin is impaired
In second place among such diseases are lesions of the small intestine. For example, hereditary cyanocobalamin malabsorption, malabsorption caused by long-term use of certain medications (PPIs, metformin, cholestyramine), celiac disease, massive intestinal resections.
3) The use of cyanocobalamin by “competitors” before it enters the blood, which happens, for example, with dysbacteriosis, diverticular disease of the small intestine, gastroduodenal anastomoses, helminthiasis (the presence of a wide tapeworm in the intestine).
4) Increased needs for vitamins in pregnant women.
Diet for this form of anemia
A balanced diet is especially necessary during the period of intrauterine development of a child, since the formation of the baby, as well as the occurrence of intrauterine pathologies that are revealed after birth, depend on the intake of vitamins in the body of a pregnant woman.
During pregnancy, the need for vitamin B12 increases by 50.0%.
products; amount of B12 in mcg
| · calf liver | · 60,0 |
| liver of a young piglet | · 30,0 |
| chicken liver | · 16,0 |
| · mackerel fish | · 12,0 |
| · rabbit meat | · 4,30 |
| · veal | · 2,60 |
| · perch fish | · 2,40 |
| · pork | · 2,0 |
| · eggs | · 0,40 |
| · fat sour cream |
For B12 deficiency anemia, diet table No. 11 is used. This diet should increase the content of protein and vitamin B12 in the body. The food preparation method is standard. You need to eat 5 times a day.
Energy value of diet No. 11:
- Proteins 110.0 grams 130.0 grams (60.0% animal origin, 40.0% plant origin),
- Fats 100.0 grams 120.0 grams (80.0% animal and only 20.0% vegetable),
- Carbohydrates 400.0 grams 450.0 grams,
- Salt no more than 15.0 grams,
- Purified water 1.5 liters.
products useful for B12 deficiency anemia; prohibited products
| · veal, pork, chicken liver | · milk |
| · salo | · baking |
| · butter | · confectionery sweet products |
| · mackerel fish | · tea |
| · meat: veal, rabbit, pork | caffeinated drinks |
| · eggs | · Coca Cola |
| · fat sour cream | · alcoholic drinks |
| · low-fat cottage cheese | Do not use vinegar in cooking |
| · hard cheese | sweet carbonated drinks |
| · soft cheese | |
| Legumes: peas, lentils | |
| vegetables: carrots, potatoes, cabbage, beets, tomatoes | |
| · fruits of all varieties | |
| · berries of all types | |
| Green vegetables are rich in iron | |
| · garden greens | |
| mineral water |
Symptoms
Heartburn is one of the symptoms of the disease
A typical clinical picture of this type of anemia can be characterized by the following syndromes: circulatory-hypoxic, gastroenterological, neuropsychic.
The first syndrome is a manifestation of general hypoxia of the body, because red blood performs the function of transporting oxygen to tissues and recycling carbon dioxide from them. A person with total hemic hypoxia is characterized by: drowsiness, weakness, high fatigue, dizziness, episodes of depression of consciousness, frequent and heavy breathing, rapid heartbeat, pale skin and mucous membranes with a yellowish tint, the presence of vascular and cardiac murmurs on auscultation.
The second syndrome includes: poor appetite, nausea, aversion to meat foods, heartburn, unstable stools, atrophy of the papillae of the tongue (“lacquered” tongue of a “crimson” color), hepatomegaly, and, infrequently, enlarged spleen.
Disorders within the third syndrome can be explained by “funicular myelosis,” a condition resulting from the gradual demyelination of the spinal cord pathways. First of all, various types of sensitivity suffer (tactile, temperature, pain, vibration), then paresthesia occurs (spontaneous tingling, burning), a little later - muscle strength decreases, normal reflexes increase or pathological ones are “disinhibited”. In the most severe cases, funicular myelosis results in dysfunction of the pelvic organs (with incontinence of urine, gases, feces), paresis, paralysis, organic depression, paranoia, hallucinations, constant insomnia, and psychosis.
Diagnostic criteria
Anemia has its own diagnostic criteria
1. Changes in blood tests: decrease in hemoglobin (less than 130 g/l); macrocytosis (erythrocyte diameter more than 12 microns), rarely the sizes remain normal (8-11 microns); hyperchromia of erythrocytes (CP more than 0.9); anisocytosis (atypical morphology of red blood cells); Jolly bodies, Cabot rings (parts of the oddly shaped nucleus inside cells). Thrombocytopenia and leukopenia cannot be excluded.
2. Change in cobalamin content in blood serum (below 220 pg/ml). Increased plasma homocysteine (more than 16 µmol/l).
3. Biochemical blood test serves mainly to monitor hemolysis. This anemia is characterized by a slight increase in indirect bilirubin, LDH.
Physical examination is important
4. Corresponding complaints and appearance of patients.
5. Reliable identification of the root cause of cobalamin deficiency.
6. Positive effect of treatment with cobalamin: an increase in the level of young red blood cells by more than ten times after a week of therapy.
7. Analysis of bone marrow punctate. This way, it is possible to reliably identify the megaloblastic type of erythropoiesis: large cell sizes, basophilic cytoplasm, and a fine chromatin network of the nucleus in cells in the late stages of maturation.
Forms
According to the degree of severity, depending on the content of hemoglobin (a special substance contained in red blood cells that carries oxygen) in the blood, they are distinguished:
- mild anemia (hemoglobin from 90 to 110 g/l, that is, grams of hemoglobin per 1 liter of blood);
- moderate anemia (hemoglobin from 90 to 70 g/l);
- severe anemia (hemoglobin less than 70 g/l).
Normally, in men, the hemoglobin content in the blood is 130/160 g/l. Situations in which blood hemoglobin is from 110 to 130 g/l are intermediate between normal and anemia.
Treatment
Treatment is carried out according to the cause of the disease
First, you should start by identifying the true cause of this type of anemia and eliminating it. For example, in case of infection with a wide tapeworm, carry out deworming; in case of intestinal dysbiosis, use bacteriophages, symbiotics, and digestive enzymes.
Secondly, nutritional correction is necessary. With many years of strict vegetarianism, changing eating habits is quite difficult, but a preventive conversation with a doctor about the consequences of vitamin B12 deficiency, the main source of which is meat, can increase the patient’s alertness and literacy.
Thirdly, the main therapeutic measure is drug therapy. Cyanocobalamin is administered intramuscularly at a dosage of 200-400 mcg per day once, in severe cases - twice a day. An effective course of injections is considered to be treatment for up to six weeks.
Complications and consequences of the disease
Cyanocobalamin deficiency negatively affects the nervous system
The greatest danger is posed by continuously progressive damage to the nervous system without treatment, which can result in paresis of the lower extremities, disorders of sensitivity and functioning of the pelvic floor organs, and depression of the human psyche.
Simultaneously with the breakdown of red blood cells, leukocytes and platelets can be destroyed. Profound leukopenia can lead to severe infectious complications. Thrombocytopenia will manifest itself as hemorrhagic syndrome (bruising, bleeding gums, severe nasal and uterine bleeding).
Prognosis and prevention
Diet plays an important role in the prevention of anemia
The prognosis is favorable only with timely detection of pathology and treatment of the patient. However, severe chronic diseases (autoimmune gastritis), as well as incurable complications, cast doubt on the prognosis.
To prevent the disease, it is recommended to consume sufficient amounts of dietary vitamin B12. The daily requirement for it is 3 mcg per day, and it is extremely easy to satisfy. For example, 100 g of beef liver contains 70 mcg of this vitamin, 100 g of beef kidneys - 25 mcg, 100 g of rabbit meat - 8 mcg of cyanocobalamin.
For people with chronic pathology and those who cannot change their eating habits, lifelong preventive courses are possible: 200–400 mcg of the vitamin is administered once a month, an alternative to this is courses of 10–14 injections every six months.
Prevention
The diet of a child suffering from B12 deficiency anemia should contain foods rich in this vitamin.
Prevention of anemia in a child should be taken care of even before the baby is born. A pregnant woman should, firstly, eat right and adhere to all recommendations for the regimen, and secondly, regularly monitor blood tests. With the development of anemia in a pregnant woman, the risk of its occurrence in the infant increases significantly.
After birth, the optimal nutrition for the baby is mother's milk. During the lactation period, it is also very important for a nursing mother to ensure proper nutrition. From the age of 6 months, complementary foods should be introduced to the baby, while following all the recommendations of the pediatrician. At 6 and 12 months, the child undergoes a blood test.
Older children should be under the supervision of a pediatrician and have an annual blood test. Children's nutrition should be balanced, providing the child with all the nutrients and vitamins necessary for a growing body. It is important to promptly identify and treat helminthiases and inflammatory diseases of the gastrointestinal tract, which can cause anemia.