General information
Pernicious anemia was first described by Addison in 1855, describing the disease as “idiopathic anemia” (anemia of unknown origin).
A detailed clinical and anatomical description of the disease belongs to Birmer (1868). It was Brimer who gave the disease the name “pernicious anemia”, i.e. pernicious anemia. For a long time the disease was considered incurable, but in 1926 Minot and Murphy made a discovery that pernicious anemia can be cured with raw liver (liver therapy). This discovery and subsequent work by the American hematologist and physiologist W. B. Castle formed the basis of modern ideas about the pathogenesis of this disease.
W. B. Castle established that normally a person produces not only hydrochloric acid and pepsin, but also a third (internal) factor - a complex compound consisting of peptides and mucoids, which is secreted by mukocytes (cells of the gastric mucosa). This compound forms a labile complex with an external factor (vitamin B12), which, after entering the blood plasma, forms a protein-B12-vitamin complex that accumulates in the liver. This complex takes part in hematopoiesis. W. B. Castle revealed the absence of internal factor secretion in the stomach in patients with pernicious anemia, but did not establish the chemical nature of the external factor.
The substance (vitamin B12), which plays the role of an external factor, was established in 1948 by Ricks and Smith.
The disease is quite common - the prevalence rate is 110 -180 patients per 100,000 population. Residents of the UK and the Scandinavian Peninsula are most susceptible to the disease.
In most cases, pernicious anemia affects people who belong to the older age group (observed in 1% of people over 60 years of age). If there is a family predisposition to the disease, the disease is detected at a younger age.
In women, the disease is observed more often (10:7 in ratio to males).
What is the cause of pernicious anemia?
Historical reference
In 1855, Thomas Addison described a fatal idiopathic anemia, which in 1872 was named Addison-Beermer pernicious anemia.
Over the ensuing decades, the generally accepted view was that pernicious anemia was the result of a harmful influence, bacterial or fungal. The popular concept was that the harmful agent caused excessive destruction of red blood cells. Clinical studies subsequently determined that pernicious anemia was more than a red blood cell disorder.
Clinical studies subsequently showed that pernicious anemia is not only associated with a lack of red blood cells.
Two important discoveries were published in the 1920s:
- pathologist George Whipple and his colleague showed that anemia could be the result of nutritional deficiencies;
- two clinical researchers, George Minot and William Murphy, developed a special diet that could reverse the pathology and cure patients.
This was a huge breakthrough because 1-2% of people over 50, primarily of northern European origin, suffered from this deadly disease.
These important discoveries gave rise to other research in the coming decades. In particular, William Castle identified the complex pathophysiological mechanisms underlying this type of anemia. The scientist’s conclusions made it possible to find new, more effective and affordable treatment methods.
Pathogenesis of pernicious anemia
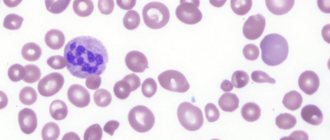
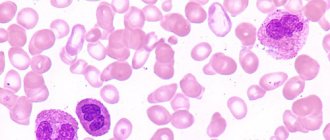
The term "pernicious anemia" is synonymous with megaloblastic anemia. This form of anemia occurs when red blood cells do not mature properly due to a lack of vitamin B12. They become too large and cannot perform their function. Such cells are called megaloblasts.
Currently, the term "pernicious anemia" is used when megaloblastic anemia is caused by vitamin B12 deficiency due to the absence of Castle factor (intrinsic factor - EF).
What is Castle factor?
Vitamin B12 can only be absorbed if it is bound to Castle's factor. The internal cavity of the stomach is lined with a thick mucous membrane. This membrane contains glands that produce gastric juice.
The mucous membrane in the lower part of the stomach contains parietal cells. These cells produce hydrochloric acid and Castle factor. In the initial part of the small intestine (duodenum), B12 binds to VF. This complex travels through the small intestine to its final part, the ileum, where it binds to receptors. There, B12 is transported through the intestinal wall into the blood, bound to transcobalamin, a transport protein that carries the vitamin into tissues and cells, where it is converted into methylcobalamin and adenosylcobalamin.
VF deficiency in PA can be caused by two mechanisms:
- progressive destruction and possible loss of parietal cells, which leads to a decrease in the production of HF;
- the presence of blocking antibodies that prevent the binding of B12 and VF.
Antibodies against VF are found only in the case of PA. The presence of antibodies against parietal cells is prognostic for autoimmune gastritis, which can ultimately lead to anemia.
Antibodies against VF are of the IgG type and are found in 50-70% of people with PA.
The presence of antibodies against VF indicates the presence of PA. However, their absence does not exclude this diagnosis.
Forms
Pernicious anemia, depending on the amount of hemoglobin in the blood of patients, is divided into:
- mild disease, which is diagnosed when hemoglobin is from 90 to 110 g/l;
- moderate anemia, detected when hemoglobin is from 90 to 70 g/l;
- severe anemia, in which the blood contains less than 70 g/l of hemoglobin.
Depending on the cause of the development of B12 deficiency anemia, there are:
- Food or nutritional anemia (develops in young children). It is observed when there is a lack of vitamin B12 in the diet (vegetarians, premature babies and children fed with milk powder or goat milk).
- Classic B12-deficiency anemia associated with atrophy of the gastric mucosa and the absence of “intrinsic” factor.
- Juvenile B12 deficiency anemia, which develops due to the functional insufficiency of the fundic glands that produce glandular mucoprotein. The gastric mucosa and the secretion of hydrochloric acid are preserved. This disease is reversible.
Separately, there is familial B12 deficiency anemia (Olga Imerslund's disease), which is caused by impaired transport and absorption of vitamin B12 in the intestines. In patients with this disease, protein is detected in the urine (proteinuria).
Treatment and prevention of pernicious anemia
The amount of vitamin B12 found in the body is directly related to the amount taken. The main treatment for pernicious anemia is injections of vitamin B12 ( cobalamin ). Determining the amount of vitamin B12 you need can be difficult because it must also replace the vitamin B12 found in the liver.
Reasons for development
Pernicious anemia develops in the body:
- As a result of impaired absorption of vitamin B12, which occurs with atrophic fundic gastritis, partial resection (removal) of the stomach and total gastrectomy, exocrine pancreatic insufficiency, small intestinal dysbiosis, Solinger-Ellison syndrome, diseases of the terminal ileum (Crohn's disease, etc.).
- If there is a violation of the supply of vitamin B12, which is caused by the lack of meat, eggs and dairy products in the diet (vegetarianism, fasting).
- With the competitive absorption of vitamin B12, which occurs during invasion by broad tapeworm (diphyllobothriasis), a type of tapeworm that parasitizes the small intestine. Infection occurs when eating unprocessed fish. The development of pernicious anemia as a result of diphyllobothriasis is observed mainly in northern countries (for example, 3% of the total number of this disease identified in Finland). Competitive absorption is also observed when the small intestine is colonized by microorganisms (the small intestine is normally sterile, since microorganisms that enter with food or during reflux through the ileocecal valve are in transit in it). A permanent bacterial flora in the small intestine is formed in the presence of anatomical anomalies (fistulas, diverticula, etc.).
- As a result of impaired transport of vitamin B12. Occurs with congenital absence of vitamin B12-binding components (congenital, transient and partial deficiency of the transport protein transcobalamin II) and with Imerslund-Gresbeck syndrome (occurs as a result of impaired transport of vitamin B12 to intestinal epithelial cells).
The causes of the disease also include an autoimmune factor - in 90% of patients, the presence of circulating autoantibodies to stomach cells that secrete hydrochloric acid and intrinsic Castle factor was detected (present in 5-10% of healthy people), and in 60% of patients - antibodies to intrinsic factor Castle.
Risk factors for anemia
It is possible to identify some factors that may increase the likelihood of developing the disease, but even if they are all present, there is no certainty that this will happen:
- Genetic susceptibility : the presence of certain genes may predispose to the occurrence of pernicious anemia (in particular, the HLA-DRB1*03 and HLA-DRB1*04 genes). These are genes involved in immune response mechanisms.
- Autoimmune diseases : People with conditions such as type 1 diabetes, Graves' disease, thyroiditis, Addison's disease, hypoparathyroidism, vitiligo, chronic inflammatory bowel disease (Crohn's disease, ulcerative rectocolitis) are at increased risk of developing pernicious anemia; in all these cases there is a genetic predisposition to autoimmune diseases.
- Prevalence increases with age : in most cases, patients are around 60 years old at the time of diagnosis, however it is thought that the onset of the disease may be earlier, by around 20 to 30 years, and so pernicious anemia is sometimes diagnosed in younger people.
- Although widespread, the condition is more common in northern Europe (especially the Scandinavian countries, England and Ireland), and is poorly represented in eastern ethnic groups.
- Female gender : Prevalence is slightly higher in women.
Pathogenesis
Normally, 6-9 mcg of vitamin B12 per day enters the human body with food (2-5 mcg is excreted, and about 4 mcg is retained in the body). Since the reserves of vitamin B12 in the body are significant, malignant anemia develops only after a long period (about 4 years) after its supply has ceased or its absorption has been impaired.
Insufficiency of cyanocobalamin (vitamin B12) leads to a deficiency of its coenzyme forms - methylcobalamin and 5-deoxyadenosylcobalamin. Methylcobalamin is necessary for the normal course of the formation of red blood cells, and 5-deoxyadenosylcobalamin ensures metabolic processes occurring in the central nervous system and peripheral nervous system.
With a deficiency of methylcobalamin, the synthesis of nucleic acids and essential amino acids is disrupted and the megaloblastic type of hematopoiesis develops. In the process of formation and maturation, red blood cells take the form of megaloblasts and megalocytes, which are quickly destroyed and are not able to perform an oxygen transport function. As a result, the number of red blood cells in the peripheral blood is significantly reduced and an anemic syndrome develops.
An insufficient amount of 5-deoxyadenosylcobalamin causes a disturbance in the metabolism of fatty acids, which provoke the accumulation of toxic methylmalonic and propionic acids in the body. These acids have a damaging effect on the neurons of the brain and spinal cord, contribute to disruption of myelin synthesis and degeneration of the myelin layer, so pernicious anemia is accompanied by damage to the nervous system.
Development of pernicious anemia during pregnancy
The disease can develop in pregnant women. Pernicious anemia occurs as a result of insufficient intake of folic acid and cyanocobalamin into the body of the expectant mother. At the same time, the level of red blood cells in the blood decreases, but hemoglobin remains normal or increases. The disease develops quite slowly, and in order to make a diagnosis of “pernicious anemia” at an early stage, it is necessary to conduct a clinical blood test. Therefore, timely completion of all tests prescribed by the doctor is extremely important. The disease manifests itself as pale skin, weakness, increased fatigue, and later digestive disorders occur. Damage to the nervous system is extremely rare; a slight decrease in sensitivity in the extremities may be observed.
During pregnancy, pernicious anemia must be cured, since in most cases the pathology can provoke placental abruption, the risk of premature birth and stillbirth.
Treatment of the disease is carried out according to the general scheme.
Symptoms
Pernicious anemia manifests itself:
- Anemic syndrome, which is accompanied by general weakness, decreased performance, low-grade fever, dizziness, and fainting. The syndrome is also manifested by shortness of breath, which occurs even with minor exertion, tinnitus and flashing “spots” before the eyes. The skin becomes pale with a slightly yellowish tint, and the face becomes puffy. Auscultation of the heart may reveal systolic murmurs, and with prolonged anemia, myocardial dystrophy and heart failure develop.
- Gastroenterological syndrome, which is accompanied by nausea and vomiting, decreased appetite and body weight, and constipation. Gunter's glossitis also occurs (the structure of the tongue changes due to a lack of vitamin B12), in which the tongue acquires a crimson or bright red hue, and its surface becomes smoothed, “varnished.” The patient experiences a burning sensation in the tongue. It is possible to develop angular (localized in the corners of the mouth) stomatitis. Gastric secretion is significantly reduced; gastroscopy reveals atrophic changes in the gastric mucosa.
- Neurological syndrome. With a deficiency of vitamin B12, muscle weakness is observed, the gait becomes unstable, the legs become stiff, and the patient experiences numbness in the limbs. Long-term deficiency of vitamin B12 leads to damage to the spinal cord and brain (vibration, pain and tactile sensitivity disappears, convulsions occur). An examination by a neurologist reveals an increase in tendon reflexes, the presence of Romberg's symptom (loss of balance with eyes closed) and Babinski's reflex (extension of the first toe during line irritation of the skin of the outer edge of the sole), signs of funicular myelosis.
Megaloblastic anemia may be accompanied by irritability, low mood, and difficulty urinating. Sometimes impotence and visual disturbances develop. If the brain is damaged, the perception of yellow and blue colors may be impaired; in rare cases, hallucinations and other mental disorders are observed.
Symptoms and complications
In most cases, there are no early signs of pernicious anemia. As the disorder progresses, shortness of breath and decreased endurance during exercise or activity may occur. A noticeable rapid heartbeat can also be an obvious symptom of B12 deficiency anemia.
People with this disorder often have very low hemoglobin , but there are few symptoms of low hemoglobin, such as fatigue. They may also develop low levels of white blood cells (which are important for fighting infections) and platelets (which are essential for blood clotting and stopping bleeding). However, infections and bleeding are rare in people with pernicious anemia.
Other symptoms that may develop include:
- pale skin;
- painful, red, shiny tongue (see photo above);
- lack of appetite and weight loss;
- tingling and numbness in the hands and feet;
- disturbance of gait and balance (especially in the dark);
- mental changes, including memory loss, irritability, mild depression and dementia;
- yellow-blue color blindness.
Diagnostics
Pernicious anemia is diagnosed using:
- Analysis of patient complaints and medical history, during which the doctor clarifies the duration of the disease, the presence of hereditary and concomitant diseases, etc.
- Physical examination findings. During the examination, the doctor pays attention to the shade of the skin, pulse and blood pressure (with B12-deficiency anemia, the pulse is often rapid and blood pressure is reduced). The tongue must be examined.
- Laboratory test data.
Laboratory tests include:
- A blood test that can detect a decrease in the number of red blood cells, an increase in their size, a decrease in red blood cell precursor cells (reticulocytes), a decreased level of hemoglobin, a decreased content of platelets and an increase in their size. A change in the color indicator (the ratio of the first three digits of the number of red blood cells and a 3-fold increase in hemoglobin level) is also detected - in the direction of increase - with a norm of 0.86 to 1.05, with pernicious anemia this ratio exceeds 1.05.
- Urinalysis, which allows you to identify concomitant diseases (pyelonephritis, etc.), as well as suggest a hereditary form of the disease.
- A biochemical blood test to detect a decrease in the level of vitamin B12 in the blood, determine the level of cholesterol, uric acid, glucose, and detect creatinine (a protein breakdown product). Megaloblastic anemia is often accompanied by an increase in the level of bilirubin, formed from the breakdown of red blood cells, in the level of iron as a result of a decrease in its use in the formation of new red blood cells, and in the level of the enzyme lactate dehydrogenase, which accelerates chemical reactions.
To examine the bone marrow under general anesthesia, a puncture is made in the area of the anterior and posterior iliac spines (to avoid data distortion, the study is carried out before vitamin B12 is prescribed). Analysis of the myelogram allows us to detect the megaloblastic type of hematopoiesis and increased formation of red blood cells.
In addition, they carry out:
- ECG, which can detect an increased heart rate and, in some cases, irregular heart rhythms.
- Gastroscopy, which reveals the absence of hydrochloric acid in gastric juice (achlorhydria) and atrophic gastritis, affecting the sections in which the secretion of hydrochloric acid and pepsin occurs. Since gastric epithelial cells look atypical during cytological examination, a differential diagnosis is made with gastric cancer.
- X-ray of the stomach, ultrasound of the abdominal organs.
- MRI of the brain and examination by a neurologist.
Vitamin B12 absorption is assessed using the Schilling test. The patient takes radioactive vitamin B12 orally, and a few hours later he is given a “loading” dose of the unlabeled vitamin parenterally. The content of radioactive vitamin in 24-hour urine is then measured. With preserved kidney function, a decrease in its secretion indicates a decrease in the absorption of vitamin B12 in the intestine.
Symptoms
Symptoms of anemia
Megaloblastic anemia symptoms are nonspecific, that is, those that cannot accurately indicate the course of this particular disease. The main external clinical signs of this disease are presented:
- increased heart rate;
- pale skin;
- dizziness;
- weakness and fatigue;
- heart murmurs;
- slight increase in temperature indicators;
- shortness of breath during physical activity;
- decreased appetite;
- stool disorder;
- dryness, burning and pain in the tongue;
- acquisition of a crimson hue on the tongue;
- numbness and limited mobility of the limbs;
- muscle weakness;
- change in gait;
- paraparesis of the legs;
- urinary and fecal incontinence;
- impairment of pain, tactile and vibration sensitivity;
- problems with sleep, up to its complete absence;
- depression and psychosis;
- hallucinations;
- decreased cognitive abilities;
- menstrual irregularities in females;
- decreased sexual desire for the opposite sex;
- emotional instability;
- loss of body weight;
- tinnitus;
- the appearance of “flies” before the eyes;
- fainting states.
Symptoms of pernicious anemia in children, in addition to the above, include:
- growth retardation;
- violation of harmonious development;
- a decrease in the resistance of the immune system, which is why inflammatory and infectious diseases very often occur, and chronic diseases are much more severe.
Treatment
Treatment of megaloblastic anemia is aimed at eliminating the cause of the disease and normalizing hematopoiesis. Therapy includes:
- Treatment of gastrointestinal diseases (for autoimmune damage to the stomach, glucocorticosteroids are prescribed), a balanced diet, which includes fermented milk products, beef, seafood, eggs and rabbit meat.
- The use of praziquantel or phenasal for diphyllobothriasis.
- Replenishment of vitamin B12 deficiency.
Pernicious anemia is treated by administering cyanocobalamin (vitamin B12) for 4 to 6 weeks, 200 to 500 mg subcutaneously once a day. Then the vitamin is administered once a week (a course of 3 months), and then they move on to injections 2 times a month for six months (the dose does not change).
Normalization of hematopoiesis occurs approximately 2 months after the start of treatment (the exact timing depends on the severity of the anemia).
Red blood cell transfusion is performed only in cases of anemic coma or severe anemia.
Treatment of pathology
If pernicious anemia is diagnosed, treatment is carried out by administering medications such as Oxycobalamin or Cyanocobalamin. The drugs are administered by injection. First of all, it is necessary to bring the concentration of vitamin B12 to normal values, later the number of injections is reduced, and the administered medicine has only a supporting effect. After therapy, patients will have to constantly monitor their vitamin levels and periodically undergo a preventive course of drug injections.
In some cases, during treatment, patients may experience a decrease in iron concentration in the body. This usually happens after 3-6 months of treatment. In such a situation, additional administration of medications that restore iron levels is required.
With successful therapy, all manifestations of the disease gradually disappear. The duration of the recovery period can be 6 months. The content of vitamin B12 is normalized 35-70 days after the start of treatment.
During the treatment, neuropathy is eliminated, urinary incontinence and other symptoms disappear in all patients. Unfortunately, vision that has been impaired as a result of optic nerve atrophy is not restored. But if visual impairment occurs as a result of hemorrhages of the macula, then recovery occurs quite quickly.
It should be borne in mind that in some cases, after treatment, serious diseases such as toxic goiter, myxedema, and stomach cancer may develop. However, this happens quite rarely (no more than 5% of cases).
Exodus
Death with pernicious anemia is possible if there is a malignant tumor. Even with long-term treatment, the outcome will depend on further actions. The outcome is favorable if the patient follows some recommendations.
First of all, the outcome will depend on lifestyle and nutrition adjustments. Especially in the presence of an intoxication factor and nutritional etiology. In people over seventy years of age, the outcome is often unfavorable.
Recovery is possible. But therapeutic therapy is quite long. May vary from several years. Moreover, the outcome in this case may be associated with lifelong intake of this vitamin.
go to top