Functions of the circulatory organs
The most important functions of the circulatory organs are: maintaining the constancy of the body’s environment under continuously changing conditions of its life; delivery of oxygen and nutrients to all organs and tissues; removal and excretion of carbon dioxide and other metabolic products. These functions are carried out in close interaction with the respiratory, digestive and urinary organs under the regulatory influence of the central nervous, autonomic and endocrine systems.
Growth, structural and functional improvement of the circulatory organs themselves continue throughout the entire period of childhood and occur unevenly, with not simultaneous maturation of individual parts, and the intense metabolic processes ongoing in the child place high demands on their activity.
Cardiovascular system of the newborn
The formation of the heart and large vessels occurs in the 3rd week of the embryonic phase, the first contraction of the heart occurs in the 4th week; Listening to heart sounds through the mother's abdominal wall is possible from the fourth month of pregnancy.
Intrauterine circulation of the newborn
Oxygen-enriched blood flows from the placenta through the ductus venosus (Arantius) into the inferior vena cava and mixes there with venous blood flowing from the lower extremities. Most of this mixed blood, thanks to a special valve of the inferior vena cava (Eustachian valve) in the right atrium, is directed through the oval window into the left atrium, the left ventricle, and from there into the aorta and through the subclavian arteries to the brain and upper limbs. Venous blood from the upper half of the body is sent to the right ventricle, then through the pulmonary artery and ductus arteriosus to the descending aorta. Thus, the brain and liver receive the most, and the lower extremities the least, oxygen-rich blood. After the birth of a child, the venous duct and umbilical vessels become empty, overgrow by the end of the 2nd week of life and turn into the round ligament of the liver and hepato-umbilical ligaments, respectively. The ductus arteriosus, and after it the oval window, close at 6–8 weeks, and sometimes at 3–4 months of life.
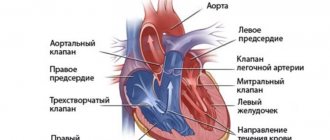
Newborn heart
The heart of a newborn is relatively large and makes up approximately 0.8% of his body weight (by 6 months - 0.4%, by 3 years and in all subsequent periods - about 0.5%). The most intense increase in the mass and volume of the heart (mainly due to length) occurs in the first years of life and adolescence. However, during all periods of childhood, the increase in heart volume lags behind the growth of the body as a whole. In addition, the parts of the heart increase unevenly: up to 2 years, the atria grow most intensively, from 2 to 10 years - the entire heart as a whole, after 10 years, mainly the ventricles increase. The left ventricle grows faster than the right. The ratio of the thickness of the walls of the left and right ventricles of the heart in a newborn is 1.4:1, at 4 months - 2:1, by 15 years - 2.76:1.
The mass of the left ventricle is also greater than that of the right. During all periods of childhood, with the exception of the ages from 13 to 15 years, when girls grow faster, boys' heart sizes are larger. Up to 6 years of age, the heart shape is usually round; after 6 years, it approaches the oval shape characteristic of adults. The location of the heart changes with age: up to 2 - 3 years, it lies horizontally on a raised diaphragm, and the right ventricle is adjacent to the anterior chest wall, forming mainly the apical cardiac impulse. By 3–4 years of age, due to an enlargement of the chest, a lower position of the diaphragm, and a decrease in the size of the thymus gland, the heart assumes an oblique position, simultaneously rotating around its long axis with the left ventricle forward. The interventricular septum is adjacent to the anterior chest wall; the cardiac impulse forms predominantly the left ventricle.
Coronary vessels up to 2 years of age are distributed according to the scattered type, from 2 to 6 years - according to the mixed type, after 6 years - according to the adult, main type. The lumen and thickness of the walls (due to the intima) of the main vessels increase, and the peripheral branches are reduced.
Abundant vascularization and loose fiber surrounding the vessels create a predisposition to inflammatory and dystrophic changes in the myocardium. The formation of sclerosis at an early age is rare, myocardial infarction is a casuistry.
Newborn myocardium
The myocardium of the newborn is an undifferentiated syncytium. The muscle fibers are thin, do not have transverse striations, and contain a large number of nuclei. Connective and elastic tissue is not developed. In the first 2 years of life, intensive growth and differentiation of the myocardium occurs: muscle fibers thicken, transverse striations appear, septal septa and a subendocardial layer are formed. At the age of 6 to 10 years, slow differentiation and growth of the myocardium continues, and by 10 years, its histological structure is similar to that of adults. In parallel, the development of the histological structures of the conduction system of the heart, which is a specialized myocardium devoid of contractile function, proceeds and ends by the age of 14-15 years. Innervation of the heart occurs through superficial and deep plexuses formed by fibers of the vagus nerve and cervical sympathetic nodes, which contact the ganglia of the sinus and atrioventricular nodes in the walls of the right atrium. The branches of the vagus nerve complete their development and myelinate by 3–4 years. Until this age, cardiac activity is regulated mainly by the nervous sympathetic system, which is partly responsible for physiological tachycardia in children of the first years of life. Under the influence of the vagus nerve, the heart rate slows down and sinus arrhythmia (such as respiratory arrhythmia) and individual “vagal impulses”—sharply prolonged intervals between heart contractions—may appear. Reflex effects are carried out by interoceptors of both the heart itself and other internal organs, which changes the rhythm frequency under the influence of various physiological factors and is regulated by the central nervous system. Myocardial functions such as automaticity, excitability, conductivity, contractility and tonicity are carried out similarly to those in adults.
Vessels of the newborn
Blood is carried and distributed to organs and tissues by vessels. Their lumen in young children is relatively wide: the arteries are equal in width to the veins. The walls of the arteries are more elastic, so peripheral resistance, blood pressure and blood flow speed in healthy children in the first years of life are lower than in adults. The growth of arteries and veins is uneven and does not correspond to the growth of the heart: by the age of 15, the circumference of the aorta increases 3 times, and the volume of the heart increases 7 times. Veins grow more intensively, and by this age they are 2 times wider than arteries. The histological structure of the arteries also changes: in newborns the walls of the vessels are thin, their muscle and elastic fibers and the subendothelial layer are poorly developed. Until the age of 5, the muscle layer grows more intensively, at 5 - 8 years all the membranes grow evenly, at 8 - 12 years the connective tissue elements differentiate and predominantly the intima grows, by the age of 12 the structure of the vessels is the same as in adults.
Capillaries of a newborn
In children, the capillaries are well developed, wide, their number is 6-8 in the linear field of vision (in adults 8-10). The shape of the capillaries is irregular, they are short and convoluted. In newborns, the subpapillary venous plexuses are well defined and located superficially. With age, they are located deeper, the capillary loops lengthen and take on a hairpin shape. Capillary permeability is significantly higher than in adults.
Basic mechanisms of disease development
- Congenital calcification of the heart valves, as well as the main and coronary vessels as a result of complex biochemical processes inherent at the genetic level. This type of disease is diagnosed in childhood and is very difficult to correct with medication;
- Metastatic calcification occurs when the normal processes of calcium removal from the body through the digestive tract, kidneys, etc. are disrupted;
- If calcium is freely deposited on the surface of the heart valves and blood vessels, then we are talking about universal calcinosis with an increase in the susceptibility of organ structures to the penetration of trace element compounds into their walls;
- Dystrophic calcification is a pathological process that was preceded by deep disturbances in the nutrition of body tissues, which served as the basis for the formation of the so-called “armored” heart and pulmonary failure.
Features of the circulatory system
Functional features of the circulatory organs in children
The functional features of the circulatory system in children include:
1.
A high level of endurance and working capacity of the child’s heart, which is associated both with its relatively larger mass and better blood supply, and with the absence of chronic infections, intoxications and harmful substances;
2.
Physiological tachycardia, caused, on the one hand, by the small volume of the heart with the body’s high needs for oxygen and other substances, on the other hand, by sympathicotonia characteristic of young children;
3.
Low blood pressure due to the small volume of blood flowing with each heartbeat and low peripheral vascular resistance due to the greater width and elasticity of the arteries;
4.
The possibility of developing functional disorders of activity and pathological changes due to uneven growth of the heart, its individual parts and vessels, peculiarities of innervation and neuroendocrine (during puberty) regulation.
Causes of aortic calcification
Calcification of the walls of the aorta and the valve apparatus of the heart organ provokes a disturbance in the metabolic process in the human body.
The causes of aortic calcification may be:
- Pathologies of the parathyroid gland;
- Hyperparathyroidism disease;
- Parathyroid adenoma;
- Malignant neoplasms of endocrine organs;
- Pathologies of the adrenal glands;
- Thyroid disease;
- Disturbance in the functioning of the sex glands;
- Diseases of the intestines that are associated with the absorption of calcium molecules;
- Cyst on the kidney organ;
- Pathology nephropathy;
- Pathologies of the urinary organs;
- Previous illness rheumatic fever in acute form.
Risk factors for the development of calcinosis include the following pathologies:
- Injury to soft muscle tissue cells;
- Fractures of bone tissue;
- Pathology hypervitaminosis of vitamin D;
- Oncological neoplasms of different localization;
- Pathologies of blood composition and hemostatic system;
- Heart defects that have a congenital or acquired etiology;
- Surgical intervention in the heart organ, or in the main arteries of the blood flow system;
- Anomalies in the structure of the arteries, in which fibrosis forms and calcified plaques accumulate on the walls of the arterial membranes;
- Pathology osteoporosis;
- Degenerative aorta in old age;
- Hereditary genetic predisposition of the body to calcinosis;
- High blood pressure index - hypertension;
- Systemic pathology atherosclerosis;
- Diseases of the endocrine system, which provoked diabetes.
The reasons for the development of aortic calcification are an unhealthy lifestyle:
- Nicotine addiction;
- Alcoholism;
- Sedentary lifestyle;
- Overweight - obesity;
- Poor nutrition;
- A constant state of stress.
Methods for studying the cardiovascular system
Methods for studying the cardiovascular system of a newborn
When assessing the state of the circulatory organs, the following are used: complaints, questioning (of mothers and older children) and objective methods: examination, palpation, percussion, auscultation, counting the pulse and measuring blood pressure, instrumental and graphic research methods.
Complaints.
Children rarely complain, usually with a severe general condition. The most common symptoms are shortness of breath when moving or at rest, indicating the presence of heart failure, general weakness, fatigue, palpitations, and at puberty (with vegetative-vascular dystonia) - pain in the heart area.
Questioning.
Relatively uninformative, since the mother usually pays attention only to very pronounced changes. However, with the help of the mother, it is necessary to clarify the genetic Jr obstetric history, obtain information about the course of pregnancy and the mother’s illnesses at this time, the characteristics of the child’s development and behavior, the diseases he has suffered and their connection with the time of the appearance of shortness of breath, palpitations, cyanosis, edema and other clinical symptoms.
Inspection
(general, area of the heart and large vessels). Upon examination, changes in skin color (cyanosis, pallor), visible pulsation of the cervical vessels, epigastrium, area of the apex of the heart (heartbeat), deformations of the chest and fingers, and severe swelling are detected.
Palpation.
This method is carried out in parallel with the examination and allows you to detect systolic and diastolic tremors, clarify the nature and location of the heart impulse, pulsation of the intercostal spaces, and pastosity of the legs. When palpating the entire area of the heart with the palm of your hand, you can feel a “cat’s purr” - diastolic tremors with narrowing of the mitral valve and an unclosed ductus arteriosus, or a more coarse systolic tremor with congenital aortic valve stenosis and a high ventricular septal defect.
The cardiac impulse in healthy children under 2 years of age is palpated in the fourth intercostal space outward from the midclavicular line, at 5-7 years - in the fifth intercostal space along the nipple line, after 7 years - inward from it. It can be weakened when the apex is located behind the ribs or strengthened when the child is excited and does physical work. Changing position can change the location of the push.
In pathological conditions, increased impulse indicates hypertrophy or heart disease, expansion and weakening indicate current myocarditis, exudative pericarditis, cardiac decompensation, collapse, emphysema, obesity. A shift of the impulse to the right is possible when the position of the mediastinum changes due to left-sided exudative pleurisy, pneumothorax, tumor or echinococcus of the lung, as well as atelectasis and fibrosis of the right lung. A downward shift indicates left ventricular hypertrophy, an upward shift indicates pericarditis or a high position of the diaphragm (with flatulence, ascites, etc.).
Pastiness of the legs indicates the initial stages of cardiac decompensation and is determined, as in adults, by pressing on the anterior surface of the tibia.
Percussion.
This research method has its own characteristics. Tapping should be weak, done with finger over finger from the lung to the heart along lines parallel to all its boundaries, always in different positions of the child’s body. The boundaries of the heart in children are compared with age norms in groups: up to 2 years, from 2 to 7 years and from 7 to 12 years.
After 12 years, the limits of relative dullness are the same as in adults. A decrease in the boundaries of the heart is observed in shock conditions and a decrease in the volume of circulating blood, pulmonary emphysema of any origin, total left-sided pneumothorax, and a diaphragmatic hernia located on the left. An increase in the boundaries is observed with hypertrophy and expansion of the cavities of the heart, congenital and acquired defects, subendocardial fibroelastosis, pericarditis, chest deformities, hypertension of the pulmonary circulation.
The shape of the heart, determined by percussion, is also important: mitral configuration for bicuspid valve stenosis, a “shoe” with a sharply emphasized waist for tetralogy of Fallot and aortic insufficiency, triangular for pericarditis.
Changing the position of the patient can change the boundaries of the heart, which is especially clearly visible in case of myocardial hypotension: in a horizontal position on the back, the boundaries are usually as wide as possible; while sitting and standing, they are reduced.
Auscultation.
This research method is also carried out in different positions of the patient, since the observed changes in the nature of tones and noises often have diagnostic significance. It is advisable to use a stethoscope or a small-diameter phonendoscope without a membrane. Do not apply excessive pressure on the chest with a stethoscope, as this weakens the sonority of heart sounds and causes pain to the child. There are also features in the auscultatory picture of the heart sounds of a healthy child: greater sonority of tones over the entire cardiac region than in adults (after 2 years), a clearly audible second sound at the apex, after 2 years - its slight accent and sometimes inconsistent splitting over the pulmonary artery , accent of the second tone over the aorta when listening to a child in a cold room. In newborns up to two weeks of age, embryocardia is determined against the background of physiological tachycardia (equality of pauses between I and II, II and I tones); the sounds, especially I, are somewhat weakened in children under 2 years of age. After 2 - 3 years, up to puberty, more than half of children hear functional noises.
With a functionally complete myocardium, an increase in tones accompanies physical and mental agitation, fever, anemia, thyrotoxicosis, compaction of the adjacent parts of the lung, and hypertension.
The first sound intensifies to a flapping sound at the apex of the heart or above the projection of the mitral valve when it narrows. The emphasis of the second tone on the aorta is determined by increased work of the left ventricle in hypertension of any origin. The emphasis of the second tone on the pulmonary artery occurs when the right ventricle is functional and the pressure in the pulmonary circulation increases in acute and chronic pneumonia, emphysema, whooping cough, defects of the interatrial and interventricular septa, unclosed ductus arteriosus, insufficiency and stenosis of the mitral valve, etc.
Weakening (muffling) of tones is observed in cardiac disorders associated with diffuse myocardial damage, exudative pericarditis, congenital defects, and non-cardiac causes are also possible: emphysema, obesity, edema and induration of the anterior chest wall with scleroderma. Isolated weakening of the first tone is observed in acute myocarditis, mitral valve insufficiency, and aortic stenosis.
Variable splitting and splitting of tones associated with the phases of breathing can be observed in healthy children due to the physiological asynchronism of the ventricles. Constant pronounced pathological splitting and bifurcation indicate either a sharp hypertrophy of one of the ventricles or a blockade of the legs of the atrioventricular bundle (bundle of His).
Arrhythmias (with the exception of sinus and respiratory) are less common in children than in adults. They are relatively often observed in infectious-allergic myocarditis. The presence of a gallop rhythm (presystolic and protodiastolic), embryocardia (after two weeks of age), pendulum-shaped and three-membered rhythms always indicates a serious myocardial pathology (hypertrophy, sclerosis, interstitial myocarditis).
Treatment options
Normalization of the condition with calcinosis is of great importance, so it is important to confirm the pathology in time and begin comprehensive treatment as soon as possible. Many people are interested in the question of how to treat aortic calcification and what to pay close attention to. As a rule, doctors prescribe medications and a special diet, but in some cases the patient may require surgical treatment of diagnosed vascular calcification. With standard treatment, the progression of the disease is noticeably reduced, but complete recovery is possible only after surgery.
Important! A timely diagnosis will save the patient’s life, therefore, when the first symptoms of calcinosis are detected, it is recommended to undergo examination and begin treatment as soon as possible.
The goal of treatment for this pathology is to restore the balance of electrolytes and blood acidity levels, maintaining the balance of magnesium and calcium. Special nutrition helps compensate for magnesium deficiency and significantly reduce the amount of calcium in the body by eliminating or reducing dairy products, certain vegetables and vitamin D.
Doctors prescribe patients to take medications containing magnesium, diuretics, blood pressure normalizers, and cardiotrophic medications. Good results are obtained by taking drugs to cleanse blood vessels: nicotinic acid and statins.
Treatment of calcinosis
If the diagnosis of calcification is made to an elderly person, in this case surgery is usually recommended (when we are talking about a serious stage of calcification). Prosthetics of the aorta, coronary vessels and heart valves can prevent sudden death and prolong the patient’s life.
To expand the aorta, the patient undergoes balloon valvuloplasty or completely replaces the aortic valve with a prosthesis. Surgical treatment is a last resort measure that can produce quick and tangible results.
The presented video describes traditional treatment methods:
Cardiovascular system disorders
Disorders of the cardiovascular system of the newborn
Cyanosis can be general and local (lips, ears, cheeks, mucous membranes, distal extremities) and is observed more often in children with congenital “blue” heart defects, especially when walking and running, as well as in decompensated acquired defects, severe myocarditis, diseases lungs.
Paleness with a grayish or slightly jaundiced tint can be with rheumatism, with a brownish (café-au-lait color) - with prolonged bacterial endocarditis.
Pulsation of the apex of the heart may indicate a congenital defect or acquired damage to the aortic valves and ventricular hypertrophy.
With a healthy heart, pulsation of this area can be observed during neurasthenia, during puberty and with anemia. Pulsation of the cervical vessels and epigastric region is most often associated with damage to the aortic valves (insufficiency) or the right ventricle with its hypertrophy and congestion in large veins.
With myocardial hypertrophy, which accompanies congenital and acquired heart defects in early childhood, a cardiac hump often forms. Obliteration of the pericardium and its fusion with the anterior chest wall can cause retraction of the cardiac region and a “negative” cardiac impulse. Long-term hypoxemia forms fingers in the form of drumsticks in children with congenital and acquired defects and cardiopathy. Swelling of the legs, abdominal wall, and bulging of the navel due to ascites are observed rarely and only in cases of severe heart failure.
Heart murmurs
Heart murmurs are heard extremely rarely in healthy children under 2 years of age. In older people, especially in puberty, inorganic, functional murmurs, usually systolic, are often detected. They can be a consequence of innervation disturbances and subsequent dysfunction of the papillary muscles and notochordal apparatus, compression of large vessels, changes in the direction of blood flow and its composition (hydremia), etc.
Functional noises are characterized by:
1.
Inconsistency, variability in duration (usually short), strength and timbre, localization (usually determined at the base of the heart and on large vessels);
2.
Dependence on body position (best heard lying down), breathing phases (disappear or sharply weaken at the depth of inspiration), physical activity (change intensity and timbre).
Organic systolic murmurs are associated with morphological changes in valves and large vessels, their incorrect location, the presence of extra holes and gross inflammatory or sclerotic changes in the myocardium. They are characterized by constancy, duration, rough or “blowing” timbre, localization at certain points, conduction along the blood flow (for example, to the apex in case of mitral valve insufficiency due to blood regurgitation), frequent combination with diastolic murmurs, which almost always have an “organic” quality. origin. These noises are not associated with body position and breathing phases; physical activity does not change their character.
Pericardial murmurs are heard extremely rarely in children, usually in a limited area along the anterior surface of the heart, resemble the scratching or crunching of snow, intensify when the torso is tilted forward, or when a phonendoscope is pressed on the chest, are not associated with the phases of the cardiac cycle and breathing, and are not carried out to other points.
In some cases, murmurs of extracardiac origin are detected (in large vessels, pleuropericardial, etc.). The final decision about the nature and origin of the noise can be made only after a phonocardiographic study.
Clinical Vascular Study
This study includes counting and characterizing the pulse (on the temporal artery in the youngest and on the radial artery in older ones) and measuring blood pressure. It is advisable to count and evaluate the pulse simultaneously with a breathing test at the very beginning of the examination, when the patient is in a calm state (or during sleep), since the rhythm frequency changes when excited, crying, moving, or eating.
In children of all age groups, there is one respiratory movement per 3-4 heartbeats. In healthy children, the pulse is rhythmic or a moderate respiratory arrhythmia is detected with an average pulse filling. An increase in heart rate in healthy children can be observed with excitement, muscle work, an increase in body temperature (for every 1 °C by 15 - 20 beats), and with acute febrile diseases.
Tachycardia occurs with scarlet fever and other childhood infections, hyperthyroidism, diffuse connective tissue diseases, cardiac and respiratory failure.
A weak and frequent pulse indicates a drop in cardiac activity and is a prognostically unfavorable symptom, especially with concomitant cyanosis, cold extremities, weakened heart sounds, enlarged liver (in severe toxic conditions, diphtheria, dysentery, pneumonia).
A tense, increased pulse is most often observed with increased work of the left ventricle and its overcoming resistance to the outflow of blood (during physical activity, hypertension, spasm of small arteries and capillaries during nephritis).
A slowing of the pulse occurs in healthy children during sleep due to the predominant influence of the vagus nerve, as well as in tuberculous meningitis, peritonitis, typhoid fever, and during the period of convalescence after scarlet fever and measles.
Blood pressure measurement
It is carried out, as in adults, according to the Korotkov method, preferably using special children's cuffs of different sizes (up to 2 years - 2 - 4 cm, for 3 - 6 years - 6 - 8 cm, for schoolchildren - 10-12 cm). Normal values are calculated in millimeters of mercury based on the patient’s age using V.I. Molchanov’s formula for maximum pressure: 80 + double the number of years. The minimum, as in adults, is 1/ъ^1/2 of the maximum. For larger children - accelerators, the initial figure is taken not 80, but 90 mmHg. Art. In newborns and children in the first year of life, the maximum blood pressure is less than 80. An increase in blood pressure can occur with stress and excitement of the child, but more often it is a symptom of nephritis, periarteritis nodosa, and vegetative dystonia of the puberty period. A decrease in blood pressure is observed in infectious-toxic shock and collapse, serum sickness, severe infectious diseases, heart failure, and myocarditis.
What does calcification of blood vessels lead to?
If calcification of the aorta and aortic valve occurs, this is a direct threat to the patient’s life, because calcification of the aortic walls loses their elasticity and strength.
In case of damage to the aorta, the disease poses a direct threat to human life, since calcium deposits on the walls deprive them of elasticity.
For the aorta, a risk factor for the development of pathology may be high blood pressure, which can injure or completely rupture the aortic membrane.
Aortic ruptures are instantly fatal. An increase in blood pressure causes calcification of the aortic valve leaflets, as well as the deposition of calcium masses on the aorta, which leads to a significant narrowing of the aortic lumen.
Calcium salt ions are deposited on all arteries of the blood flow system, which causes their narrowing. The most dangerous are: calcium deposits in the heart and brain vessels.
Aorthocalcinosis of the root and arch of the aorta, coronary arteries, aortic and mitral valves quickly leads to the development of myocardial infarction with a fatal outcome.
80.0% of heart attacks with aortic calcification end in premature death. Atherocalcinosis of the cerebral arteries provokes a hemorrhagic stroke with a fatal outcome.
92.0% of strokes with calcification of the internal carotid arteries of the cervical spine and cerebral vessels result in the death of the patient.
Symptoms
The manifestation of the disease occurs when the level of calcium in the blood increases above 3 mmol per liter. In this case, the following clinical picture can be observed in the newborn:
- frequent regurgitation,
- vomit,
- breast refusal,
- lag in weight gain,
- signs of anorexia,
- increased excitability,
- periodic seizures,
- hypertension,
- dehydration,
- constipation for more than 5-7 days,
- the appearance of dense purple nodules in the legs and buttocks.
Diagnosis of hypercalcemia in a newborn
The diagnosis is made based on studying the results of a blood test - based on the level of calcium in it. To identify the etiology of the disease, its complications and for differential diagnosis, the following methods can be used:
- urine and stool tests,
- ECG or EchoCG,
- magnetic resonance or computed tomography of internal organs,
- Ultrasound of the glands and abdominal organs,
- intravenous pyelography,
- denistometry,
- radiography.
Indications for such procedures may be:
- detection of pathologies during screening,
- complications during gestation,
- premature birth,
- presence of the disease in the mother.
What are calcifications and why are they dangerous?
Calcifications are an accumulation of calcium salts in any organ of the human body. Most often, during the examination, not one, but several such lesions are discovered, and the reason for their appearance has long been known - this is how the body tries to cope with dead tissue that may appear after injury or inflammation. It turns out that calcifications are a kind of defense of the body, when those areas that, over time, as a result of decomposition, can cause enormous harm, are literally packed into such “capsules”.
Traditional recipes against calcinosis
It is believed that it is possible to stop the development of calcinosis using garlic-based folk remedies. The unique ability of this plant to dissolve lime deposits was discovered by European scientists who conducted research on the effects of its biologically active substances on blood vessels. For preventive purposes, it is enough to eat only two cloves per day.
Chinese healers prepared garlic tincture from 300 grams of peeled and crushed garlic cloves and 200 grams of alcohol (vodka). After 10 days of infusion, it was taken according to the following scheme:
- 5 days, starting with one drop per 50 ml of cold milk, three times a day, adding one drop with each dose. In the evening of the fifth day, you need to drink 50 ml of milk with 15 drops of garlic tincture.
- 5 days, reducing one drop at each dose. On the 10th day in the evening you need to drink 50 ml of milk with one drop of infusion.
- Then take 25 drops at each dose until the tincture runs out.
The recipe for the “Elixir of Youth”, which was used by Tibetan monks to cleanse blood vessels and prolong life, has been preserved:
- They took 100 grams of dry herbs of chamomile, motherwort and birch buds. The mixture was thoroughly mixed and crushed. One tablespoon of the prepared mixture was brewed with 0.5 liters of boiling water and left for 20 minutes. A glass of warm, strained infusion with the addition of a tablespoon of honey should be drunk in the evening before bed. The second portion is drunk in the morning on an empty stomach.
Both of these balms effectively cleanse blood vessels, eliminating signs of atherosclerosis and calcification of the aortic walls , restoring their elasticity. It is recommended to use them once every five years.
Symptoms
Clinical signs of MARS in newborns are usually absent. In many children, such anomalies do not manifest themselves in any way at an older age. Symptoms of MARS may appear during the active growth of the child or after the onset of some acquired disease. Anomalies may appear:
- Pain or tingling in the heart.
- Feelings of interruptions in the work of the heart.
- Changes in blood pressure parameters.
- Weakness and fatigue.
- Dizziness.
If MARS is a symptom of connective tissue dysplasia, then the child will also have skeletal lesions, developmental abnormalities of other organs, autonomic changes and other signs of such a pathology.