Insufficient blood flow to the heart muscle leads to coronary artery disease. Its complication may be cardiomyopathy, in which the myocardium weakens to such an extent that it loses tone, and the chambers of the heart expand. Weak cardiac output provokes circulatory failure. With extensive damage to the heart muscle, death can occur if it is impossible to perform a heart transplant.
When is the diagnosis made?
In accordance with European and American cardiological standards, a similar diagnosis is made in up to 75% of patients in cases of heart failure and is defined as ischemic dilated cardiomyopathy. This does not correspond to the ICD, but reflects the cause and consequences of the disease.
Among all forms of coronary heart disease, cardiomyopathy accounts for 5–8%. And if the ischemic form is compared with general cases of pathology, then it will account for up to 13% of all cardiomyopathies.
The disease is detected predominantly in men (90% of cases), the most affected age is from 45 to 55 years.
Classification
All cardiomyopathies are divided into primary and secondary.
Primary diseases are divided into groups:
- Congenital, which appear during the period of intrauterine development, mainly due to maternal smoking, consumption of alcohol and medications, stress and anxiety, improper or insufficient nutrition.
- Acquired, arising after exposure to toxins, metabolic disorders or viruses.
- Mixed, combining both types of negative impact.
Secondary pathologies are caused by the following diseases or conditions:
- the effects of certain medications, including chemotherapy;
- alcoholism;
- endocrine diseases that provoke myocardial dysfunction;
- obesity;
- diseases of the gastrointestinal tract;
- eating disorders;
- diabetes;
- the use of harsh long-term diets leading to an acute lack of vitamins and nutrients;
- negative effects at the cellular level (radiation, toxins, poisons, etc.).
Also read: How does adhesive pericarditis manifest?
Primary cardiomyopathy is divided into types:
- dilated or ischemic;
- hypertrophic;
- restrictive;
- arrhythmogenic dysplasia.
Secondary diseases are of the following types:
- alcoholic;
- diabetic;
- thyrotoxic (associated with pathologies of the thyroid gland);
- stressful.
The ischemic form of the disease is called congestive due to the presence of poor blood supply.
Pathological changes in the heart
The narrowing of the coronary arteries causes a state of hypoxia of the most “working” cells in the body - myocytes. Lack of oxygen sharply reduces the possibility of energy production, since the biochemical process of producing calories requires the obligatory presence of oxygen molecules, enzymes, coenzymes, hormones, B vitamins, glucose, ketone bodies, amino acids, and fatty acids.
Myocytes “know how” to produce energy in an oxygen-free mode, but it is not enough to ensure the necessary functioning of the myocardium. As a result, the heart mass increases.
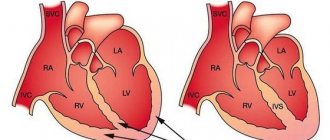
Some researchers prove thickening of the wall of the left atrium (more than 1.5 cm), much less often changes affect the right atrium. Thickening is not accompanied by a violation of the total volume of the chambers. Others claim that the wall thickness does not change (no more than 11 mm). There are cases of similar changes in the septum. At the initial stage, the left ventricle expands, then the right one is involved. The adaptation process takes from 3 to 6 months.
Pathological changes in the heart that are caused by ischemic cardiomyopathy are divided into 2 options:
- symmetrical shape - the increase concerns evenly the right and left parts of the heart;
- asymmetrical - one of the cameras is modified more than the other.
Functional changes can be called “weakness” of the heart muscle. The ability to pump blood into the vascular bed is depleted. Heart failure develops.
Risk factors
Experts have identified a number of risk factors that increase the likelihood of developing the disease. If these factors are present in your life, then they need to be removed as quickly as possible. Their list is as follows:
- presence of coronary artery disease in the family;
- stable high blood pressure;
- smoking and drinking alcohol;
- high cholesterol;
- large body weight;
- sedentary lifestyle;
- diabetes;
- accumulation of abnormal proteins in tissues (amyloidosis);
- advanced kidney pathologies.
Men are more susceptible to developing ischemic cardiomyopathy than women who have not reached menopause. After this period, the probability of developing ischemic cardiomyopathy becomes the same. In women over 35 who use oral contraceptives and have a nicotine addiction, the chances of developing ischemic cardiomyopathy increase.
Changes at the cellular level
In the myocardium, massive death of myocytes occurs due to small focal necrosis, fibrosis, replacement with adipose tissue and inflammation. Myofibrils change and disintegrate. Ischemia leads to various forms of myocyte damage:
- fiber dissolution (lysis) occurs;
- contractures (dense fibrous threads) form;
- “clumpy disintegration” - cutting of fibers into separate pieces is described as the most severe type of damage;
- new bundles of myofibrils are elongated and are not located along the line of contraction, therefore they “work” asynchronously and chaotically.
An area with altered myofibrils under a microscope
In 1984, a term arose in the United States that characterized cells as “dormant” and the myocardium “hibernated” (not capable of contracting). Functions in living cells decrease in proportion to the degree of circulatory disturbance in the coronary vessels. Scientists consider this mechanism to be adaptive, reducing the needs of the myocardium to match the incoming nutrition. In this case, no signs of a heart attack are detected.
At the same time, the name “stunned” myocardium was proposed. This dysfunction is characterized by the preservation of normal coronary blood flow at rest.
Severe ischemic cardiomyopathy: there is not much chance of survival without help
Insufficient blood flow to the heart muscle leads to coronary artery disease.
Its complication may be cardiomyopathy, in which the myocardium weakens to such an extent that it loses tone, and the chambers of the heart expand. Weak cardiac output provokes circulatory failure.
With extensive damage to the heart muscle, death can occur if it is impossible to perform a heart transplant.
Causes of ICMP development and risk factors
Cardiomyopathy occurs when the coronary arteries are damaged, most often of atherosclerotic origin. In this case, myocardial ischemia may in the first stages be accompanied by a weakening of the heart muscle, or this occurs against the background of frequent attacks of angina, especially unstable form, Prinzmetal.
Myocardial infarctions, in particular repeated, extensive, atypical ones, lead to the formation of this condition. In such cases, such an outcome is a protective mechanism for the survival of patients in vascular accidents.
Risk factors for ischemic cardiomyopathy include:
- complicated heredity;
- male gender;
- arterial hypertension;
- increased cholesterol levels in the blood;
- abuse of nicotine, alcohol or drugs;
- excess body weight;
- deposition of amyloid protein in the myocardium;
- kidney failure;
- diabetes.
For women, the risk of cardiomyopathy increases after menopause or taking contraceptive pills, as well as in the presence of one or more additional causes.
We recommend reading the article about dilated cardiomyopathy. From it you will learn about the forms of the disease and the reasons for its development, characteristic symptoms, diagnostics and treatment methods.
And here is more information about thyrotoxicosis and the heart.
“Falling asleep” of the myocardium in pathology
To describe the processes occurring in the heart muscle, the term hibernation (falling asleep) was proposed. This most fully reflects a reversible decline in function.
In this case, in proportion to the decrease in blood supply to the myocardium, its need for nutrients decreases.
This process prevents necrosis (infarction) from developing, the cells remain viable, and after the restoration of blood flow they self-heal.
In addition to the generating myocardium, the following processes develop in the heart muscle:
- decreased contractility of muscle fibers;
- stretching of ischemic areas in the systole phase;
- expansion of cavities;
- partial hypertrophy;
- fibrous (sclerotic) changes;
- apoptosis of cardiomyocytes – programmed breakdown into separate fragments.
Myocardial hypertrophy in cardiomyopathy
Symptoms of ischemic dilated cardiomyopathy
In the initial stages, signs of cardiomyopathy may be completely absent. The clinical picture of the disease corresponds to angina pectoris - attacks of pressing pain behind the sternum that occur after physical or emotional stress, and then at rest.
As myocardial damage spreads, its contractility weakens. This is especially true for the left ventricle. Therefore, at later stages, the signs of the disease do not differ from the characteristic manifestations of circulatory failure:
- labored breathing,
- accelerated pulse,
- swelling in the legs,
- congestive wheezing in the lungs,
- cough,
- increased weakness.
A distinctive feature of ischemic cardiomyopathy is the rapid progression of symptoms. Compared with dilated idiopathic cardiomyopathy, thromboembolism and arrhythmia are less common with myocardial ischemia.
Watch the video about cardiomyopathy and its consequences:
Diagnostic methods
When questioning the patient, it is imperative to determine whether there are risk factors for coronary artery disease, whether there have been angina attacks or a heart attack in the past. When examining, pay attention to swelling of the legs and an enlarged liver. Auscultation helps to identify wheezing over the lungs, rhythm disturbances, weakened first and additional third sounds, and accelerated pulse.
Due to the stretching of the cavity of the left ventricle, a murmur is heard during systole at the apex, the boundaries of the heart are expanded, mainly to the left.
Additional research data:
- ECG - overload of the left ventricle, the rhythm is often sinus, tachycardia, traces of a previous heart attack, diffuse changes in the T wave. Holter monitoring is used to detect hidden ischemia.
- Chest X-ray - the contour of the heart shadow is expanded, the aortic wall is dense, calcified, the arch is elongated and deployed in the ascending part, congestive processes in the lungs.
- Ultrasound with Doppler sonography - low cardiac output, dilation of the heart chambers, low motor activity of the left ventricle and increased rigidity of its walls.
- MRI and CT provide a layer-by-layer picture to determine the affected area.
- Myocardial biopsy is used for differential diagnosis in difficult cases.
- Scintigraphy with thallium radioisotopes is recommended in preparation for transplant surgery or revascularization (installation of a stent, shunt). Identifies small foci of reduced drug accumulation.
- Coronary angiography is prescribed to identify blocked arteries and signs of atherosclerosis.
- Blood tests with lipid profile and coagulogram are needed to determine further treatment.
Treatment of the patient
There is no specific treatment for cardiomyopathy, so symptomatic therapy and prevention of complications are carried out. The following tools are used for this:
- nitrates for attacks of heart pain - Cardiket, Monosan;
- non-selective adrenergic receptor blockers – Carvedilol;
- calcium antagonists – Corinfar, Diltiazem;
- diuretics – Veroshpiron, Lasix;
- cardiac glycosides - Strophanthin, Digoxin for tachycardia;
- antiarrhythmic - Cordarone;
- anticoagulants – Aspirin, Plavix;
- hypotensive - Hartil, Zocardis;
- hypolipidemic - Liprimar, Traykor;
- to strengthen the myocardium - Riboxin, Mildronate, Neoton, Coraxan.
In this case, it is necessary to follow a dietary diet with a limitation of table salt and liquid, animal fats and sugar, and flour products. Physical activity for each patient is calculated individually, it is necessary to avoid overwork and stress.
When indicated, heart surgery is performed:
- installation of a pacemaker (with or without a defibrillator);
- vascular bypass;
- balloon expansion with stenting;
- removal of atherosclerotic plaque;
- heart transplant.
Death as a real threat with ICMP
Often, the progression of heart failure cannot be stopped, despite complex therapy. This increases the risk of death from the following complications:
- pulmonary edema,
- cardiogenic shock,
- sudden cardiac arrest;
- recurrent myocardial infarction,
- ventricular fibrillation,
- pulmonary embolism.
Ventricular fibrillation as a complication of ischemic cardiomyopathy
Once diagnosed, only a third of patients have a 5-year chance of survival.
This is possible with complete cessation of bad habits, control of blood pressure, cholesterol and glucose levels in the blood, maintenance of normal body weight and adequate therapy.
With early treatment or after transplantation, the prognosis is more favorable. There are cases of 10-year survival after heart transplantation.
We recommend reading the article about restrictive cardiomyopathy. From it you will learn about the pathogenesis and forms of the disease, symptoms, methods of diagnosis and treatment.
And here is more information about the forms of atrial fibrillation.
Ischemic cardiomyopathy develops as a consequence of insufficient coronary blood flow. Some myocardial cells enter a dormant state, the strength of heart contractions decreases, and the cavities expand (especially the left ventricle). Progressive heart failure can be fatal if not treated sufficiently.
Symptomatic therapy is recommended; in many cases, a heart transplant is the only chance to save a life.
Source: //CardioBook.ru/ishemicheskaya-kardiomiopatiya/
Possible causes of pathology
The connection between cardiomyopathy and acute infarction with an area of more than 20% of the total heart mass, and repeated infarctions has been proven. Some authors consider the disease to be a consequence of improved survival of patients with acute coronary pathology and fairly good treatment.
In these cases, changes are confirmed by anamnestic data and ECG dynamics. Particular importance is attached to the painless form of heart attack.
The appearance of primary pathology without electrocardiographic abnormalities, but tending to ischemic causes due to clinical manifestations (angina attacks), remains unclear.
Provoking factors are considered:
- hypertension;
- disruption of the structure of blood lipoproteins towards an increase in the low-density fraction;
- unhealthy lifestyle with drinking alcohol, smoking, lack of exercise;
- thyroid diseases, diabetes mellitus;
- damaging effect of adrenal hormones, catecholamines;
- disturbances of central regulation under stress, increased nervous load;
- hereditary increased sensitivity and “vulnerability” of myocardial cells.
What is the pathology and its development associated with?
The progression of ischemic cardiomyopathy is associated with a previous myocardial infarction, especially when it recurs. In addition, the disease is a consequence of the formation of atherosclerotic plaques in the coronary arteries. Due to the accumulation of harmful substances, the lumen narrows and the blood circulation is disrupted. This leads to the following phenomena:
- ischemia;
- oxygen starvation of the myocardium;
- disruption of the contractile function of the heart muscle;
- destruction of myofibrils;
- excessive growth of muscle tissue;
- changes in the shape and size of the ventricles.
Among the provoking factors of the disease are the following:
- hypertension;
- unhealthy lifestyle: bad habits, limited physical activity;
- changes in blood composition with a predominance of low-density lipoproteins;
- dysfunction of the thyroid gland;
- progression of diabetes mellitus;
- negative impact of hormones produced by the adrenal glands, catecholamines;
- pathologies of the functioning of the central nervous system caused by emotional overload;
- a genetic factor that determines the sensitivity of cardiac muscle cells.
Characteristic symptoms
The clinical picture of ischemic cardiomyopathy necessarily includes 3 typical symptom complexes:
- 100% of patients have signs of congestive heart failure;
- in 50–70% of cases, characteristic symptoms of angina pectoris;
- from 20% to half of patients suffer from various thromboembolic complications.
The patient presents complaints characteristic of any heart disease
Mandatory addition are more or less pronounced signs of left ventricular failure:
- shortness of breath during physical and nervous stress;
- attacks of suffocation at night;
- increased fatigue, weakness;
- urinary retention, swelling in the feet and legs;
- weight gain.
The disease proceeds and develops at a slow pace. Some patients do not feel any disturbances and do not consult a doctor.
Among other manifestations, you can pay attention to the following:
- attacks of stable angina;
- moist cough;
- dull pain in the right hypochondrium;
- tachycardia and various forms of arrhythmia;
- loss of appetite.
Symptoms may occur intermittently and occur infrequently. Therefore, patients do not immediately consult a doctor, and necessary treatment is delayed.
Cough with sputum and moist rales in the lower parts of the lungs indicate heart failure
Symptoms of ischemic cardiomyopathies
For reference. Most often, the disease develops in men who have previously suffered a myocardial infarction . The disease also often develops in patients with angina pectoris, or after transluminal balloon angioplasty or coronary artery bypass grafting.
In patients with diabetes mellitus, symptoms of ischemic cardiomyopathy often develop against the background of silent myocardial ischemia.
Symptoms of the disease resemble those of idiopathic dilated cardiomyopathies. However, with ischemic cardiomyopathies, signs of severe heart failure progress much faster than with DCM (dilated cardiomyopathy).
When examining the patient, signs of cardiomegaly are revealed (usually due to the left half of the heart), increased heart rate, the appearance of arrhythmias (this symptom is observed less frequently in ICMP than in dilated ones), dullness of heart sounds, and protodiastolic galloping rhythms.
It is also possible for blood clots to appear in the ventricular cavity with the subsequent occurrence of thromboembolic complications.
Symptoms of CHF appear:
- fatigue,
- the appearance of shortness of breath symptoms not associated with physical activity,
- swelling,
- frequent dizziness,
- fainting,
- sensations of “interruptions” in the work of the heart, etc.
Attacks of angina pectoris may also occur, manifested by burning pain in the chest, shortness of breath, sometimes heartburn, profuse sweating, and nausea.
Diagnostic signs
A medical examination reveals:
- swelling in the feet and legs;
- liver enlargement;
- varying degrees of wheezing in the lungs during auscultation;
- accelerated and disturbed heart rhythm;
- expansion of the left border into the axillary region;
- systolic murmur at the apex, formed by relative mitral valve insufficiency with a distended left ventricle.
The ECG shows left ventricular overload; 80% of patients have correct sinus rhythm. Various types of arrhythmias:
- ventricular extrasystoles - rarely;
- atrial fibrillation is present in 15–20% of patients;
- disturbance of atrioventricular conduction - about 5%;
- bundle branch block - up to 15%;
- electrolyte changes in the myocardium.
X-ray confirms dilatation of the left ventricle
On a plain chest x-ray, patients are characterized by signs of aortic atherosclerosis:
- wall seal;
- expansion in diameter;
- ostial calcification;
- lengthening and reversal of the ascending part and arc.
An early sign of heart failure is a decrease in left ventricular ejection fraction. This indicator can be measured by magnetic resonance imaging, ultrasound and Doppler examination of the heart. Normally, the emission value approaches 55%. In patients it is significantly reduced.
A form of cardiomyopathy with a normal ejection level cannot be excluded; it is called heart failure with preserved ejection fraction.
Coronary angiography with contrast of the coronary vessels often reveals multiple thrombotic changes in the branches of the arteries. Less often, these changes do not correspond to the severity of the condition and the patient’s complaints. Such discrepancies support the involvement of vascular inflammation in the occurrence of cardiomyopathy.
Causes
The main reason for insufficient oxygen supply to the heart muscle is damage to the coronary arteries due to atherosclerosis. Hypoxia also progresses due to the fact that the muscular wall of the heart hypertrophies (increases). A more rare cause is myofibril contracture (prolonged excessive contraction of muscle fibers).
An important factor in the development of ICMP is an imbalance in the synthesis of substances produced by the endothelium (the inner lining of blood vessels). There is insufficient production of vasodilators (substances that dilate blood vessels) against the background of normal production of vasoconstrictors, resulting in additional vasoconstriction.
Dysmetabolic cardiomyopathy The ascending portion and arch of the aorta are also subject to atherosclerotic damage, which leads to its stretching, thickening and lengthening. At the same time, deposition of calcium salts may occur in the area of the aortic ring and its ascending section.
Features of choosing an examination method
Myocardial biopsy is performed in rare cases of differential diagnosis with a tumor. A special device is inserted through the catheter to collect tissue for analysis.
To prescribe optimal treatment, it is important to identify the reserve capabilities of the myocardium and the level of myocyte viability in unfavorable areas. This can be established through special studies with isotopes (thallium, fluorodeoxyglucose) that have an affinity for cardiac muscle tissue. The result serves as a prognostic test; a sharp decrease in viable cells indicates poor results of therapy. The method in determining treatment tactics has limitations and its own indications; it is necessary in the following situations:
You can also read: Fatty degeneration of the myocardium
- when selecting patients for heart transplantation and revascularization (restoration of blood supply);
- with proven ischemic disease, the absence of a large scar with a decrease in the ejection fraction to 35% or lower.
Cardiac surgeons consider it dangerous to use the technique in patients with a stable form of angina of the fourth functional class and an unstable form.
MRI for patients with fitted defibrillators or pacemakers is performed in the vascular mode. This eliminates the risk of unfavorable situations.
Treatment of the patient
There is no specific treatment for cardiomyopathy, so symptomatic therapy and prevention of complications are carried out. The following tools are used for this:
- nitrates for attacks of heart pain - Cardiket, Monosan;
- non-selective adrenergic receptor blockers – Carvedilol;
- calcium antagonists – Corinfar, Diltiazem;
- diuretics – Veroshpiron, Lasix;
- cardiac glycosides - Strophanthin, Digoxin for tachycardia;
- antiarrhythmic - Cordarone;
- anticoagulants – Aspirin, Plavix;
- hypotensive - Hartil, Zocardis;
- hypolipidemic - Liprimar, Traykor;
- to strengthen the myocardium - Riboxin, Mildronate, Neoton, Coraxan.
In this case, it is necessary to follow a dietary diet with a limitation of table salt and liquid, animal fats and sugar, and flour products. Physical activity for each patient is calculated individually, it is necessary to avoid overwork and stress.
When indicated, heart surgery is performed:
- installation of a pacemaker (with or without a defibrillator);
- vascular bypass;
- balloon expansion with stenting;
- removal of atherosclerotic plaque;
- heart transplant.
Differences from dilated cardiomyopathy
Differential diagnosis with dilated cardiomyopathy is mandatory.
General signs:
- enlarged heart;
- identification of areas of impaired myocardial contractility;
- the presence of scar changes in the heart muscle;
- increasing deficiency.
For the ischemic form of cardiopathy, the following are more typical:
- previous myocardial infarction;
- the presence of symptoms typical of angina pectoris;
- changes on the ECG, coronary angiography confirming stenosis of the coronary arteries, diffuse type cardiosclerosis.
Less common manifestations in the ischemic form are thrombosis and embolism as complications of the disease: detected in 40% of patients, and in the dilated version - in 60%.
Auxiliary signs in 35% of patients consist of anamnestic data. The “ischemic” type of cardiomyopathy is confirmed by the presence of risk factors.
Diagnostics
To clarify the diagnosis, the following is carried out:
- collection of anamnestic data,
- radiography of the OGK,
- Echo-KG,
- ECG,
- coronary angiography,
- scintigraphic examination,
- auscultation of the heart,
- palpation of the apex beat,
- percussion of the borders of the heart,
- general blood and urine tests,
- coagulogram,
- blood biochemistry, etc.
Treatment
Modern cardiology has made it possible to stop the destruction of myocardial cells in the early stages of the disease. The treatment package includes:
- a regime with limited physical activity, stress, and sufficient rest;
- nutrition according to the requirements of the anti-sclerotic diet;
- use of drugs from the group of β-blockers (Carvedilol);
- the use of diuretics such as Furosemide and Spironolactone;
- cardiac glycosides for tachycardia;
- if thrombosis is suspected or has a history, indirect anticoagulants are used.
Surgical methods To restore myocardial vascularization, a necessary condition is the preservation of a sufficient number of viable cells. A coronary artery bypass surgery is performed, followed by continuation of conservative treatment of angina pectoris and heart failure.
With pronounced scar changes, revascularization is considered inappropriate and even life-threatening for the patient. Selection operations can be:
- removal of a cardiac aneurysm;
- installation of a pacemaker;
- heart transplantation.
Drug treatment
For the treatment of ischemic cardiomyopathy I use:
- beta blockers - Atenolol, Bisoprolol;
- ACE inhibitors – Perindopril, Ramipril;
- sartans - Candesartan, Telmisartan (for intolerance to ACE inhibitors);
- aldosterone antagonists – Spironolactone;
- diuretics – Indapamide, Torasemide (for severe congestion);
- nitrates - Isosorbide Dinitrate (only in the presence of attacks of pain).
Doctor's advice: what medications should you take regularly and why?
In addition to the above medications, the patient in any case constantly needs to take the following medications:
- antiplatelet agents (acetylsalicylic acid) – prevent thrombosis, thereby reducing the risk of myocardial infarction;
- statins (Atorvastatin, Rosuvastatin) – drugs that lower blood cholesterol levels;
- anticoagulants (Warfarin, Dabigatran) - blood thinning drugs, they are necessary for the prevention of stroke in patients who have developed atrial fibrillation;
- hypoglycemic agents (Metformin, Glibenclamide) - if a biochemical blood test reveals a high level of glucose in the blood, I refer the patient to an endocrinologist to confirm diabetes mellitus, prescribe medications and a special diet;
Complications
Pathological changes in ischemic cardiomyopathy can lead to the following consequences:
- severe heart failure of the left and right ventricular type;
- intensification of ischemic processes;
- acute myocardial infarction;
- arrhythmias;
- lethal outcome.
Diagram of the dependence of treatment outcomes on the degree of myocyte viability
Causes of development of ischemic cardiomyopathy
For reference. Ischemic cardiomyopathies are most often caused by severe damage to the coronary vessels by atherosclerotic plaques.
Secondary ischemic cardiomyopathy can develop against the background of ischemic heart disease, myocardial infarction, severe endocrine pathologies
(decompensated forms of diabetes mellitus, thyroid pathology, adrenal dysfunction, etc.).
Predisposing factors contributing to the development of ischemic cardiomyopathies are the presence of the following in the patient:
- hypertension (especially with hypertensive crises);
- heart rhythm disturbances;
- alcoholism;
- physical inactivity;
- frequent stress;
- overwork, chronic sleep deficiency;
- family history of cardiovascular pathologies;
- autoimmune pathologies;
- hormonal disorders;
- severe lipid imbalance;
- blood clotting disorders, with a tendency to thrombosis;
- electrolyte imbalance;
- severe disorders of protein metabolism;
- cardiac aneurysms;
- toxic damage to the cardiovascular system, etc.
Forecast
The ischemic form of cardiomyopathy has a worse prognosis for the patient’s life compared to others. Reasons for this:
- severe, life-threatening arrhythmias;
- possible fatal complications;
- long and complex surgical interventions;
- use of various potent medications in therapy.
The mortality rate with conservative treatment of patients with established myocardial viability is 16%, and with the use of surgical methods - 3.2%. With non-viable myocardium, these figures are close to the same: from 6.2 to 7.7%.
Patients with symptoms of myocardial ischemia must undergo examination for early diagnosis of cardiomyopathy. Correct and timely therapy allows you to save and prolong the patient’s life.
Surgical methods of treatment
Ischemic cardiomyopathy in severe cases requires surgical intervention. These methods include:
- implantation of a pacemaker, which is carried out to normalize the heart rhythm;
- angioplasty, designed to dilate affected vessels;
- stents are special tubes that keep arteries open;
- atherectomy - this method of surgical intervention allows you to remove plaque from the venous walls;
- Radiation therapy is used to keep the arteries clear after angioplasty.
In some cases, coronary artery bypass grafting is used. This method is carried out to improve blood flow to the heart muscle. To do this, a previously removed vein is placed near the affected artery. This is necessary so that the blood moves through the new vessel, bypassing the affected one.
If we are talking about too large a lesion, then the only method to save the patient’s life is a heart transplant.
Approaches to the treatment of ischemic cardiomyopathy
The basis of therapy is taking medications. Surgical intervention is performed only in exceptional cases, as it poses a threat to the patient's life.
Drug treatment
Patients will be prescribed medications such as:
- antiarrhythmic drugs (Digoxin);
- beta-blockers (Metaprolol, Carvedilol);
- ACE inhibitors (Capoten);
- diuretics (Lasix);
- anticoagulants (acetylsalicylic acid).
Recommendations for correcting the regime
In parallel with taking special medications, the patient must comply with the following rules:
- limit to a minimum the amount of fat and salt consumed;
- refuse increased physical activity;
- avoid stress and emotional tension;
- leave enough time for proper rest;
- to refuse from bad habits.
Methods of surgical treatment
Surgery for ischemic cardiomyopathy is indicated only if conservative methods of therapy have failed.
The following methods of surgical treatment of pathology are distinguished:
- Pacemaker implantation. An implantable device is necessary when detecting heart failure. Thanks to the pacemaker, the heart rhythm is normalized. The device also reduces the risk of sudden death caused by ischemic cardiomyopathy.
- Implantation of a cardioverter-defibrillator. This measure is required for ventricular arrhythmia, a condition that threatens the patient’s life. The device monitors the rhythm of the heart muscle.
- Coronary bypass surgery. During the operation, another, previously removed, vessel is inserted next to the blocked artery. It is through it that the blood flow is directed. This event stimulates blood flow to the heart muscle.
- Angioplasty is an operation to widen the arteries to improve their patency.
- Installation of stents to expand the lumen of blood vessels.
- Atherectomy is a manipulation aimed at cleansing the walls of the arteries from plaques and plaque that impede the flow of blood.
- In the most severe cases, the patient requires a heart transplant.
Nutritional Features
People suffering from ischemic cardiomyopathy are recommended to include the following foods and drinks in their diet:
- baked goods without salt;
- low-fat dairy products;
- vegetables processed in various ways;
- seafood;
- lean fish;
- cereals;
- pasta from durum wheat;
- vegetable soups;
- berries and fruits, fresh or dry;
- honey;
- vegetable oils;
- green leaf tea;
- fresh juices.
You should not consume the following foods and drinks that negatively affect the condition of the heart muscle:
- meat and fish of fatty varieties;
- confectionery;
- salty and spicy dishes;
- fatty broths;
- canned food;
- smoked meats;
- onion garlic;
- semi-finished products;
- strong coffee and tea;
- alcohol.
Folk remedies
The point of using folk recipes for ischemic cardiomyopathy is to alleviate the patient’s condition. Such therapies cannot cure the disease and should under no circumstances be the basis of therapy.
The following recipes are useful:
- Viburnum berry tincture. To prepare, you need to take 40 g of raw materials (the berries must be ripe), pour a glass of hot water. Let the liquid brew for 2 hours, then strain. The resulting volume is the daily dose of the medicine. You need to drink it 2 times during the day.
- A decoction based on motherwort. You should take 15 g of raw material and fill it with 0.5 liters of hot water. The product must be infused for 7 hours. After this, the liquid must be filtered. Take the prepared infusion throughout the day. The norm is a glass of decoction, the volume of which should be divided into 4 doses.
- Herbal collection. It is necessary to prepare 2 tablespoons of nettle leaves and a tablespoon of motherwort, mix the ingredients, pour 250 liters of boiling water. Infuse the product for an hour, then strain. Take half a glass twice a day.
- Infusion of flax seeds. To prepare the product, you need to pour 4 teaspoons of flax seed into a liter of water. Place the mixture on the stove and let it boil. The product should be infused in a water bath for an hour. After this, the broth must be filtered. Take the finished product warm, half a glass, up to 5 times a day.
During the treatment process, the doctor regularly monitors the most important indicators: heart rate, pulse rhythm, and the patient’s blood pressure level.