The aorta is the largest vessel. Through it, blood flows from the left ventricle of the heart to the organs and limbs. And if coarctation (narrowing, stenosis) of the aorta occurs, it affects the entire blood circulation. And, accordingly, on organs and tissues. This is usually a congenital anomaly. It leads to serious and dangerous complications. To prolong the patient's life and improve the prognosis, surgical intervention is needed.
The main treatment method for coarctation of the aorta is surgery.
General information
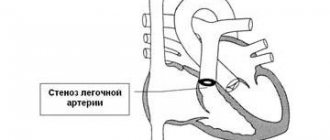
The pathology is listed in ICD 10. This is the abbreviated name for the International Classification of Diseases. Each disease is assigned a number, which makes it easier to find information about the disease. Coarctation of the aorta is found in the section “Congenital anomalies of the large arteries.” Its number is Q 25.1. The disease develops while the baby is in the womb. But pathology can be detected in both infants and adults. With stenosis, the vessel narrows. Usually at the point of bending - where the aorta “turns” down from the left ventricle of the heart (aortic isthmus). Less often - in the chest or abdominal area. Due to pathology, less blood passes through the vessel. If left untreated, it can be fatal.
When coarctation of the aorta occurs, problems arise:
- The difference in pressure above and below the narrowing. At the top it is high, at the bottom it is low.
- The left ventricle becomes greatly stretched and hypertrophied as the heart has difficulty pushing blood through the aorta.
- The heart is under a lot of stress.
- Little blood flows to the lower extremities. Because of this, they develop worse.
- Due to blood pressure, the arteries dilate and increase in diameter.
- The aorta develops lateral vascular branches. They also grow near the intercostal vessels, thoracic and left subclavian arteries.
Without surgical treatment, coarctation of the aorta is often fatal. 55–65% of newborns die from this disease. Even if the body has “adapted” to improper blood circulation, after a while patients may experience serious problems:
- blood clots;
- heart failure;
- atherosclerosis of arteries;
- angina pectoris;
- aneurysms (dilation) of blood vessels;
- thromboembolism;
- cardiac asthma;
- intracerebral hemorrhages;
- arterial hypertension;
- pulmonary edema;
- myocardial infarction;
- stroke;
- septic endocarditis;
- problems with blood circulation negatively affect all organs: the patient may develop ischemia of the brain, heart, kidneys, and intestines.
Many of these diseases are life-threatening. Without treatment, the patient may die from ruptured aneurysms. It is not possible to completely get rid of the pathology. There is a risk that even after surgery the patient will have problems associated with cardiovascular failure. But surgery is needed to prolong the patient’s life and improve its quality.
How does blood flow change during coarctation of the aorta?
The free flow of blood will be impaired due to the presence of resistance along the path. Above the stenosis, pressure increases; accordingly, arterial hypertension develops in the vessels of the upper half of the body (“the head, neck, chest, and upper limbs suffer” in this case). These changes develop due to an obstruction of normal blood flow in the area of stenosis and are associated with factors such as increased heart function, increased contraction rhythm, increased blood ejection from the heart; as the changes progress, other mechanisms may be activated (activation of neurohumoral systems).
Below the stenosis, on the contrary, there is a decrease in blood pressure, since the outflow of blood from the stenotic area decreases. In this case, the lower part of the body “suffers” (namely, the vessels that supply blood to the internal organs and lower limbs). Due to the fact that a smaller than normal amount of blood enters the vessels located below the stenosis, anastomoses or bypass blood flow paths (intercostal arteries, arteries of the chest wall, hypogastric arteries) develop compensatoryly. These bypass pathways allow blood to circulate from the heart to areas of the body below the stenosis.
Below the narrowed area, the so-called turbulent blood flow (“vortex”) develops, which, due to increased pressure on the vessel, causes thinning and expansion of the aortic wall in this area.
As the load on the left ventricle increases, due to the constant obstruction of blood flow, it becomes overloaded and thickens. This ultimately ends in the development of heart failure.
Symptoms
Coarctation of the aorta has the following symptoms:
- headache, migraine;
- weakness (sometimes increasing), increased fatigue;
- dizziness;
- "noise in ears;
- pale skin;
- cramps in the limbs;
- cold feet - feet often freeze;
- chest and abdominal pain;
- fainting;
- numbness of the limbs;
- pain in the calf muscles;
- lameness;
- heaviness in the head;
- feeling that the heart is not working “right”: interruptions in heartbeat, rapid rhythm;
- shortness of breath, cough;
- high blood pressure appears even with moderate physical activity;
- memory impairment, fatigue;
- deterioration of vision and hearing;
- nosebleeds;
- The upper half of the body (chest, arms, shoulders, head) develops better and faster than the lower half (pelvis, legs).
Signs of aortic coarctation vary depending on the stage and classification of the pathology, the age and gender of the patient, and concomitant diseases. For example, in children 5–14 years old, only weakness, shortness of breath and headaches are observed. But in adolescence, heart failure develops. She has more pronounced symptoms: nosebleeds, fainting, arrhythmia, skin numbness, lameness. Some of the symptoms described are also characteristic of other ailments. A complete examination is required to make a diagnosis.
Examination and diagnosis
Pathologies in the development of the aorta in the fetus are usually visible even before birth. Their signs are noticed during an ultrasound of the expectant mother and listening to the baby’s heart. After the baby is born, an examination is also carried out. General diagnostics (for both children and adults) reveals concomitant diseases, pathologies, and heart defects. It includes:
- Patient interview. This is how the doctor determines what symptoms bother the patient. If the patient is too young to answer questions, the conversation is carried out with his mother.
- Analysis of the patient’s life and general condition. They look at how much he weighed at birth and whether he developed normally compared to his peers.
- They ask whether any of your relatives have had heart or cardiovascular disease. And also whether there were cases of child mortality in the family. This is necessary to determine whether there is a genetic predisposition.
- Inspection. Feel the feet. In patients they are cold. They listen to the heart. Assess skin condition, physique, weight. They feel the pulse (with narrowing of the aorta, it is very weak on the legs and at the same time good on the arms).
- Urine and blood analysis. This is necessary to identify concomitant diseases and pathologies.
- Electrocardiography. It is used to determine whether there is thickening of the walls of the ventricles.
- HMEKG. "Daily" cardiogram. It is recorded over 1–3 days using a device that must be carried with you. Such diagnostics are needed to identify rhythm disturbances.
- Radiography. The size of the heart and the condition of the lungs are assessed.
- MRI (Magnetic resonance imaging). A contrast agent is used to “illuminate” organs and blood vessels. It is administered intravenously. And then they do a CT scan. You can get detailed and three-dimensional images. This is how they find out the size of the aorta and see if the diameters of the vessel above and below the stenosis differ. Determine whether there are aneurysms. MRI scans other organs to identify concomitant diseases and pathologies.
- Ultrasound. Ultrasound examinations evaluate the size of the heart, check whether the chambers are dilated, and determine where the pathology is located.
- Echocardiography. After this examination, a diagnosis of “coarctation of the aorta” is made. Using echocardiography, the size of the aorta and narrowing are determined.
- Catheterization and aortography. A flexible tube is inserted into the femoral artery. It can be “brought” to the heart valve. The contrast agent flows through it. It is harmless to the body. It simply “highlights” organs and blood vessels. So that they are clearly visible during aortography. This is an accurate and effective method. With its help, you can determine where the narrowing is, how large it is, whether it affects the size of the aorta, and whether collaterals (lateral circulatory pathways) have appeared because of it.
- Probing of the heart chambers. A catheter is inserted, to which a camera is attached.
- Consultation with a cardiac surgeon.
Based on the results of the examination, treatment is prescribed. There are several types of operations. Each of them is suitable for a specific type of aortic coarctation. Therefore, diagnostics are needed.
Causes
Typically, such pathologies appear when the child is in the womb. There are disturbances in the development of the fetus. Causes:
- When the embryo is still forming, a duct connects the aorta to the pulmonary artery. In newborns, it closes quickly as soon as the baby begins to breathe. But due to improper development, duct tissue can move onto the vessel. It will close and “drag” part of the aortic wall behind it.
- Pathologies of the interventricular septum.
- During the formation of the fetus, the aortic arches were not connected correctly.
- There are falciform ligaments of the aorta.
- Violation of intrauterine circulation.
Pathologies in the development of the embryo can arise due to genetic predisposition, heredity, and mutations.
Risk factors also include what happens to the expectant mother:
- Viral or infectious diseases in the first trimester.
- Taking certain medications. It is especially dangerous to take medications that are not approved by a doctor in the early stages of pregnancy. Be sure to look at the contraindications. And consult your doctor before choosing medications.
- Environmental influence. This is not only bad ecology. For example, you should not work with harmful substances: varnishes, paints.
- Diseases of the pelvic organs.
- Diabetes.
- There were abortions.
- The expectant mother has bad habits: alcohol, smoking.
- Coffee.
- Late pregnancy, the woman giving birth is over 35 years old.
These factors increase the risk of developing various pathologies in the fetus. Not just stenosis. This does not mean that if a woman becomes pregnant at 40, she will necessarily have a sick child. If you eat right, lead a healthy lifestyle, don’t get nervous, keep your body in good shape, undergo examinations, regularly visit your doctor and listen to his recommendations, then it’s unlikely that anything bad will happen. But bad habits of the mother can harm the baby.
Sometimes coarctation of the aorta appears in adults. Moreover, the pathology is not congenital. Such anomalies develop for other reasons:
- chest injuries;
- vascular injuries;
- atherosclerotic vascular damage, atherosclerosis: plaques narrow the aortic lumen;
- Takayasu's disease, inflammation of the aorta.
Why and how it develops
The aorta is formed incorrectly during intrauterine development:
- if there is a genetic predisposition to the problem;
- if women have suffered viral or bacterial diseases;
- if the expectant mother smokes, drinks alcohol and drugs during pregnancy;
- as a result of living in unfavorable environmental conditions;
- if a woman has been in contact with toxic substances.
The process of coarctation formation occurs in the tenth week of embryonic development. Negative factors contribute to the fact that tissues in the ductus arteriosus attach the aorta to the left pulmonary artery. Immediately after birth, the lungs begin to participate in breathing and the duct must close. During its closure, the aorta stretches and becomes like an hourglass. The damaged area may vary in size. At the site of narrowing, additional vessels begin to form, which are called collaterals. They appear to maintain blood circulation at the required level.
Classification
The clinical picture may vary depending on the type of pathology. There is a classification based on the patient’s age (adult, child), location of the stenosis, its shape, anatomical features, stages of development, and concomitant diseases. The doctor will find out these details after diagnosis. An ultrasound of the heart alone is not enough. A detailed examination is needed (EchoCG, MRI, aortography, cardiogram, electrocardiogram, catheterization, tests). The treatment regimen, type of surgery and prognosis depend on the results.
According to their shape and anatomical features they are distinguished:
- isolated coarctation (there are no other diseases of the heart and blood vessels, only this anomaly was found);
- narrowing of the aorta is accompanied by damage to the interventricular septum;
- stenosis and patent ductus arteriosus;
- there are other heart defects and vascular pathologies.
By location and course of action:
- Typical. At the site of the bend of the aorta.
- Atypical. In the abdominal or chest area.
According to the age:
- Children's. The blood flows through the arterial duct, which has not yet closed. Blood circulation is practically no different from uterine circulation.
- Adult. The body adapts. Additional vessels develop through which blood flows to the stenosis.
Prevention
If the heart defect is not congenital, then a number of measures can be taken to avoid the occurrence of aortic stenosis. Avoid the severe consequences of sore throat (rheumatism), treat it promptly and completely, and prevent diseases such as atherosclerosis and infective endocarditis. If you have an existing disease, reduce the load on your heart.
For prevention, folk remedies are used, for example, hawthorn in the form of jam (add it to a glass of water and drink it on an empty stomach).
Age
- Critical - up to a year. For infants with this pathology, the first year of life is the most dangerous period. Children of this age have a high mortality rate - 55 - 65%. Coarctation of the aorta in newborns is accompanied by severe heart failure. The kidneys and lungs suffer from this.
- Adaptation – 1 – 5 years. The symptoms are not that pronounced. The body “gets used” to abnormal blood circulation.
- Compensatory – 6 – 14 years. The disease practically does not manifest itself. Only fatigue, dizziness, and migraine are noticeable.
- Relative decompensation – 15 – 20 years. Heart failure develops again. Oxygen starvation of organs begins.
- Complete decompensation - 21 - 30 years. Serious complications may occur: heart attack, stroke, aneurysms, hemorrhages, acute hypertension, hypertension. Risk of death.
Critical moments can arise during any of these periods. Even if symptoms do not appear, this does not mean that the danger has passed.
Treatment
The main thing is not to overload the body. Neither before nor after treatment. No physical activity, stress, bad habits (alcohol, smoking, coffee). Even junk food can make the condition worse. There are no medications that can “cope” with this disease. Only surgery (if there are no contraindications) and constant monitoring by a cardiac surgeon will help. Other treatment measures will not be effective. Medicines are needed to relieve the symptoms of hypertension. Medicines are used to reduce the risk of developing an infection. They also improve the condition of brain tissue, kidneys and myocardium, which are weakened by oxygen starvation.
Treatment for coarctation of the aorta is usually prescribed between the ages of 1 and 5 years, unless there are complications. First, tests are taken, ultrasound and magnetic resonance examinations, catheterization, aortography are performed, and a cardiogram is recorded. It's a long process. If the case is critical, the operation can be performed on infants up to one year old. You should not delay your visit to the doctor. The older the patient, the worse the postoperative prognosis. If you do not start treatment before age 10, it will be too late.
Types of procedures:
- Balloon dilatation. Suitable if the stenosis is minor. Or the previously operated vessel has narrowed again. A balloon is inserted into the aorta and inflated. Thus, the walls stretch. The vessel can be fixed using stents - they set the desired size of the aorta.
- Aortoplasty. For restoration, material is taken from the subclavian artery.
- Plastic reconstruction. The aorta is cut and stitched without stenosis. Suitable if the narrowing is of small extent and the ends of the vessel can be connected.
- Vascular prosthesis. The stenosis is completely removed, and a “prosthesis” made of synthetic material is placed in its place.
- Bypass surgery. A synthetic vessel is “added” to the aorta, the ends of which are attached above and below the coarctation. This creates a bypass for blood flow.
Possible complications
With coarctation of the aorta, complications are caused by the following disorders:
- arterial hypertension;
- changes in the aorta and emerging collaterals;
- development of bacterial or infectious-allergic inflammatory processes.
Such complications include the following pathologies:
- pulmonary edema;
- acute cerebrovascular accidents;
- hemorrhages in the spinal cord and brain, leading to paresis and paralysis;
- hypertonic disease;
- cardiac asthma;
- renal failure;
- heart failure;
- aortic aneurysm and its rupture;
- aneurysms of intercostal arteries;
- bacterial endocarditis;
- endoaortitis;
- calcification of the aortic walls;
- endomyocarditis.
The complications of aortic coarctation described above can lead to the death of a child at any age.
Forecast and recommendations
Without surgical intervention, the life expectancy of patients rarely reaches 20–35 years. The risk of death in infancy is high. Although this depends on the stenosis - if the narrowing is minor, then it is not so dangerous. Treatment is complex and long. But it gives positive results in 95% of cases. The prognosis depends on the classification of the disease, the patient's age and other related factors. Ideally, the patient’s life can be extended to 40–50 years. But at the same time you will have to monitor your health, tone, and take medications.
Any physical activity or stress should be avoided. Get hooked on proper nutrition. And, most importantly, constantly see a doctor and undergo regular examinations . There is always a risk of re-stenosis and the development of heart failure.
During the rehabilitation period, some symptoms will still appear. For example, high blood pressure, weakness, dizziness. Doctors will prescribe medications that will make you feel better. It will be possible to find out something specific after surgery and rehabilitation. The doctor will do a re-diagnosis and tell you if there are any results. He will also give detailed recommendations that you must follow.
Coarctation of the aorta in children and adults occurs for various reasons. Usually this is a congenital pathology - it appears at the stage of fetal formation. But due to injuries and inflammation of blood vessels, it can develop in adulthood. This is a very dangerous disease that cannot be cured with pills. Only surgery will help. Without surgery there is a risk of death.