photo: independent.co.uk
Facing certain death, doctors were forced to perform a life-saving transplant when she was two years old. But instead of removing the diseased heart entirely, they grafted the donor heart onto her own, allowing the weaker organ to rest and heal inside her body. Life became a constant struggle as Hannah's immune system slowly began to reject her transplant.
In her first public appearance, the healthy 16-year-old girl from South Wales spoke of her delight at having her original heart returned after becoming the first person in Britain to have a transplant of this kind.
“It was really weird, I felt empty,” Hannah said of the moment she woke up from her breakthrough surgery and realized her real heart was pumping fully for the first time in a decade.
“The second heart was inside me for so long, but suddenly it disappeared. I felt like something was missing in my chest. But I was so happy."
In February 2006, surgery was performed again at Great Ormond Street Hospital to give Hannah the use of her heart.
Classification of heart diseases
The heart is a vital organ, so any disturbances related to its structure or functioning lead to severe disturbances throughout the body. Today, a number of organic heart diseases are known, which most often lead to tissue destruction and in some cases cause the death of the patient.
Conditional classification of organic heart diseases
- Coronary heart disease - includes sudden coronary death, angina (unstable and tension), myocardial infarction.
- Heart defects (congenital and acquired).
- Inflammatory diseases of the myocardium, endocardium and pericardium.
- Rheumatic heart disease.
Determining the type of pathology allows us to establish the cause of its development. In the future, it is possible to carry out effective treatment, which will ultimately improve the patient’s quality of life, and in some cases save his death.
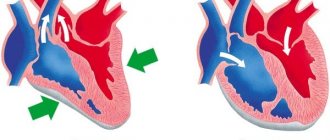
Unique operations
Surgeries in which doctors leave a patient's heart in place and transplant another into the right side of the chest are rare.
One of them was held in London in 1996. The famous heart surgeon Magdi Yacoub performed a heart transplant on two-year-old Hannah Clarke.
Cardiac ischemia
The pathology is based on a disorder of blood circulation in the coronary vessels that supply the heart muscle (myocardium). The pathology develops against the background of atherosclerosis of the vascular wall, due to which the blood flow through the vessel partially or completely stops. Also, the cause of coronary heart disease (CHD) can be thrombosis of the coronary vessels, which also causes the development of a clinical picture of acute or chronic circulatory disorders.
The most dangerous are acute forms of coronary artery disease, manifested by unstable angina, myocardial infarction and acute coronary syndrome. The latter disease causes sudden death. Additionally, chronic forms of IHD are distinguished, which are characterized by a pronounced clinical picture. In particular, this includes cardiosclerosis, stable angina and asymptomatic myocardial ischemia.
In what cases is there a risk of developing IHD?
- With poor nutrition, when high-calorie and fatty foods are consumed in large quantities.
- If preference is given to a sedentary lifestyle, or work involves prolonged periods of sitting.
- In case of frequent consumption of alcoholic beverages and other bad habits, especially smoking.
- When lipid metabolism disorders develop, often expressed in metabolic syndrome, hypothyroidism, obesity, diabetes mellitus.
- Upon reaching a certain age (in older people, IHD develops more often), although recently, due to frequent stress, IHD is often detected in people of working age.
- Emotional lability and a tendency to depression can also cause coronary circulation problems.
A pronounced clinical picture of IHD includes a number of characteristic symptoms: burning chest pain, pain in the area of the scapula or along the left arm. Such an attack, depending on the form of coronary artery disease, can last from several minutes to half an hour. The appearance of pain indicates a lack of oxygen in some part of the myocardium, therefore, if ischemia is not treated, a heart attack develops, with all its aggravating consequences.
Results and discussion
In a postmortem examination of the corpses of children who died from SIDS, the most consistent signs were hypotrophy, congestion of internal organs, thymomegaly, hyperplasia of lymphoid tissue (peribronchial and in the intestinal mucosa), hypoplasia of the adrenal cortex, and hypertrophy of the right ventricular myocardium. Most of these signs are not specific and indicate acute hypoxia of vital organs or an unfavorable background state of the neuroimmunoendocrine system responsible for the reactivity of the body.
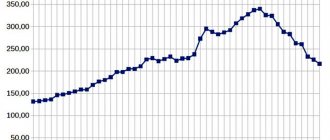
When studying the circulatory organs, we drew attention to some features of the heart, associated not only with the actual increase in its mass and hypertrophy of cardiomyocytes, but also with discoordination of the growth and development of the parts of the heart. Thus, when studying the dynamics of the cardiac index with age, it was noted that in SIDS its values practically did not change (Fig. 1).
Figure 1. Dynamics of the cardiac index during the first year of life in sudden infant death syndrome. This reflects an imbalance between the relative rate of body weight growth and the faster, spasmodic growth of heart weight, which, in our opinion, may create a favorable background for the implementation of cardiac mechanisms in SIDS.
Microscopic examination of histological sections of the myocardium in most cases revealed not only hypertrophy of ventricular cardiomyocytes in the subendocardial layer (Fig. 2a),
Figure 2. Pathological changes in sudden infant death syndrome.
a — hypertrophy of cardiomyocytes and their nuclei in the subendocardial layer of the myocardium of the right ventricle (d., 5 months 5 days). Hematoxylin and eosin staining. ×700. but also fibrosis of the endocardium and myocardial stroma (see Fig. 2, b, c).
Figure 2. Pathological changes in sudden infant death syndrome. b — fibrosis of the endocardium and subendocardial zone of the left atrium (m., 1 month 18 days). Van Gieson picrofuchsin staining. ×150.
Figure 2. Pathological changes in sudden infant death syndrome.
c — fibrosis of the right atrium stroma (m., 9 months). Van Gieson picrofuchsin staining. ×300. The nerve ganglia were located in a disorderly manner; attention was drawn to the difference in the size of the ganglia within the interatrial septum (see Fig. 2, d).
Figure 2. Pathological changes in sudden infant death syndrome.
d — interatrial septum in the area where the oval window is located. Nervous ganglion, some cells lack nuclei. Nissl staining. ×600. Some ganglion cells had dystrophic changes and necrobiosis. Near the ganglia, as a rule, nerve fibers in a state of edema were located (see Fig. 2, e).
Figure 2. Pathological changes in sudden infant death syndrome. d — interatrial septum in the area where the oval window is located. Nervous ganglion, some cells lack nuclei. Nissl staining. ×600.
Macroscopic examination of the heart with high consistency in the corpses of children in the first 3 months of life with SIDS revealed ectasia of the oval window and an increase in the size of both ventricles of the heart. The heart mass in its absolute values corresponded to the age norm. Considering that most researchers, when separately weighing the chambers of the heart, noted hypertrophy of the right ventricle of the heart in SIDS [8, 9] and the fact that in most observations we noted an increase in the size of both ventricles when weighing separately, it was of interest to compare the mass of the ventricles with the mass of the heart in dynamics. Quantitative characteristics of the mass of the right and left ventricles of the heart with the determination of the indices of the right and left ventricles made it possible to clarify through which parts of the heart and in what sequence the increase in heart mass is ensured.
In children who died from SIDS, a significantly higher mass of the right and left ventricles was obtained compared with the age norm. However, the dynamic increase in the mass of the heart chambers was characterized by unevenness in different age periods of the first year of life. During the first 3 months of life, the increase occurred due to both ventricles with the leading role of the right ventricle, in the subsequent months of life - mainly due to the left ventricle. In the control group, the increase in heart mass during the first year of life occurs evenly due to both ventricles.
Thus, we have identified significant features of cardiomorphogenesis in SIDS during the first year of life: an imbalance between body growth and heart growth, expressed in an accelerated increase in heart mass, as well as discoordination in the increase in mass of the right and left ventricles of the heart. In this aspect, our results differ from the literature data on an increase in the mass of only the right ventricle during the death of a child from SIDS [2].
Mathematical processing of the research results confirmed the reliability of our data. A correlation analysis carried out to establish the nature of the relationship between the increase in heart mass and the mass of individual ventricles allowed us to establish the different nature of the relationship between these phenomena.
The increase in heart mass in children who died from SIDS occurred only during the first 3 months of life due to both ventricles, which is confirmed by a stable correlation between the mass of the heart and the mass of both ventricles of the heart (|r|>0.8).
In this situation, it is necessary to find out what happens in the right and left ventricles of the heart during the syndrome from the point of view of structural transformations, due to which structures the mass of the ventricles increases normally and in SIDS, and whether these changes can be designated as hypertrophy. Therefore, we conducted a morphological and morphometric study of histological sections of the myocardium and a study of the structural features of isolated cardiomyocytes over time during the first year of life of children who died at home (see Fig. 2, f).
Figure 2. Pathomorphological changes in sudden infant death syndrome. e - isolated working cardiomyocyte of the right ventricle (m., 1 month 16 days).
In the interatrial septum, at the location of the oval window, during a morphometric study, a pronounced predominance of the percentage of connective tissue area in relation to muscle tissue was observed.
In the ventricles, the area of isolated cardiomyocytes of children who died from SIDS was significantly lower than in children of the control group (Fig. 3),
Figure 3. Diagram of average statistical indicators of the area of isolated cardiomyocytes of different parts of the heart by the end of the first year of life. The linear parameters of cells and their nuclei changed towards shortening the length and increasing the diameter, and the number of nuclei per unit area increased. As expected, the average area of the stroma in the myocardium increased, since during a light-optical study of histological preparations, signs such as endocardial fibrosis, especially in the atria, and a large amount of stroma of the ventricular myocardium attracted attention.
At the same time, significant differences were noted in the dynamics of parenchymal-stromal relationships on the part of the right and left ventricles of the heart in children who died from SIDS.
In the myocardium of the right ventricle of the heart, a significant dynamic increase in the area of the parenchyma was noted with a simultaneous decrease in the myocardial stroma. Since the area of individual myocytes increased slightly, and the number of nuclei per unit area dynamically increased, we can assume that the increase in the mass of the right ventricle is due to true myocardial hypertrophy and an increase in the number of myocardial cells, i.e. the possibility of dividing them.
In the myocardium of the left ventricle, the area of the parenchyma significantly decreased, while the area of the stroma increased noticeably. Since the planimetric and linear dimensions of cardiomyocytes decreased with an increase in the number of nuclei per unit area, we can conclude that the increase in the mass of the left ventricle in SIDS was associated mainly with an increase in the volume of stromal structures, and cardiomyocytes, while retaining the ability to divide into a state of hypertrophy, did not entered.
Myocardial infarction
The pathogenesis of the disease is closely related to atherosclerosis, as a result of which myocardial infarction goes through three stages in its development:
- The initial destruction of the inner wall of the vessel due to the presence of an atherosclerotic plaque, which remained in the vessel for a long time and affected its inner wall with fragments and various active components.
- The formation of a blood clot in vessels affected by atherosclerosis due to the destruction of the endothelial layer and further attachment of platelets and other blood cells to the affected areas.
- The thrombus blocks the lumen of the vessel, additionally the coronary arteries spasm, as a result of which the area of the myocardium supplied by this vessel is deprived of oxygen and tissue necrosis (death) occurs.
In most cases, myocardial infarction develops in a typical (anginal) form, when severe pain occurs in the heart area, radiating to the left arm, lower jaw, and left shoulder blade. The painful sensations continue for a long time, about half an hour or more.
It is important to remember that nitroglycerin does not help with myocardial infarction, so it is recommended to take this medicine before providing medical assistance in order to slightly improve the patient’s condition.
Myocardial infarction can develop in other, atypical, forms - asthmatic, arrhythmic, abdominal, cerebrovascular, asymptomatic. In any case, you must immediately call an ambulance and transfer the patient to doctors for further resuscitation.
In addition to the extra leg
In 1905, a 35-year-old American carpenter named Durr placed an advertisement in newspapers saying that he was ready to bequeath his body with two hearts to anyone who would pay a lot of money. He was examined by several experts, and the conclusions were unanimous - Durr really has two hearts, and the carpenter is absolutely healthy. A group of doctors offered him $10,000 to perform an operation to remove one of his hearts while he was alive. But the unique man wisely refused, fearing the consequences of surgical intervention.
In 1844, George Aippert, the famous man with three legs, was born in Germany. He worked in the circus of the largest American hoaxer Phineas Taylor Barnum, where they showed many unusual people (for example, the Russian boy Fyodor Evtishchev, who was born with a hairy face reminiscent of a dog's muzzle). Only in 1906, when George Lippert died, an autopsy showed that there were two hearts in his chest - neither he himself nor those around him even knew about it.
There is evidence of the existence of such a person in pre-revolutionary Russia - in 1911, a reference book on surgery was published in Yekaterinburg, which reported on the rural paramedic Vladimir Ognivtsev, who had two hearts, and even provided a diagram of the movement of blood in his body.
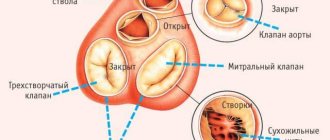
Heart defects
May be congenital or acquired. The first type of heart defects is more common in children, when at birth the newborn shows signs of impaired development of the heart and blood vessels (pallor or, conversely, cyanosis, poor sucking, frequent cries, shortness of breath, etc.).
The main forms of congenital heart defects:
- Ventricular septal defect.
- Atrial septal defect.
- Patent ductus arteriosus.
- Pulmonary artery stenosis.
- Coarctation of the aorta.
- Aortic stenosis.
In most cases, congenital defects require defect plastic surgery or angioplasty. Only sometimes, and even then not all defects, can be independently resolved and eliminated when the child reaches a certain age. If, on the contrary, everything was fine with the child, and then symptoms of the disease began to appear during physical activity, you should immediately contact a cardiologist so that a decision can be made on the optimal treatment method.
Amazing Brothers
A unique case occurred in Irkutsk. Elvira Chernikova, who was looking for her cousin, told about him through newspapers. The boy was born to her aunt Valentina Dedyukhina in 1937. The doctor who examined him persuaded the woman to abandon the child because he had two hearts, and the doctor assured the mother that the baby with such a pathology simply would not survive. Valentina Dedyukhina signed the refusal, but literally a few months later she regretted it and began to look for her son. It turned out that the boy disappeared along with the same gynecologist who allegedly adopted him. The time was difficult, and the mother, who had formalized the abandonment of her son, did not contact law enforcement agencies.
A few years later, Valentina Dedyukhina’s sister also had a son with two hearts! Elvira Chernikova says that now, although he is quite elderly, he is a healthy man, and both hearts are working properly. Now she is trying to find that cousin who disappeared in 1937.
This story gives reason to assume that the phenomenon of two hearts may have some connection with genes - after all, the birth of human phenomena occurred among sisters.