Marmara operation for varicocele
Periodically occurring nagging pain in the scrotum and obvious asymmetry of the testicles may indicate the development of varicocele - a pathological dilation of the veins in the area of the pampiniform plexus. If left untreated, insufficient blood circulation to the affected area can lead to urinary problems. In severe cases, the disease affects the quality of seminal fluid, increasing the risk of infertility. The Marmara operation for varicocele is a minimally invasive surgical intervention and ensures complete elimination of the pathology.
Read in the article
Complications after surgery
Indeed, serious consequences after such intervention are extremely rare. But it will not be possible to completely eliminate them.
So, during the recovery period the patient may find:
- Minor bleeding from the wound;
- Inflammation/infection (removed with antibiotics);
- Hydrocele of the ovary - caused by accidental damage to the lymph ducts;
- Testicular swelling;
- Allergic reaction to suture threads.
Relapse, that is, repeated vein defects in this area, is very rare. If this happens, then this phenomenon can be explained by the structural features of the male blood system.
Advantages of the technique
The incidence of varicocele is detected in 15% of the entire male population. The expansion of the walls of blood vessels in the area of the spermatic cord provokes excessive intra-abdominal pressure, physical overload, injuries to the pelvic organs, and tight underwear. In some cases, the process develops due to compression of the venous plexus by a growing tumor.
The initial stage of the disease is asymptomatic. The problem is revealed only when a feeling of heaviness appears in the scrotum on the side of the affected testicle. Discomfort increases during fast walking, running, and sudden movements. Over time, swollen veins begin to appear through the skin, the patient experiences pain at rest, and is unable to lead a full sex life.
Surgical treatment is used in advanced cases. Varicocele surgery according to Marmar has a number of advantages over other types of interventions:
- access to the affected area is through a small incision in the groin, which avoids extensive injury to muscle tissue and adjacent vessels;
- high precision using optical technology preserves the integrity of the pelvic organs and does not disrupt their functions;
- thanks to the gentle technique, there is no need for general anesthesia, and the risk of massive bleeding is significantly lower;
- a small incision in the projection of the venous plexus allows patients with a high degree of obesity and other pathologies to be operated in this way;
- The postoperative recovery period is several times shorter than with abdominal surgery.
Medical statistics record low rates of complications and relapses after using the technique. During the operation, the surgeon does not need to palpate the affected area through a layer of soft tissue. It is much easier to detect under thin skin; you just need to carefully remove it and separate it.
AndrologistMed recommends: Pros and cons
The microsurgical method has a number of advantages:
- low risk of complications in the postoperative period;
- low percentage of relapses;
- small, inconspicuous scar;
- short inpatient treatment;
- improvement in sperm count after six months.
The disadvantages of the operation are:
- high price;
- often used local anesthesia, which may not relieve the patient from pain during the operation.
- a technique that requires special equipment, as well as extensive experience and qualifications from the surgeon.
Preparing for the intervention
The need for Marmara surgery is discussed by the patient with the attending physician if progression of the varicocele is detected.
Preparation for intervention includes collecting laboratory results:
- general urine and blood analysis;
- a detailed biochemical test for the level of glucose, creatinine, bilirubin, urea;
- blood clotting test, coagulogram if necessary;
- spermograms;
- studies for HIV, hepatitis B and C, Wasserman reactions.
In order to identify cardiovascular abnormalities and infectious diseases of the lungs, an ECG and fluorography are performed. In the presence of chronic somatic and neurological diseases, acute inflammation, or trauma, the patient is prescribed additional types of examinations by specialized specialists.
The date of the operation is postponed if any acute process is detected in the patient, including ARVI.
Surgical intervention is contraindicated if the patient has:
- hypertension;
- severe heart damage;
- renal or liver failure;
- impaired hematopoietic function or low coagulability.
A few days before the intervention, the patient may be prescribed a course of anti-inflammatory and antibacterial drugs to prevent possible complications. In the last 12 hours, complete fasting and limited drinking are indicated.
Preparation
Before undergoing the Marmara operation, the patient must pass a mandatory minimum of laboratory tests and undergo all necessary instrumental studies. Before the procedure, the patient's hair in the future surgical area is shaved. The patient is prohibited from eating and drinking for 12 hours before the intervention. It is important to tell your doctor about any slight changes in how you feel before the surgical procedure. This will help avoid complications during surgery. Preparation before the intervention includes avoiding sports and avoiding nervous strain.
Technique of the operation
The operation is performed on an outpatient or inpatient basis, depending on the general condition of the patient. The groin area is thoroughly shaved and disinfected.
- The patient is given drugs for local anesthesia or epidural anesthesia. Under general anesthesia, Marmar intervention is performed extremely rarely.
- The surgeon dissects the skin and tissue below the inguinal ring, making an incision of 2.5–3 cm. Using special retractors, the layers of tissue are moved apart and the capillaries are compressed. The wound is dried with sterile material.
- An additional dose of anesthetic is injected into the levator muscle.
- The doctor gropes and removes the spermatic cord, fixing it to the edge of the wound. When working with vessels, a special microscope is used. The affected areas of the veins are clamped with a ligature. The tissues are irrigated with Papaverine to prevent spasm.
- After bandaging the main fragment, the patient is asked to tense the abdominal muscles by exhaling sharply. The so-called Valsalbe maneuver helps to identify unrecognized varicose veins and ligate them.
- After a control check of the vessels and the end of the operation, the wound is sutured with absorbable material and covered with a bandage. Sometimes threads are used that require removal after the suture has healed.
Subsequently, an almost invisible scar in the form of a thin line remains at the incision site.
Possible complications of the intervention include:
- suppuration of the surgical wound;
- increased body temperature;
- hydrocele;
- severe pain when moving.
To reduce the risk of subsequent infection, the patient is prescribed a course of antibiotics for several days. To relieve stress and maintain the venous plexus, it is recommended to wear a special bandage - a suspensor. Pain in most cases disappears after 5–7 days.
Classification
In addition to the side on which inflamed veins are found, varicoceles are divided depending on the size of the veins. This classification takes into account not only the magnitude of the development of varicose veins, but also how the distinctive signs are clearly diagnosed.
There are two types of pathology:
- without symptoms or preclinical;
- with obvious manifestations or clinical form.
When the presence of varicose veins has no symptoms and can be determined exclusively using ultrasound diagnostic methods, they speak of a preclinical form. This degree is called subclinical. Determining pathology by palpation in this case is impossible.
The photo schematically shows inflamed veins
Clinical forms have clearly distinguishable symptoms as shown in the photo, and can be diagnosed by palpation and visually. Depending on the development of the pathology, three degrees are distinguished, the characteristics of which are indicated in the table.
Classification of clinical forms of the disease
| Degree | Symptoms | Diagnostics |
| First | Characterized by mild and infrequent pain in the scrotum area. | Valsalva maneuver, ultrasound, Dopplerography. |
| Second | The pain is dull and nagging in nature, appears after exertion, and goes away at the end of the working day with rest. The veins are palpated. At this stage, lying down, the inflamed veins in the scrotum subside. | Palpation and visual |
| Third | The pain is constant and does not go away with rest. The veins are constantly inflamed, painful, and clearly visible. The scrotum swells on the side of the inflamed testicle, becomes bluish, and its skin becomes dry. The diseased testis decreases in size and sags. | Visually. Palpation. |
Please note that an ultrasound and spermogram should be prescribed even if the diagnosis is clear. These tests make it possible to most accurately identify the degree of pathology, which helps in the treatment and prognosis of the disease.
Drug therapy is accompanying, the main treatment is surgery
Diagnostics
Diagnostics includes both classical methods - palpation and visual examination, as well as the appointment of laboratory tests. The main diagnostic methods are described in the table.
Methods for diagnosing varicocele:
| Diagnostic method | Description |
| Palpation. Valsalva maneuver | Examination of patients Palpation helps to identify varicose veins in the second and third stages. The Valsalva maneuver allows you to identify the disease at the first stage. Instructions for carrying out: the man is in a standing position, straining or coughing, the doctor at this time feels the veins of the scrotum, which tense when the press is tense. |
| Visually | Visual manifestations of pathology The second and especially the third degree of varicose veins are detected visually: inflamed veins, morphological changes in the scrotum and testicle are visible. |
| Ultrasound and Dopplerography |
Ultrasound diagnostics registers even minimal changes in the lumen of the veins during the initial stages of the formation of varicose veins, and Dopplerography makes it possible to detect reflux and make its quantitative measurements (see Diagnosis and treatment of varicocele on the left). |
| Spermogram |
A spermogram allows you to identify pathologies of spermatogenesis, monitor and track the dynamics of the disease. This is an indispensable analysis in the fight and prevention of male infertility. |
| Biochemical blood test for hormones | Blood analysis Quantitative analysis of steroid male hormones allows us to assess the functional activity of the testes, since they are endocrine glands. Many physiological and biochemical processes, including the level of potency, depend on the amount of testosterone in the male body (see Is varicocele dangerous, does this disease affect potency). |
Timely diagnosis and treatment reduce the risk of male infertility
How to perform Marmara surgery for varicocele
Various treatment methods for varicocele are described in detail on this page . This article will discuss the surgical treatment of varicocele, and, first of all, the Marmara operation .
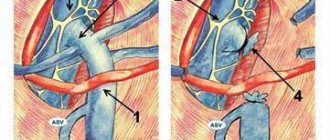
The purpose of surgery for varicocele is to ligate or cross the varicose veins of the testicle, thereby eliminating the cause of the disease and restoring normal blood supply. Previously, supra-inguinal access (that is, above the inguinal canal) was used for this purpose - these are the Ivanissevich and Palomo operations. At the same level, veins are crossed during laparoscopic surgery. The reason for the popularity of these methods was that the testicular vein at this level is represented by 1-3 rather large trunks, which, as a rule, were ligated as a single block, together with the accompanying lymphatic vessels, and in the Palomo operation - with the testicular artery. A fairly high percentage of relapses and complications (formation of dropsy, testicular atrophy) after these operations forced us to look for more effective and safe methods. And with the development of microsurgical technology, an operation was proposed that has become today the “gold standard” for the treatment of varicocele - the Marmara operation .
Indications for Marmara surgery are any stage of varicocele, including the bilateral form of the disease. The Marmara operation is especially effective for recurrent varicocele, after unsuccessful Ivanissevich or Palomo operations. Infertility caused by varicocele is a good reason to perform this particular microsurgical intervention due to the maximum positive effect on testicular function. In addition, the Marmara operation can easily be performed on patients who do not want general anesthesia (that is, anesthesia).
contraindications to performing the Marmara operation for varicocele. The exception is general surgical contraindications, which are described on this page . This intervention can be performed on all patients with varicocele, if the doctor has the appropriate experience and technical equipment.
Preparation for Marmaru surgery for varicocele involves shaving the pubic and scrotal hair (the evening before or the morning of the operation). If the operation is planned under general or spinal anesthesia, then for six hours it is necessary to avoid taking any liquid or food (strictly on an empty stomach).
Where and by whom is the operation performed?
Hospitalization for Marmar surgery is usually not required; in most cases, the procedure is performed one day in a day hospital. But if necessary, the patient can be left under medical supervision for 1-3 days. This may be necessary if the operation involved certain technical difficulties, required the use of general anesthesia, or led to decompensation of the man’s existing concomitant pathology. Hospitalization is also preferable when performing interventions in childhood.
USEFUL INFORMATION: Implantation bleeding or menstruation: how to distinguish?
For varicocele, surgery is performed by a urologist surgeon or reproductive specialist. In this case, the doctor must have a certificate to perform microsurgical interventions. After all, the Marmara technique involves the use of not only general surgical, but also special skills.
Marmara operation technique
The operation can be performed under general anesthesia, spinal or local anesthesia. The patient can choose the type of anesthesia in our clinic himself, after discussing all the pros and cons with the surgeon and anesthesiologist. During the Marmara operation, a small cosmetic skin incision (no more than 2-3 cm) is made in the groin area, on the side of the base of the penis. Next, the urologist isolates and holds the spermatic cord.
After hydropreparation, using an operating microscope and microsurgical instruments, each of the 8-12 stems of the testicular vein is isolated and ligated separately, avoiding crossing the lymphatic tract. Of course, this is a very painstaking work, which also requires special equipment, but the results of the operation are well worth the effort. During the isolation of the venous trunks, it is very important to identify and preserve the testicular artery and vas deferens. A microscope or binoculars help with this. on the accuracy of this stage of the Marmara operation .
Questions about the article
Novel
October 11, 2020 at 09:44 pm
Hello, I had Ivanisevich surgery at the age of 14, now I’m 45 and the veins in the groin area on the left side have started to swell. The tubercle near the penis can be visually seen to subside when pressed or lying down. Is it dangerous?
Anton Evgenievich Rotov
October 11, 2020 at 10:36 pm
I'm afraid that it is impossible to draw an accurate conclusion from the description. To clarify, do an ultrasound of the scrotum. You can send me the result by email
Salim, 23 years old
April 12, 2020 at 10:09 pm
Hello. I am 23 years old. On 03/21/19 I underwent laparoscopy of a varicocele on the left. After 7 days I discovered swelling and tenderness in the testicle. A diagnosis of acute epididymitis was made. Antibiotics and a local antitumor were prescribed. 24 days have passed, but the inflammation and swelling do not go away (inflammation of the appendage has decreased, but the pain on palpation or touch is acute). I took a blood and urine test and they said: everything is normal. Could lymphatic vessels or an artery be affected? operated by Professor K.M.N. Does it lead to dropsy?
drrotov
April 13, 2020 at 09:09 pm
During surgery, theoretically, various undesirable moments are possible. Let's hope everything ends well. Continue to be monitored by a urologist.
Postoperative period
After completion of the Marmara operation, the patient is placed in a ward for some time under the supervision of medical staff. After a follow-up examination, he can leave the clinic with an extract and recommendations.
The next day, I conduct another follow-up examination and a demonstration dressing change (in which I demonstrate the sequence of actions for the patient). Patients usually perform the rest of the dressings themselves at home. After 10-12 days, I once again monitor the healing of the wound and remove the stitches. At the request of the patient (for example, a nonresident who finds it difficult to come for an examination in 10 days), I apply self-absorbing sutures. Restrictions after Marmara surgery are limited to the exclusion of heavy physical activity for a period of 1 to 3 months.
In general, the postoperative period after Marmara surgery is easy. The patient does not become incapacitated and can return to daily activities the very next day. Pain is not typical for this operation, and the need to take painkillers is extremely rare.
A final examination, including ultrasound of the scrotum and spermogram analysis (if the Marmara operation was performed for infertility), is carried out 3 months after the operation.
Recovery after
From the operating room the patient goes to the ward, where he stays for no more than 2 - 4 hours, and then after an examination the doctor sends him home.
If there is severe weakness, severe pain in the wound, and the bandage quickly becomes wet, then the patient may be left in the department for observation until the next day.
Recommendations for home treatment indicate the necessary antibiotics and painkillers.
The dressing should be changed every day, and then every two to three days for a total of 10 days. After this, the stitches are removed.
During the first month, patients wear a suspensor that supports the operated testicle; they are not allowed to take a steam bath, engage in active sports, lift weights, or have sex. After consultation with a surgeon, some of the restrictions can gradually be lifted.
Complications of the Marmara operation for varicocele.
Like any surgical procedure, complications may occur with the Marmara operation . These include: bleeding and hematoma of the scrotum, infectious and inflammatory complications, relapse of varicocele, formation of testicular hydrocele (hydrocele), testicular atrophy. The frequency of complications of the Marmara operation directly depends on the experience of the surgeon and in my practice for many years does not exceed 1-2%. At the same time, fortunately, there were never any serious complications (which include testicular atrophy).
To reduce the risk of complications, I do not skimp on instruments; I use only proven and high-quality disposable consumables and suture material from leading Western manufacturers.
So, who needs to undergo Marmara surgery for varicocele?
- For a patient newly diagnosed with varicocele
- For a patient with bilateral varicocele
- In case of unsuccessful previous operations for varicocele
- In case of recurrence of varicocele
- A man with infertility due to varicocele
Where in Moscow can a Marmara operation be performed for varicocele? I operate at the Centrosoyuz Clinical Hospital, a cozy hospital located in the center of Moscow. The operation is performed both on a commercial basis and under a compulsory medical insurance policy.
The advantages of microsurgical varicocelectomy according to Marmar are:
- A small cosmetic incision in the groin area, in the hair growth area (the scar is almost invisible)
- The greatest efficiency of the operation is achieved through the use of operating binoculars and microsurgical instruments
- Lowest percentage of relapses and complications (less than 5 percent)
- Can be performed on an outpatient basis, without hospitalization
- Short and easy postoperative and recovery period
I offer my patients only the most modern and most effective treatment methods!
Indications for Marmara surgery
This method of surgical treatment can be prescribed for a disease such as varicose veins of the spermatic cord, or varicocele.
With varicocele, the normal blood circulation of the testicle is disrupted, which can lead to a deterioration in the quality and (or) motility of sperm - and, as a result, cause infertility.
According to various sources, about 20% of men face this problem.
Operation Marmara
Indications and contraindications
There is an opinion among clinicians about the need for surgery in patients who have reached adulthood. Today, varicocele is eliminated only according to the characteristics of the course, degree of development and risks of complications.
Among the main indications, doctors highlight the following:
- unsatisfactory spermogram data;
- pain, heaviness or discomfort in the scrotum;
- the desire to give an aesthetic appearance to the scrotal cavity.
The sensations with varicocele are reminiscent of testicular hydrocele. Signs of pathology intensify in hot weather, when feeling unwell, and when walking. Sometimes provoking factors can be an inguinal hernia, tumors (usually oncogenic), and indirect varicose veins due to hemorrhoidal growths. In addition to the indications for Marmara surgery, there are a number of contraindications.
Contraindications
Contraindications can be both relative and absolute. The feasibility of the procedure is determined by the doctor after diagnostic studies and studying the patient’s clinical history; the main ones include:
- infectious diseases of various origins (for example, acute respiratory viral infections, acute respiratory infections, influenza);
- drugs that increase blood clotting;
- exacerbation of chronic diseases (enterocolitis, peptic ulcer, ENT diseases);
- seasonal allergic reactions;
- the period after critical conditions (myocardial infarction, stroke, hypertensive crises with alveolar edema, and others).
The decision to perform an operation is made by a urological surgeon based on diagnostic data, clinical history and patient complaints. If there are objective indicators that the operation is impossible, the patient is offered alternative methods to solve the problem.
Stages and technology of the procedure
Varicocele surgery is performed in one day in a day hospital. The procedure itself takes 20 minutes. Depending on the symptomatic picture and stage of the disease, the patient may be left under observation for 72 hours. Hospitalization is carried out in cases of technical complications during the procedure or in case of decompensation of a concomitant illness. Children must be hospitalized.
Operation Marmara
The Marmara operation technique for varicocele involves the use of a local anesthetic. General anesthesia is used very rarely, in cases of serious complications. The procedure is carried out by penetrating through a small incision located in the groin area, in close proximity to the spermatic cord. The approach provides the opportunity to bypass the main vessel and retrogradely approach the transformed ducts of the appendages of the scrotum.
After anesthesia, the upper layer of the dermis and fiber are dissected, and the tissues to be phased are separated with retractors. Bleeding vessels are compressed and the wound is dried. Next, the muscle that elevates the testicle is retracted and an anesthetic drug is injected. Then the surgeon isolates the spermatic cord and fixes it. At this stage, optics are used to make movements more precise.
Deformed vessels are tied with silk thread. All vessels with a diameter greater than 2 mm are subject to ligation. Next, the surgeon checks the quality of the sutures by applying Papaverine hydrochloride. This allows you to relieve the vasomotor spasm that occurs reflexively, and to see bleeding areas if the lumen of the deformed vessels was not completely blocked.
A thorough examination and Valsalve test can help identify defects in the work. The dissected layers are sutured alternately with absorbable threads. In some cases, a non-absorbable thread is applied only to the outer layer, about which the patient is warned in advance.
Upon completion of the procedure, a sterile dressing is applied to the suture. If there are no signs of postoperative bleeding, the patient is sent home. After the procedure, a course of antibiotics is required. Do not neglect this additional measure, otherwise the risk of infection or infection increases.
Advantages and disadvantages of the Marmara operation
Compared to other methods of intervention, the Marmara method has the following advantages:
- Low risk of complications and relapses associated with increased accuracy of the operation.
- Invisible seam.
- Small incision, less chance of infection, short hospital stay.
- No complications of general anesthesia.
The disadvantages of the technique are usually listed as:
- High cost of the operation.
- Painful sensations before and during the intervention. This is due to the predominant use of local anesthesia.
- The surgical technique is highly dependent on the qualifications of the doctor and the technique used.
Recovery period
The Marmara operation allows you to cure a patient literally in 1 day without a significant risk of complications or relapse of the pathology. The recovery period after marmara surgery is quite easy for most patients, without complications. After all the manipulations have been carried out, a man should not significantly change his daily routine or established lifestyle.
During the first few days after the operation, patients are advised to refrain from any physical activity. You will also have to significantly reduce excessive physical activity over the next few months.
In rare cases, the following complications have been reported after surgery:
- bleeding;
- wound infection;
- development of dropsy;
- re-development of the disease.
After the operation is performed, the patient will be advised to undergo regular physical examination by his attending physician so that he can be convinced of the effectiveness of the therapy. The patient will also have the bandage changed and the wound healing process monitored. Sutures are removed 1 week – 14 days after the procedure.
conclusions
Varicocele is a male ailment that is one of the factors of infertility. And this is explained by the fact that in a testicle with such a defect the temperature is higher than normal. It approaches the general body temperature, and for healthy sperm production the temperature should be slightly lower. Also, with varicocele, oxygen starvation of the testicle is recorded, and in its tissue, in addition, free radicals can accumulate, which damage these same tissues. If you do not operate on time, the problem of male infertility can become difficult to resolve.
The choice of method to eliminate the problem depends not only on the medical decision: the patient’s readiness for surgery is also important.
Sometimes you have to consult not only a urologist from the clinic, but also another specialist. There is no need to worry: the rarest operations lead to complications. The problem must be solved clearly, and these drastic actions should not be put off for a long time.
How to prepare for the procedure?
Preparation for surgery involves the final formulation and clarification of the diagnosis of “varicocele”. Further examinations should identify possible medical diseases or infections for which surgery cannot be performed.
The main preparatory examinations are:
- fluorography;
- ECG;
- general blood test with leukemia formula;
- general urine analysis;
- determination of platelet count and blood clotting time. If a history of thrombus formation is detected, a coagulogram is performed;
- biochemical blood test (determination of glucose levels, bilirubin and its fractions, urea and creatinine);
- analysis for hepatitis B and C;
- test for sexually transmitted diseases (syphilis);
- spermogram.
If there are any pathologies, consult a specialist and his written permission or prohibition to perform surgical intervention. The specialist may also recommend therapy for the postoperative period to avoid complications due to the existing disease.
Preparation for surgery on the part of the patient is as follows:
- on the eve of the operation it is necessary to take a shower;
- shave the pubis and perineum;
- Refrain from eating and drinking for 12 hours (this will make it easier to recover from anesthesia);
- take medications approved by your doctor;
- If you experience symptoms of a cold or flu, notify a specialist;
- to refuse from bad habits;
- refrain from sexual intercourse before the procedure.