Acute disorders of mesenteric circulation. Intestinal infarction
Synonyms: intestinal infarction, mesenteric thrombosis, acute mesenteric ischemia, acute mesenteric circulation disorder, acute intestinal vascular disease.
This is a group of pathological conditions similar in course and prognosis, caused by disturbances in blood flow in the arterial, venous or microvasculature of the mesenteric vessels. This pathology is one of the most severe diseases that a surgeon has to deal with in his practice, and is currently accompanied by an extremely high mortality rate (67-92%). Unsatisfactory treatment results are primarily due to late diagnosis and inadequate surgical tactics.
ICD-10 CODE
K55.0. Acute vascular diseases of the intestine.
Classification
Disease code according to ICD-10 K55.0.
Pathology is usually classified into three main groups:
| Acute mesenteric infarction | In most cases, the superior mesenteric artery is affected, and in most cases the cause is not thrombosis, but embolism; patient complaints usually fit the picture of an “acute abdomen”. |
| Obliteration of chronic type | More often it is characterized by occlusion or obliteration of the celiac trunk, superior mesenteric artery, less common is occlusion of the main trunk of the inferior mesenteric artery. |
| Mesenteric ischemia of non-occlusive type | Occurs in 50% of cases. |
| Thrombosis of mesenteric veins | Occurs quite rarely. |
The most common cause of thrombosis of this type is long-term atherosclerosis, the treatment of which was not carried out or was carried out insufficiently.
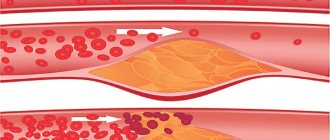
The mechanism is simple: a cholesterol plaque begins to form in one of the vessels, which sooner or later clogs the lumen of the vessel completely, blocking the blood flow. The area of the intestine that does not receive blood begins to change irreversibly, and the changes originate from the mucous membrane.
As pathological processes progress, the intestinal wall becomes thinner and, as a result, the contents end up in the abdominal cavity. The result is peritonitis.
Another reason for the development of pathology is blood hypercoagulation, in which blood coagulates inside the vessel. This occurs due to an imbalance between the coagulation and anticoagulation systems.
In this case, hypercoagulation can be both congenital and acquired.
The cause of the development of the disease can also be damage to the vascular endothelium, due to which substances that trigger blood clotting processes enter the bloodstream in excess.
Most often, endothelial damage develops due to chemotherapy for tumor processes, surgical interventions, and injuries.
A common reason for the development of thrombosis is also stagnation, which is formed due to an incorrect lifestyle or prolonged forced immobility of the patient.
Other reasons may be:
- inflammatory pathologies of the abdominal cavity;
- injuries that interfere with normal blood circulation;
- endocarditis;
- myocardial infarction.
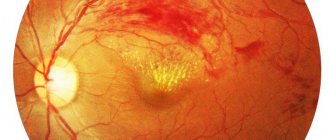
From here you can find out in detail the description of central retinal vein thrombosis.
Read also: Varicose veins of the uterus and pelvis
Epidemiology
Acute disorders of mesenteric circulation are more common in elderly and senile patients. Although the average age of patients is about 70 years, this does not exclude the possibility of developing the disease in young people. The proportion of deaths from intestinal infarction under the age of 40 is about 10%, with half of the deaths under 30 years of age. Among the patients, women significantly predominate. In recent years, acute disorders of mesenteric circulation have become more common, which is associated both with an increase in human life expectancy and with the spread of congenital and acquired thrombophilic conditions.
Prevention
The occurrence of intestinal arterial thromboembolism can be prevented through timely surgical treatment of aortic and mitral heart defects, adequate antiarrhythmic therapy and long-term use of indirect anticoagulants in patients with a permanent form of atrial fibrillation. Prevention of atherothrombosis involves the constant use of antiplatelet agents. To prevent venous mesenteric thrombosis, it is necessary to identify and correct thrombophilic conditions.
How does the chronic form of thrombosis manifest?
The chronic form of thrombosis should be considered in patients with heart failure complicated by myocardial infarction. The clinic distinguishes 4 stages:
- I - the patient has no complaints, the thrombus is an accidental finding during angiography;
- II - typical complaints of pain along the intestines after eating, the person refuses food because of this;
- III - constant pain, flatulence, impaired absorption of the small intestine, diarrhea;
- IV - the occurrence of intestinal obstruction, which manifests itself as an “acute abdomen”, with peritonitis and gangrene.
Main features of pathology
Among practical surgeons, there are still two myths regarding acute disorders of mesenteric circulation. First: “Such a disease exists, but it is extremely rare.” Second: “If a patient has developed mesenteric thrombosis, then there is practically no chance of recovery.” Both points of view, of course, have certain grounds, but they do not always correspond to reality.
Why do these ideas not correspond to the real state of affairs, although they are very similar to the truth? Indeed, acute disorders of mesenteric circulation have been considered extremely rare diseases for many years. If we analyze reports from general surgical hospitals, the proportion of patients with acute disorders of mesenteric circulation is only 0.10-0.39%. At the same time, it is well known that these patients are hospitalized with suspicion of various other diseases not only in surgical and vascular departments, but also in therapeutic, infectious diseases, cardiac intensive care units, etc. Analysis of general hospital mortality based on autopsy data shows that the percentage of deaths from disorders mesenteric blood flow is significantly higher - from 1.0 to 2.5%. The number of deaths from intestinal infarction exceeds the number of deaths from such a common disease as acute appendicitis. To these figures it is necessary to add favorable treatment outcomes and cases of compensation or subcompensation of mesenteric blood flow occurring spontaneously or under the influence of conservative therapy, and then it becomes clear that this pathology does not at all belong to the category of casuistic.
The existence of the second myth stems from the first and is due, first of all, to late diagnosis. Often time is missed for correct actions only because, when conducting differential diagnosis in an unclear clinical situation, the surgeon simply does not include this pathology in the list of analyzed causes of the patient’s serious condition.
In addition, one more important point must be taken into account. There is such a method of making a diagnosis in an unclear situation as dynamic observation
, which in emergency surgery all clinicians constantly and successfully use and are accustomed to trusting it. In the case of an acute disorder of mesenteric circulation, this method can deprive the patient of his last chance at life, since irreversible changes in the intestinal wall occur within 6-8 hours. When the doctor finally comes to the idea of the correct diagnosis, he will no longer be able to help the patient with developed total intestinal necrosis.
To understand the pathogenesis of acute disorders of mesenteric circulation, the nature and extent of damage to various parts of the gastrointestinal tract, it is necessary to consider the features of its blood supply.
Blood supply to the intestines
Arterial blood supply
The intestine is carried out by two unpaired branches of the abdominal aorta - the superior and inferior mesenteric arteries.
The superior mesenteric artery
(
a. mesenterica superior
), unpaired, departs from the anterior surface of the aorta at the level of the XII thoracic or I lumbar vertebra, immediately below the celiac trunk, goes down and forward. The acute angle of origin of the superior mesenteric artery makes it a kind of “trap” for emboli. Coming from under the lower edge of the neck of the pancreas, the artery lies on the anterior surface of the ascending part of the duodenum, and then enters the mesentery of the small intestine and descends to the right iliac fossa, branching into its terminal branches. The superior mesenteric artery gives off the following branches: the inferior pancreatic-duodenal artery, anastomosing with the superior artery of the same name, 18-24 intestinal arteries running in the mesentery to the loops of the jejunum and ileum, the ileocolic artery, the right and middle colic arteries. Thus, it has a huge “area of responsibility”, supplies blood to the entire small and right half of the large intestine, and participates in the blood supply to the duodenum and pancreas. Near the mouth, the average diameter of the artery is about 9 mm (from 6 to 15 mm), then as the branches depart, its lumen gradually narrows, and after the ileocolic artery departs, it is halved.
The left half of the colon is supplied by the inferior mesenteric artery
(
a. mesenterica inferior
), unpaired, which extends from the anterior left surface of the aorta 3-5 cm above its bifurcation. The artery divides into the left colon, sigmoid arteries and superior rectum. It has powerful collateral connections with the superior mesenteric through anastomoses between the left colic and middle colic arteries (Riolan arch) and with the internal iliac arteries through anastomoses between the upper, middle and lower rectal arteries.
The system of anastomoses between the superior and inferior mesenteric arteries is capable of functioning effectively only in one direction - from the basin of the superior mesenteric artery to the basin of the inferior mesenteric artery. In other words, the superior mesenteric artery is able to compensate for the occlusion of the lower one and take over the blood supply to its basin, but vice versa - not. This feature of the blood supply to the colon explains the absence in most cases of ischemic damage during occlusion of the mouth of the inferior mesenteric artery. If necrosis develops, the area of damage is usually limited to the sigmoid colon. Thus, when talking about acute disruption of the arterial mesenteric blood supply, as a rule, they mean occlusion of the superior mesenteric artery.
Diseases of the digestive system (K00-K93)
Excluded:
- selected conditions occurring in the perinatal period (P00-P96)
- some infectious and parasitic diseases (A00-B99)
- complications of pregnancy, childbirth and the puerperium (O00-O99)
- congenital anomalies, deformities and chromosomal disorders (Q00-Q99)
- diseases of the endocrine system, nutritional disorders and metabolic disorders (E00-E90)
- injuries, poisoning and some other consequences of external causes (S00-T98)
- neoplasms (C00-D48)
- symptoms, signs and abnormalities identified by clinical and laboratory tests, not classified elsewhere (R00-R99)
This class contains the following blocks:
- K00-K14 Diseases of the mouth, salivary glands and jaws
- K20-K31 Diseases of the esophagus, stomach and duodenum
- K35-K38 Diseases of the appendix [vermiform appendix]
- K40-K46 Hernias
- K50-K52 Non-infectious enteritis and colitis
- K55-K64 Other intestinal diseases
- K65-K67 Diseases of the peritoneum
- K70-K77 Liver diseases
- K80-K87 Diseases of the gallbladder, biliary tract and pancreas
- K90-K93 Other diseases of the digestive system
The following categories are marked with an asterisk:
- K23* Lesions of the esophagus in diseases classified elsewhere
- K67* Lesions of the peritoneum in infectious diseases classified elsewhere
- K77* Liver lesions in diseases classified elsewhere
- K87* Lesions of the gallbladder, biliary tract and pancreas in diseases classified elsewhere
- K93* Affects of other digestive organs in diseases classified elsewhere
Read also: How many times can there be a varicocele?
Excludes: diaphragmatic hernia (K44.-)
The following additional fourth codes are for use with categories K25-K28:
- .0 Acute with bleeding
- .1 Sharp with perforation
- .2 Acute with bleeding and perforation
- .3 Acute without bleeding or perforation
- .4 Chronic or unspecified with bleeding
- .5 Chronic or unspecified with perforation
- .6 Chronic or unspecified with bleeding and perforation
- .7 Chronic without bleeding or perforation
- .9 Unspecified as acute or chronic, without bleeding or perforation
Note. A hernia with gangrene and obstruction is classified as a hernia with gangrene.
Included: hernia:
- acquired
- congenital [except diaphragmatic or esophageal hiatus]
- recurrent
Includes: non-infectious inflammatory bowel diseases
Excluded:
- irritable bowel syndrome (K58.-)
- megacolon (K59.3)
Factors of occurrence
The causes that provoke the development of the disease (ICD code 10 I 80) are divided into 3 factors:
- Thickening of the blood due to changes in its composition.
- Reducing the speed of blood flow.
- Damage to the inner lining of blood vessels.
These factors are diagnosed individually or in combination. They contribute to the development of varicose veins, which is the cause of acute thrombophlebitis.
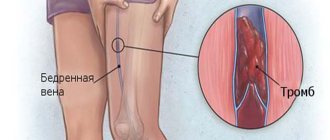
Vein thrombosis is a rather dangerous disease that can be fatal if a blood clot breaks off and enters the arteries of the lung or heart.
Thrombophlebitis (ICD code 10 I80) develops with forced immobility of a limb (with a fracture).
Thrombosis of the veins of the lower extremities is caused by taking estrogen-containing hormones prescribed for infectious and autoimmune diseases. Oncological diseases provoke thrombophlebitis of the lower extremities. Installation and long-term presence of a catheter in the venous bed and frequent injury to the walls by injections lead to the formation of blood clots.
In 65% of cases, thrombophlebitis is diagnosed in women. The pattern is associated with wearing high-heeled shoes, tight jeans and taking hormonal contraceptives. The cause of the disease may be pregnancy. During this period, physiological activation of coagulation processes occurs, preventing bleeding in the postpartum period, and the inflamed vessel wall leads to the formation of a blood clot. People aged 40-55 years are at risk. At this age, the condition of the body's vascular system deteriorates significantly.
Thrombosis is hereditary. Causative factors include obesity, unbalanced diet, physical activity, smoking and drinking alcoholic beverages.
Deep vein thrombosis has a specific code in the ICD-10 classification – I80
Diagnostics
In order to diagnose deep vein thrombosis, which is included in the ICD-10 classifier, the doctor must conduct an external examination, as well as conduct a series of laboratory tests. Skin color, the presence of swelling and vascular nodes are taken into account. The following research methods are usually used:
- Blood analysis,
- Coagulogram,
- Thromboelastogram,
- Determination of prothrombin index, as well as C-reactive protein.
The deep veins are examined using ultrasound to determine the nature of the blood clot that has formed.
Classification of the disease
ICD 10 code I80 includes phlebitis and thrombophlebitis. Symptoms vary depending on the location of the clot. There are 2 types of diseases:
Superficial thrombophlebitis develops in the great saphenous vein. It is easy to diagnose. Inflammatory changes occur in the area of the affected vessel, but if varicose veins are not observed, then thrombophlebitis is interpreted by ICD 10 as a complication of gynecological pathology or a symptom of a malignant tumor in the organs of the digestive system. Thrombophlebitis ICD 10 also includes thrombosis in the intestine.
When palpating the inflamed saphenous vein, the patient experiences stabbing pain. Symptoms of superficial thrombophlebitis: scarlet stripes on the skin, swelling of the ankles and feet, increased body temperature.
Without treatment, thrombosis spreads to the deep veins. The patient's health worsens. Infiltration and hyperemia are observed in the area of the thrombosed vessel.
There are 2 types of thrombosis that require special attention:
- Ileofemoral thrombosis is a subtype of deep vein thrombophlebitis. The disease affects large vessels in the femoral and iliac veins. If blocked, it can be fatal. Ileofemoral thrombosis develops rapidly. The patient develops severe swelling of the lower extremities. High body temperature is added to the symptoms. The skin acquires a bluish tint. Complete blockage can lead to the development of gangrene.
Such an acute inflammatory process of the lower extremities is dangerous for human life, and ignoring it can lead to death
- Mesenteric vascular thrombosis is a blockage of the mesentery or mesentery. Without treatment, thrombosis of the mesenteric vessels leads to the death of the affected area. Mesenteric thrombosis (code K55 in ICD 10) requires immediate surgical intervention.
Signs
At the initial stages of development, disease of the vessels and deep veins of the lower extremities can occur without the appearance of any symptoms. But soon the following signs appear:
- swelling of the lower extremities occurs. Moreover, the higher the area of inflammation is located, the more pronounced the edema process is,
- painful sensations of a pulling and bursting nature,
- the skin becomes very sensitive and reacts to any pressure. In the place where vascular thrombosis has formed, it becomes warmer and acquires a reddish tint. Often the surface of the lower extremities acquires a bluish color characteristic of the disease,
- itching and burning,
- the venous system becomes more expressive and changes its structure.
Sometimes an infection is added to the inflammatory process, which can lead to an abscess and purulent discharge.
Symptoms
Thrombosis of the lower extremities according to the clinical picture is classified into:
- Spicy. Symptoms of the acute form appear suddenly. The patient experiences muscle pain along the thrombosed vessel. Acute thrombosis is accompanied by elevated body temperature. Red stripes appear on the skin. Deep vein thrombophlebitis differs from superficial thrombophlebitis in severe swelling, heaviness in the legs and bluish skin. The pain intensifies, causing lameness.
- Chronic. With this form, blood clots may dissolve or enlarge. Chronic deep vein thrombophlebitis has a sluggish nature. The patient may experience pain only upon palpation.
The main factors that can provoke deep vein thrombophlebitis are: tissue nutritional disorders and the development of aseptic inflammation
When the inferior vena cava is blocked, bilateral swelling of the limb is observed. If the thrombus is located in the iliac segment, then unilateral edema is noted. When walking for a long time, aching pain appears in the calf muscle.
Thrombosis is manifested by numbness of the limbs, loss of sensitivity, tingling of the skin, chills and hardening of the lymph nodes. The first symptoms of the chronic form may appear a year after the exacerbation. The disease can be migratory in nature. This form is characterized by rapid development. The migratory form affects the superficial veins. Dense thrombosed nodules can change their position, appearing in different parts of the limb. Seals are accompanied by swelling and increased body temperature.
International disease code
At the head of statistics in health care and the systematization of all pathological conditions is the document “International Statistical Classification of Diseases and Health-Related Problems.” It was created through the efforts of the World Health Organization. The document is reviewed by it once a decade with a view to making amendments. Since 1999, the Russian Federation has used ICD-10 (tenth updated reissue).
The main feature of ICD-10 is its alphanumeric encryption technique. This code uses one Latin letter and three numbers. The classification is divided into 21 classes, which correspond to the first letter of the ICD-10 code. Classes are divided into blocks of different headings.
In accordance with ICD-10, thrombophlebitic lesions of the superficial and deep veins of the lower extremities belong to class I00-I99 Diseases of the circulatory system. This class includes blocks describing rheumatic heart pathologies, disorders caused by high blood pressure, cerebrovascular diseases, ischemic and other heart pathologies.
Lesions of the veins, lymphatic trunks and nodes, not systematized in other headings, including diseases of the peripheral superficial or deep vessels of the lower extremities, belong to block I80-I89.
Thrombophlebitis of the superficial and deep vessels of the legs belongs to the combined category of phlebitis and thrombophlebitis. This category has its own subsection in the ICD-10 classification: nosological class I80 Phlebitis and thrombophlebitis. This subsection covers endophlebitis, perivenous and intrinsic inflammation of the venous trunks, including purulent. The subsection does not include thrombophlebitic processes that complicate medical termination of pregnancy, childbirth and the immediate days after birth, pathological post-inflammatory intracranial blockages, blockages of the spinal cord, portal vein and migratory vessels, as well as postphlebitic syndrome.
I80 Phlebitis and thrombophlebitis:
- I80.0 superficial vessels of the legs.
- I80.1 femoral venous vessel.
- I80.2 other deep vessels.
- I80.3 lower extremities of uncertain location.
- I80.8 other location.
- I80.9 unspecified localization.
Thrombophlebitic lesions of the superficial veins of the lower extremities are coded I80.0. This painful condition requires a differential diagnosis with thromboangiitis obliterans I73.1, lymphangitis I89.1 and periarteritis nodosa M30.0.
Damage to the deep veins of the lower extremities is encrypted under code I80.3. A differential diagnosis of thrombophlebitis is carried out with thrombosis of the arterial trunks I74.3–I74.5, obliterating endarteritis I70 and symmetrical gangrene (Raynaud's disease) I73.0.
ICD-10 does not indicate whether the process is acute or chronic.
The eleventh revision of the international disease register (ICD-11) is planned for 2020. Unlike ICD-10, subsequent classification will take into account etiology, clinical and diagnostic signs, effect on pregnancy and quality of life.
Treatment
For thrombophlebitis, doctors prescribe treatment based on the diagnostic results obtained. Treatment includes:
- drug therapy;
- surgical intervention.
Thrombophlebitis has several forms: acute and chronic
If thrombosis affects the superficial veins, then treatment is carried out with medication. The patient is prescribed phlebotonics, anti-inflammatory drugs, ointments. Conservative treatment relieves swelling, reduces pain and restores blood flow. Anti-inflammatory drugs include drugs such as Ibuprofen, Aspirin and Diclofenac. Heparin ointment and Troxevasin have a local effect.
For thrombosis of superficial veins, doctors prescribe electrophoresis with anticoagulants, UHF therapy and magnetic therapy. Physiotherapeutic procedures dissolve blood clots and reduce swelling and pain.
Conservative treatment is carried out in combination with compression therapy. For thrombophlebitis, elastic bandages and compression stockings (stockings or tights) should be worn. The degree and class of compression is prescribed by a phlebologist depending on the severity of the disease.
Short description
Atherosclerosis of the mesenteric arteries is manifested by two main syndromes: abdominal angina and thrombosis of arterial (often venous) branches. The latter is accompanied by acute or chronic intestinal ischemia, and subsequently chronic ischemia develops.
• Abdominal toad - an attack of colic-like abdominal pain - occurs soon after eating, often relieved by nitroglycerin, repeated vomiting and bloating are often observed; fasting stops attacks of abdominal pain; diagnosis is difficult (rarity of the syndrome, lack of specific signs) and is extremely important due to the danger of untimely recognition of acute pathology of the abdominal organs. Treatment : split meals, nitroglycerin, papaverine hydrochloride 0.04–0.06 g 3–4 times a day before meals, pancreatin (1–1.5 g) or panzinorm forte (1–2 tablets) after meals.
• Acute mesenteric ischemia is a classic syndrome of decreased blood flow, usually due to damage to the superior mesenteric artery. Patients are found to have advanced atherosclerotic cardiovascular pathology, often with a history of chronic heart failure, myocardial infarction, cerebrovascular disease or peripheral vascular disease. Many patients received drugs that cause spasms of the smooth muscles of internal organs (for example, digoxin). Mesenteric vascular embolism is often associated with cardiac arrhythmias. Clinical picture •• The most common symptom is sudden severe pain in the umbilical region •• Quiet abdomen with reduced peristalsis. With circulatory decompensation, necrosis develops in the intestinal wall, with an increase in the clinical picture of paralytic intestinal obstruction, and later peritonitis. The diagnosis is established by X-ray data, supported by changes in blood parameters (leukocytosis, often more than 20´109/l) and angiography data. A Doppler study can detect decreased blood flow through the superior mesenteric artery or celiac trunk. Treatment is surgical removal of the embolus; In some cases, antithrombotic agents, balloon angioplasty of narrowed vessels, or bypass surgery are used. Considering the latent course of the initial stage of the disease, the disease is more often diagnosed intraoperatively in patients with symptoms of peritonitis with an unclear diagnosis. In the presence of segmental necrosis, after embolthrombectomy, resection of the necrotic area of the intestine is performed. With total intestinal necrosis, death is inevitable, and symptomatic treatment is carried out - analgesics.
• Chronic mesenteric ischemia develops only in the presence of significant occlusion of two of the three main visceral arteries, usually in elderly individuals with a history of cardiovascular disease. Clinical picture •• Intermittent cramping pain in the abdomen, occurring 15-30 minutes after eating and lasting for hours •• Characteristic fear of food in most patients due to the connection of the pain syndrome with food intake •• Loss of body weight. The diagnosis is confirmed by angiographic detection of significant narrowing (>50%) of two of the three main visceral arteries. Treatment is surgical reconstruction of blood vessels. Pharmacological correction with vasodilators is ineffective.
• Ischemic colitis occurs due to insufficient supply of arterial blood to the colon (usually to the left half, especially in the area of the splenic flexure). The high vulnerability of the intestinal blood circulation in this area is caused by the junction of the superior and inferior mesenteric arteries. The rectum, which has an abundant blood supply, is extremely rarely susceptible to ischemic lesions. Clinical picture •• Diarrhea (blood in the stool) •• Pain in the lower abdomen •• Vomiting (rare). The diagnosis is suggested by excluding other causes of bloody diarrhea in the elderly (polyp, carcinoma, diverticulitis or angiodysplasia) •• Leukocytosis up to 20´109/l •• Irrigography or CT reveals diffuse changes in the submucosal membrane, sometimes with the presence of gas in the intestinal wall •• Sigmoidoscopy in most cases helps to detect only the presence of mucus mixed with blood. Treatment •• Parenteral nutrition •• Antibiotic therapy to prevent secondary infections. The prognosis for chronic ischemia is generally favorable. Late strictures may develop and require balloon dilatation or surgical excision.
ICD-10 • I70.8 Atherosclerosis of other arteries • K55 Vascular diseases of the intestine
Thrombosis of mesenteric vessels: symptoms, causes, treatment
- Causes of the disease
- Symptoms of the disease
- Treatment of pathology
Mesenteric vascular thrombosis is a disturbance in the strength and flow of blood in the mesenteric vessels due to mechanical blockage of the veins. Vascular occlusion leads to acute ischemia with the possible development of intestinal infarction and peritonitis.
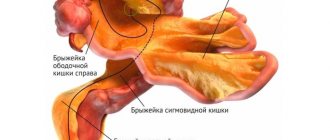
Mesentery are mesenteric cords through which internal organs are attached to the posterior abdominal wall, including the intestines.
Veins pass through it to the small intestine, nerve endings, and mesenteric lymph nodes.
Lymphatic system of the abdominal cavity
Changing the vascular walls is not a matter of one year, manifesting itself after several decades from the time of activation.
Therefore, diagnosis of the disease often occurs in adulthood or old age.
The risk group for diagnosing the disease should include people who have disturbances in the functioning of the organs of the circulatory system, neoplasms, mechanical injuries, or after surgery.
In accordance with the international classification of diseases, 10th revision, thrombosis of mesenteric veins in newborns is not a separate pathology; it is assigned an ICD-10 code. According to the ICD code - 10, intestinal thrombosis is defined as a severe vascular process.
Today, a number of variants of the pathology are known:
Thrombosis. It is characterized by the direct formation of a blood clot in the mesenteric veins and arteries, which provokes partial and complete blocking of blood flow and an increase in the synthesis of coagulation parameters.
Heart attack. Pathology involves occlusion of blood flow due to a violation of the integrity of the vessel structure in the intestinal wall, after which the intestinal tissues are filled with blood. After diagnosing a blood clot, treatment of the disease has two surgical options: removal of the clot or necrotic area of the vessel.
Embolism. A distinctive feature of the disease is that after a blood clot forms in one vessel, for example, in the lower extremities, it breaks off and “travels” throughout the body, becoming attached to another vein or aorta.
Embolism is the most dangerous disease, because no one can predict the trajectory of the clot, the separation field, or determine the disease, for example, thrombosis of cerebral vessels, and, accordingly, the lesion.
It should be noted that chronic deformation of blood vessels in the intestine is the result of various pathologies of microcirculation, not excluding diseases of the lower extremities.
Causes of the disease
The reasons for the activation of the disease are different. Despite this fact, the prerequisites for the development of the disease for the patient are the presence of dysfunctions in the local or general blood flow, and a predisposition to the formation of clots (genetic). The most common causes of mesenteric vascular thrombosis are as follows:
- Congenital, acquired heart defects. They cause heart failure, in which the speed of blood flow slows down and a clot forms on the valve.
- Hypertensive diseases along with atherosclerosis.
- Atherosclerotic diseases in blood vessels, during which plaque formation occurs, gradual blockage of veins and aortas occurs; possible “clot travel”, embolism of veins and arteries. For example, atherosclerosis can provoke thrombosis of cerebral vessels.
- Heart attack.
- Varicose veins The disease is characterized by the detachment of a parietal thrombus, after which it provokes occlusion of the mesenteric vessels.
- Septic condition. The pathology is characterized by impaired microcirculation, an increased risk of the formation of clots of various sizes, and the spread of bacteria (sinus thrombosis).
- Postoperative complications. For example, the most common complications after surgery during the rehabilitation period are: sinus thrombosis of the dura mater, sinus thrombosis of the cavernous vessel, etc.
Causes of pathology
For most situations, the causes that provoked thrombosis of the mesenteric vessels cannot be eliminated in a short period. Effective treatment involves exclusively surgical intervention, removal of consequences, and prevention of the cause of activation of the pathology.
The volume and location of development of diseases of the small and large intestines directly depend on the location of occlusion of the mesenteric vessels. Diagnosis of occlusion of the upper artery: a section of the intestine is subject to necrosis: the entire thin intestine and the initial parts of the thick intestine. Diagnosis of occlusion of the lower artery, pathology manifests itself as dystrophy. Necrotic deformities of the descending parts of the colon.
Intestinal thrombosis can be artificially caused by the actions of an unqualified surgeon on the aorta, in which, after removing the clot, the stationary blood flow follows its direction to the region of the lower extremities. Thus, steal syndrome is formed, that is, intestinal ischemia due to increased blood flow in the lower extremities.
Symptoms of the disease
The symptoms of the disease from one position have a unique character, and from the other they are similar to such common diseases as appendicitis and ulcers. The main symptom of activation of intestinal thrombosis is a sudden severe pain.
As the pathology progresses, the intensity of the pain increases, the person cannot move or carry on a conversation normally. The location of the pain completely depends on the period of the disease and where the vessel occlusion occurred.
Symptoms of pathology
After a certain period, a patient with intestinal thrombosis experiences a variety of symptoms affecting the digestive tract (dehydration with blood discharge, mucus). The progression of the pathology is indicated by obstruction of food, bloating, flatulence, inability to listen to peristaltic sounds, weakness of the lower extremities and body.
Symptoms of intestinal thrombosis and a subsequent period of wall necrosis often occur with peritonitis. Along with this, the patient feels pain, manifestations of intoxication of the body (weakness of the lower extremities, high temperature, sudden changes in blood pressure, weak pulse sensitivity).
Based on these symptoms, a qualified specialist can correctly make a diagnosis and determine the severity of the disease. Therefore, it is important to contact a medical facility to make a timely diagnosis based on the existing symptoms.
Otherwise, if you ignore the symptoms, namely weakness of the lower extremities and pain, you can expect irreversible consequences, for example, diagnose cerebral vascular thrombosis (cavernous sinus, superior longitudinal sinus, transverse sinus, inferior longitudinal sinus, anterior intercavernous sinus, posterior intercavernous sinus .
Symptoms and treatment of mesenteric intestinal thrombosis
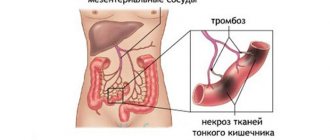
A dangerous disease is intestinal infarction. If doctors do not intervene in time, necrosis of the intestinal walls may begin, and saving a person will not be easy - the mortality rate reaches 70%. What kind of disease is this, what are its symptoms?
In the human body there is a special fold of the peritoneum - the mesentery. It holds the intestines together. Its vessels are called mesenteric. Each of them supplies a specific area of the intestine. Like any blood vessels, they can become clogged with blood clots.
If blood circulation in them is disrupted, a person develops a dangerous disease - thrombosis of mesenteric vessels, which is also called intestinal infarction. It threatens a person’s life, because doctors cannot immediately make the correct diagnosis, especially at the beginning of the disease, and provide the necessary assistance.
The disease is diagnosed in both men and women. Middle-aged or elderly people are most often affected.
Acute vascular diseases of the intestines (K55.0)
This subheading includes: 1. Acute:
– fulminant ischemic colitisColitis – inflammation of the mucous membrane of the colon;
– intestinal infarction;
– ischemiaIschemia is a decrease in blood supply to an area of the body, organ or tissue due to weakening or cessation of arterial blood flow. small intestine.
2. Mesenteric, [arterial, venous]:
– embolismEmbolism is blockage of a blood vessel by an embolus (a substrate circulating in the blood that is not found under normal conditions);
- heart attack; - thrombosis.
3. Subacute ischemic colitisColitis is inflammation of the mucous membrane of the colon.
from this subcategory :
– “Necrotizing enterocolitis in the fetus and newborn” – P77;
– “Embolism and thrombosis of the abdominal aorta” – I74.0;
– “Embolism and thrombosis of other arteries” – I74.8; – “Embolism and thrombosis of unspecified arteries” – I74.9.
Mobile application “MedElement”
Download the application for ANDROID
Mobile application “MedElement”
Download the application for ANDROID
1. Occlusive mesenteric arterial ischemia (OMAI): 1.1. Acute mesenteric arterial embolus (AMAE); 1.2.
Acute mesenteric arterial thrombosis (AMAT). 2. Nonocclusive mesenteric ischemia (NOMI).
3.
Mesenteric venous thrombosis (MVT).
Causes leading to the development of acute intestinal ischemia
1. Occlusive causes (embolism and thrombosis of the mesenteric arteries) are the main pathophysiological mechanisms for the development of acute intestinal ischemia. More often affected is the superior mesenteric artery, which is responsible for the blood supply to the small intestine, cecum, ascending and, partially, transverse colon.
The inferior mesenteric artery is responsible for supplying blood to part of the transverse and completely descending colon, as well as the sigmoid and rectum. Since the inferior mesenteric artery has anastomoses with the celiac artery, with its lesions a less obvious clinical picture is observed.
1.1. Embolism – occurs in approximately 50% of cases of acute intestinal ischemia. Embolism occurs mainly as a result of blood clots migrating from the heart through the bloodstream. Thrombi form on artificial valves, as well as due to atrial fibrillation, parietal thrombosis of the left ventricle after a heart attack, mitral stenosis, endocarditis.
In rare cases, emboli may consist of particles of atherosclerotic plaques, which may be displaced into the mesenteric artery basin during arteriography or surgery (for example, resection of an aortic aneurysm). Emboli are prone to fragmentation and displacement into the distal segments of the vessel, which causes a segmental type of intermittent ischemia.
1.2. Thrombosis of mesenteric vessels is the main cause of acute intestinal ischemia in 25% of cases. The thrombotic type develops directly in the mesenteric arteries as a result of acute arterial thrombosis of the proximal segment of the vessel (most often the mouth of the superior mesenteric artery) against the background of heart failure, hypercoagulation, trauma, pancreatitis, and tumor processes.
Also predisposing to thrombosis are aortic aneurysm, aortic dissection, arteritis, dehydration, smoking and diabetes.
2. Non-occlusive causes (cause less than 20% of acute intestinal ischemia): 2.1 Atherosclerosis is the main cause of acute ischemia. 2.2 Compression of vessels from the outside by a volumetric process, low cardiac output and perfusion pressure associated with congestive heart failure, acute myocardial infarction, shock of various origins, hypovolemia, and a sharp iatrogenic decrease in blood pressure.
2.3 Drugs (digitalis, ergotamine, vaspressors, cocaine) can also cause ischemia as a result of vasoconstriction (spasm).
3. Venous thrombosis – is the cause of acute intestinal ischemia in less than 10% of cases. The occurrence of venous thrombosis in 80% of cases is due to the following reasons:
– hypercoagulability (deficiency, imbalances or abnormalities of coagulation factors): polycythemia vera (the most common cause), thrombocytosis, sickle cell anemia, pregnancy, use of oral contraceptives; – neoplastic processes causing compression of veins or hypercoagulation (paraneoplastic syndrome); – infections, usually intra-abdominal localization (for example, appendicitis, diverticulitis or abscess); – venous congestion due to liver cirrhosis (portal hypertension); – venous injuries due to accidents or surgical interventions, especially portocaval anastomoses; – increased intra-abdominal pressure when performing pneumoperitoneum for laparoscopic operations; – pancreatitis; – decompression sickness.
Subsequently, three pathogenetic stages are realized sequentially: ischemia, infarction, peritonitis (some authors also distinguish the stage of functional intestinal obstruction). The implementation of the stages depends on the variant of the course: with compensation of blood flow, with subcompensation of blood flow, with decompensation of blood flow.
Note
1. Researchers found a significantly higher risk of acute mesenteric ischemia in patients with inflammatory bowel disease (hazard ratio 11.2, P
Source: https://diseases.medelement.com/disease/%D0%BE%D1%81%D1%82%D1%80%D1%8B%D0%B5-%D1%81%D0%BE%D1% 81%D1%83%D0%B4%D0%B8%D1%81%D1%82%D1%8B%D0%B5-%D0%B1%D0%BE%D0%BB%D0%B5%D0%B7 %D0%BD%D0%B8-%D0%BA%D0%B8%D1%88%D0%B5%D1%87%D0%BD%D0%B8%D0%BA%D0%B0-k55-0/ 4700
Localization and stages of the disease
Intestinal infarction develops when any part of the vessels of this organ is blocked, but most often occlusion of the trunk or mouth of the superior mesenteric artery occurs. Doctors divide this trunk into 3 parts. When each of them is affected, a specific part of the intestine is affected.
- Blockage of the first segment. Thrombosis of the small and cecum, the right half of the small intestine.
- Blockage of the second segment. The entire ileum and part of the jejunum are affected. Sometimes blind and ascending thick.
- Blockage of the third segment. Only the ileum is affected.
The stages of development of the disease are as follows:
- Ischemia. There is not complete, but partial bleeding of the walls of blood vessels. Later it is possible to restore blood circulation.
- Heart attack. Changes occur in the tissues of the abdominal cavity, and symptoms of intoxication appear.
- Peritonitis. Intoxication increases, the peritoneum becomes inflamed.
Causes
Intestinal infarction may be a consequence of atherosclerosis of the mesenteric vessels. The disease results in the formation of a plaque that interferes with blood flow. But most often this is an unpleasant consequence of various heart diseases in which a blood clot forms. This could be cardiosclerosis, cardiac aneurysms, myocardial infarction, etc.
So, in a person who has survived a myocardial infarction, the heart muscle ruptures. It is accompanied by bleeding. A blood clot forms at the site of injury. When blood clots break off, they can “travel” through arteries and veins. If this clot reaches the mesenteric vessels, they become clogged, and thrombosis of the mesenteric vessels is diagnosed.
Internal bleeding also occurs with other diseases, and each of them can cause thrombosis. Sometimes the vessels are compressed by a tumor, or the disease develops due to injury.
Pathways for blood clots to enter the mesentery
Movement of a blood clot through the arterial system:
From the heart - when an aortic aneurysm, resulting from a heart attack, is torn from the wall;
From the thoracic or abdominal aorta - in case of vessel dissection;
Detachment of an atherosclerotic plaque;
Directly from the mesenteric artery - as a result of its damage as a result of trauma (for example, a blow to the stomach).
Formation of a blood clot in the venous system:
Inflammatory bowel pathologies affecting veins (thrombophlebitis);
Decreased blood pressure due to deterioration in the activity of the heart muscle;
Portal hypertension as a complication of hepatitis;
Blood stagnation due to portal vein thrombosis;
Diseases and conditions that increase blood viscosity - consequences of splenectomy, long-term use of hormonal oral contraceptives, pathologies of the hematopoietic organs.
With a heart defect characterized by communication between its chambers, a thrombus can enter the mesenteric arteries from the vessels of the leg through the vena cava, right atrium, left ventricle, and abdominal aorta.
Symptoms
Symptoms of the disease immediately make themselves felt; the disease begins acutely.
However, this thrombosis also has a prodromal period, which can last 1-2 months. These symptoms are observed in patients who have vasoconstriction:
- occasional abdominal pain;
- the stomach is bloated;
- the patient feels nauseous and sometimes vomits;
- stomach hurts every time after eating;
- the chair is unstable.
- Ischemic stage (lasts 6-12 hours). Thrombosis of intestinal vessels in case of acute onset makes itself felt with severe pain. The patient begins to scream, rush about, and cannot find a place for himself. It is impossible to relieve this pain even with narcotics, but antispasmodics provide some relief. The following symptoms will also help to recognize intestinal thrombosis: the patient’s skin is pale, with a bluish tint;
- pulse is rare;
- blood pressure rises;
- the stomach is soft;
- tongue is wet;
- nausea, vomiting;
- Many people experience diarrhea with blood, but there may also be constipation (in a quarter of patients).
- The pain gradually subsides, because necrosis of the intestinal walls has already begun, and pain receptors have died.
- dry tongue;
Intestinal thrombosis without medical assistance leads to the death of the patient. If it was arterial thrombosis, the person will die after 2 days, if it was venous - after 5-6 days.
Diagnosis and treatment
The danger of this disease is that the symptoms in the early stages are similar to other abdominal diseases, of which there are many. Most often it is confused with appendicitis. How is an accurate diagnosis made?
- They take a blood test. If the number of leukocytes in the blood increases, this confirms the diagnosis.
- They take an x-ray. Thanks to it, the development of acute intestinal obstruction is determined. This symptom may suggest intestinal thrombosis.
- Angiography is performed. This is the most reliable diagnostic method. A radiopaque substance is injected into the artery, thanks to which an X-ray examination of the circulatory system can be performed.
The doctor may prescribe other, additional tests.
Treatment
Intestinal thrombosis is a life-threatening disease. Therefore, it is important to seek help from a doctor in the first hours of illness. If the patient was able to get to the hospital on time and was immediately diagnosed correctly, then conservative treatment without surgical intervention is possible.
The doctor will prescribe intravenous medications that will dissolve the blood clot and restore impaired bleeding. But such treatment is the exception rather than the rule, since it is not possible to quickly make a diagnosis: the patient is examined, excluding other diseases (pancreatitis, cholecystitis, appendicitis, etc.).
Therefore, there is often only one option left - surgery. If necrosis has not yet occurred, the surgeon removes the thrombus, part of the vessel, and performs artery replacement. If you did not manage to intervene in time, you have to remove the affected part of the intestine. However, it is not always possible to save the patient. Mortality is very high, with necrosis of the intestinal wall - up to 70%.
Mesenteric thrombosis is a dangerous disease that can only be cured with timely consultation with a doctor. Therefore, if you experience any pain in the abdominal area, it is important to immediately call an ambulance, otherwise time will be lost. Every minute increases the likelihood of the patient’s death, because after a few hours, medical assistance may be useless.
Mesothrombosis of intestinal vessels: causes, forms, course, diagnosis and therapy
Have you been struggling with HYPERTENSION for many years without success?
Head of the Institute: “You will be amazed at how easy it is to cure hypertension by taking it every day.
Intestinal vascular thrombosis is not a disease of young people; it affects middle-aged and elderly people. This is explained by the fact that atherosclerotic changes in the vascular walls develop and progress throughout life. Intestinal infarction, acute arterial or venous insufficiency are pathological conditions that have different etiologies and development mechanisms, but lead to acute disorders of the blood supply to the intestinal tract. The two main types of circulatory disorders (arterial and venous) can form a mixed form, which occurs in particularly advanced cases.
Impaired blood supply to the intestines
With mesenteric thrombosis, in approximately 90% of cases, the superior mesenteric artery, which supplies blood to most of the intestine (the entire small intestine, cecum, ascending colon, 2/3 of the transverse colon and hepatic angle), is affected, therefore the disorders here are the most severe. The share of lesions of the inferior mesenteric artery, which supplies blood to 1/3 of the transverse colon (left), descending colon and sigmoid, accounts for about 10%.
Our readers successfully use ReCardio to treat hypertension. Seeing how popular this product is, we decided to bring it to your attention. Read more here...
Acute mesenteric arterial insufficiency (AMI) can be of organic origin, resulting in occlusion of the great vessels, or of a functional nature, in which no changes in the lumen are observed.
In cases of organic lesions, the lumen of the mesenteric vessels is blocked primarily and the cause of this is trauma and embolism. Secondary overlap occurs as a result of thrombosis, which, in turn, was the result of long-term progressive changes in the vascular wall or outside it.
The most severe forms of impaired blood supply to the intestinal tract are embolisms and injuries of mesenteric vessels, which is explained by the lack of previously prepared developed collateral blood flow, and, consequently, the lack of compensation for the disturbed main blood flow.
Causes of primary disturbance of arterial blood flow
The causes of embolism are directly related to heart disease:
- Mitral valve stenosis;
- Heart rhythm disturbances;
- Cardiac aneurysm;
- Myocardial infarction, in which there is a marked decrease in the contractility of the left ventricle. An embolus (blood clot) in this case is formed as a result of increased blood clotting due to a disturbance in the speed of blood flow. A blood clot in the mesenteric arteries comes from the aorta, but sometimes it can form in the mesenteric vessel itself, although very rarely.
Injuries to the mesenteric arteries can lead to their complete rupture (a blow to the abdomen), which results in exfoliation of the intima, which, in turn, can completely or critically block the lumen.
Secondary occlusion of mesenteric arteries
The causes of secondary mesenteric insufficiency are the following pathological conditions:
- Stenosis of atherosclerotic origin (most often) at the mouth (place of origin) of arteries, because a large vessel departs from the aorta at an acute angle, creating conditions for the occurrence of turbulent blood flows. With a sharp decrease in blood flow, which happens when the artery narrows by more than 2/3 (considered a critical indicator), thrombosis of the mesenteric vessels is possible. Similar events occur when an atherosclerotic plaque ruptures or is damaged with complete obstruction (closure) of the lumen of the vessel. This will inevitably entail necrosis of the tissues that this vessel provides with blood, therefore atherosclerosis of the mesenteric arteries accounts for the largest percentage of cases of intestinal vascular thrombosis;
- Tumors, rudiments of the peduncle of the diaphragm and fibers of the celiac plexus, which lead to compression of the artery;
- A drop in cardiac activity with a pronounced decrease in blood pressure;
- Surgical (for the purpose of reconstruction) interventions on the aorta, the reason for which was its blockage - steal syndrome. When a blood clot is removed, blood begins to rush into the lower extremities at high speed, partially bypassing the mesenteric arteries and at the same time “sucking” blood from them into the aorta. In conditions of mesenteric obstruction, multiple thromboses with intestinal necrosis or intestinal infarction with subsequent perforation develop, while the main trunks of the mesenteric artery may not thrombose.
The etiological factors of acute mesenteric thrombosis of the intestine, or rather its arteries, can be different, but the mechanism for the development of pathological changes is always the same - intestinal ischemia.
Forms of intestinal ischemia
The clinic of intestinal ischemia differs in 3 degrees of severity, which are directly dependent on the diameter of the damage to the main arteries and collateral blood flow:
- Decompensated ischemia is the most severe form of damage to arterial vessels, in which irreversible effects can quickly occur if the time to restore blood flow is missed. It is characterized by absolute ischemia (decompensation of the intestinal blood supply disorder) and occurs in 2 phases. A period of time up to 2 hours is considered a phase of reversible changes. A phase lasting 4-6 hours is not always reversible; the prognosis can become unfavorable overnight, since after this time gangrene of the intestine or part of it inevitably occurs and then restored blood flow no longer solves the problem;
- Subcompensated disruption of the blood supply to the intestine provides collateral blood flow and in this case the symptoms of thrombosis of the intestine (its vessels) resemble the chronic form of mesenteric arterial insufficiency;
- The compensated form is chronic intestinal ischemia, when collaterals completely take care of the main blood flow.
Clinical manifestations of intestinal vascular thrombosis
Symptoms of intestinal thrombosis depend on the height of the overlap of the mesenteric artery and the form of ischemia:
- Sudden, rather intense pain is most characteristic of the subcompensated form of ischemia, although with decompensation of the blood supply disorder it also occurs, but soon weakens due to the death of nerve endings (at the site of the intestinal lesion and in the mesentery itself), which cease to signal trouble in the body (imaginary improvement );
- Intoxication caused by intestinal gangrene is especially characteristic of decompensated ischemia and is manifested by a thready pulse, unstable blood pressure, significant leukocytosis and vomiting;
- The phenomena of peritonitis (pronounced tension of the abdominal wall reminiscent of a perforated gastric ulcer) are most characteristic of thrombosis of the small intestine (superior mesenteric artery) in the case of the development of gangrene and intestinal perforation, which often occurs against the background of decompensated and subcompensated ischemia;
- The disappearance of intestinal motility (with intestinal necrosis) is inherent in decompensated ischemia, while in subcompensated ischemia, on the contrary, it has high activity and clarity;
- Passage disorder (frequent loose stools) and intestinal colic accompany the compensated form, with an admixture of blood - subcompensated ischemia. Due to the cessation of peristalsis in decompensated circulatory disorders, an enema (blood in the stool) is necessary to evaluate stool.
It should be noted that before the development of thrombosis of the intestinal arteries, it is possible to establish a diagnosis of acute mesenteric arterial insufficiency. The following signs may indicate impending thrombosis of mesenteric vessels:
- Abdominal pain that gets worse after eating or walking for a long time;
- Unstable stool (constipation, diarrhea, their alternation);
- Weight loss (may indirectly indicate the onset of a stenotic process at the mouth of the mesenteric artery).
Embolism of the superior mesenteric artery, on the contrary, is characterized by the absence of this symptom complex.
Diagnosis of mesothrombosis
With the correct diagnostic approach, it is possible not only to determine the disorder of the intestinal blood supply itself, but also the reasons that caused it. In this regard, collecting anamnesis and asking the patient about the course of the disease plays an important role. Clarifying the time of onset of pain, its intensity, and the nature of stool can significantly help the doctor in choosing surgical treatment, since there is still no other alternative in the case of mesothrombosis.
Diagnosis of OMAN involves selective angiography, which makes it possible to determine the level and nature of artery blockage, which will also be important for providing emergency care, naturally, in the form of surgical intervention.
The laparoscopic method still remains decisive in any type of acute surgical pathology, where mesothrombosis is no exception. Rather, on the contrary, in case of a decompensated circulatory disorder, the surgeon has only 2 hours at his disposal, so it is clear that there is no need to delay the diagnosis. With the help of laparoscopy, it is possible to clarify the nature of the damage to the intestinal tract within a short time.
Only a radical method that cannot be postponed
Conservative treatment of intestinal thrombosis, that is, the mesenteric arteries that supply it with blood, is unacceptable, however, mesenteric insufficiency can begin to develop suddenly, which is always aggravated by the total spasm of blood vessels that accompanies the disease.
With the active administration of antispasmodics, it is possible not only to alleviate the patient’s suffering, but also to transform a more pronounced degree of ischemia into a less severe one. However, the progression of mesothrombosis leads to the blocking of important collaterals, which significantly aggravates the patient’s condition, due to the fact that they cease to compensate for the blood supply. If we proceed from this position, then a violation of the blood supply to the intestines in each specific case may have its own “surprises”, which very significantly affect the outcome of the surgical intervention.
Emergency care in the form of surgical treatment of mesenteric thrombosis is the only way to save a human life, however, the general set of measures provides for intensive preoperative preparation, which corrects disturbances of central hemodynamics.
Surgery for intestinal thrombosis consists of the required components:
- Inspection of the intestine and palpation of the mesenteric vessels, starting from the mouth;
- Determination of pulsation in the mesenteric arteries at the borders of the affected intestine, where in cases of doubt, dissection of the mesentery is considered appropriate (establishing arterial bleeding).
The actual liquidation of OMAN may include the following methods of carrying out the operation:
- Complete restoration of blood flow in the absence of intestinal necrosis;
- Improving blood supply to the subcompensation site in case of bowel changes;
- Resection of the changed intestine.
In order to improve or restore blood supply, reconstruction of the great arteries or embolectomy is used, which is considered a fairly effective method. In this case, the surgeon can “milk” the embolus with his own fingers.
Reconstructive surgery in the form of direct intervention in the area of stenosis and thrombosis or the creation of a shunt between the mesenteric artery and the aorta below the level of stenosis and thrombosis (less traumatic) is performed in case of blockage of the artery lumen by a thrombus and is carried out according to emergency indications. The gangrenous intestine is cut off from healthy tissue and removed, but in this case, great importance is attached to restoring blood flow, because by limiting only to resection, the doctor always risks losing the patient (this situation results in up to 80% of deaths).
In addition, in the postoperative period, in addition to a set of generally accepted measures, patients are prescribed anticoagulants (heparin). However, if blood flow is not restored, then it becomes necessary to use high doses of heparin. This is fraught with such consequences as failure of the anastomotic sutures, which occurs due to the fact that the level of fibrin, the task of which is to glue the peritoneum, drops sharply.
Video: mesenteric ischemia - diagnosis, explanation and surgery
Thrombosis of mesenteric veins and mixed form of acute circulatory disorder
The cause of acute mesenteric venous insufficiency (AMVI) is most often thrombosis of venous vessels, involving an entire segment of the intestinal mesentery. This is usually due to an excessive increase in blood coagulation and impaired peripheral and central hemodynamics.
The clinical picture of intestinal venous thrombosis has the following symptoms:
- Severe pain localized in a specific area of the abdomen;
- Frequent loose stools mixed with blood or bloody mucus;
- The phenomena of peritonitis appearing as necrotic changes in the intestine develop.
Diagnosis is based on history, clinical picture and laparoscopic examination.
Treatment consists of removing the affected intestine within healthy tissue.
The prognosis for venous thrombosis, in contrast to arterial blood supply disturbances, is favorable. The intestinal loops, while continuing to be supplied with arterial blood, are completely affected very rarely.
The mixed form, in which thrombosis of an arterial vessel occurs simultaneously in one segment of the intestine and a venous one in another, is considered in its pure form to be an extremely rare phenomenon, which is usually detected during surgery.