RH FACTOR
(rhesus - after the name of the monkey species Macacus rhesus) is a system of allogeneic human blood antigens, independent of the factors that determine blood groups (AB0 system) and other genetic markers.
R.-f. human was discovered in 1940 by K. Landsteiner and A. Wiener. The antigen system received the name “Rh factor” due to the fact that its antigen was discovered in humans using rabbit serum immunized with red blood cells from a monkey of the species Macacus rhesus. R.-f. most expressed in erythrocytes. It is less clearly represented in leukocytes and platelets. In blood plasma R.-f. Not found.
There are six main antigens of R.-f. To designate this system of antigens, two nomenclatures are used equally: the Wiener nomenclature and the Fischer-Reis nomenclature. According to the first, antigens of R.-f. denoted by the symbols Rh0, rh', rh", Hr0, hr', hr"; according to the second, they use letter designations: D, C, E, d, c, e. They often use two nomenclatures at the same time. In this case, the symbols of one of the designations are placed in brackets. A large number of antigen variants in R.-f. allowed Rosenfield (R. E. Rosenfield) et al. in 1962 to propose a new digital nomenclature for the designation of R.-f. It included Rh antigens from Rh 1 to Rh 35.
Synthesis of antigens R.-f. controlled by genes of the first pair of chromosomes. The presence of R.-f. in erythrocytes. encoded by six genes linked in groups of three on one chromosome. The pairs of genes that control the antigens D—d, C—C, and E—e are allelic, since each individual contains six genes that control the synthesis of R.-f. However, fewer antigens may be detected phenotypically (five, four, three), depending on the number of tomozygous loci in the individual.
Antigen (factor) Rh0(D) is the main antigen in R.-f., and has the greatest practical significance. It is found in the red blood cells of 85% of people living in Europe. The Rh0(D) antigen is not homogeneous; it includes a number of smaller subunits - RhA, RhB, RhC, RhD, due to the differences of which hemolytic disease of newborns sometimes develops (see) in Rh-positive mothers.
Based on the presence of Rh0(D) antigen in erythrocytes, Rh-positive blood is isolated. Human blood, erythrocytes lacking this antigen, is classified as Rh-negative. They approach donors with Rh-negative blood differently. Their red blood cells should not contain any of the three antigens - Rh0(D), rh'(C), rh"(E). This approach to assessing the Rh status of donors eliminates the possibility of recipient sensitization to these antigens and significantly reduces the risk of post-transfusion complications. The Rh0(D) antigen in 1.5% of cases occurs in a weakly expressed genetically determined variant - the Du variety. The Rh0(D) antigen is unevenly distributed among representatives of individual races. As you move from west to east, the frequency of its presence changes significantly. In the European population, the frequency of occurrence of persons with Rh-negative blood type is 15%, and in Mongoloid races it is approx. 0.5%. The overwhelming number of Asian residents are carriers of the Rh0(D) antigen, therefore, among pregnant women, immunological conflicts according to R.-f. are less common than among pregnant women of the European population.
Allelic to the Rh0(D) antigen gene is the Hr0(d) antigen gene. The existence of the Hr0(d) antigen has not been proven, since the corresponding antiserum has not been obtained for it. The expected frequency of occurrence of this antigen in the European population is ca. 63%
The second pair of antigens controlled by allelic genes includes the rh'(C) and hr'(c) antigens. The rh'(C) antigen was discovered by A. Wiener in 1941 using blood serum obtained from a patient with a hemolytic reaction that occurred after a blood transfusion. Its occurrence frequency is about 70%. There are several variants of this antigen (Cw, Cx), differing in severity. The rare occurrence of these variants (Cw - 2.5, Cx - 0.001%) determines their low significance. The hr'(c) antigen was discovered two years later using the blood serum of a Rh-positive woman who gave birth to a child with hemolytic jaundice. The frequency of occurrence of hr'(c) is approx. 80%.
The third pair of antigens, the synthesis of which is controlled by allelic genes, consists of the rh"(E) and hr"(e) antigens. The rh antigen (E) was discovered by A. Wiener in 1943. The frequency of occurrence of the antigen is approx. 30% among the European population. The hr"(e) antigen was discovered by AE Mourant in 1945. The frequency of occurrence of this antigen is approx. 97%. M.A. Umnova (1976) notes the following frequency of occurrence of R.-f. antigens. among Russians: Rh0(D) - 85.03%, rh'(C) - 70.75% „ rh"(E) - 31.03%, hr'(c) -84.04%, hr"(e ) — 96.76% .
Very rarely, human blood does not give positive results with any blood serum against R.-f. antigens. Red blood cells of such blood are designated Rh NULL. Rh NULL red blood cells resemble the Bombay blood type, lacking all ABO system antigens (see Blood Groups). It is generally accepted that persons with Rh NULL red blood cells have the Xr0 gene in a homozygous form, which represses the production of R.-f antigens. Such persons can transmit R.-f. antigens to children without phenotypically showing these signs themselves. The presence of the Xr0 gene indicates pathology, since in individuals with Rh NULL red blood cells, disorders of the red blood cell membrane are often observed, causing their rapid destruction.
One of the varieties of R.-f. is the LW antigen, so named after the researchers K. Landgeiner and A. Wiener, who discovered it. The LW antigen is detected mainly by heteroimmune blood sera obtained from guinea pigs against the erythrocytes of Macacus rhesus monkeys. The antigen is found in 99% of people, regardless of their Rh status. The LW antigen includes the Rh0(D) antigen. Therefore, anti-LW sera, after adsorption by Rh-negative erythrocytes, acquire the specificity of anti-Rh0(D).
Antibodies against R.-f. (see Antibodies), usually immune. Determination of anti-Rhesus antibodies is carried out using the hemagglutination method (see). The reaction uses human erythrocytes of known affiliation according to R.-f. This also makes it possible to determine the specificity of antibodies. In addition, the quantitative characteristics of antibodies are determined by the titer of the blood serum being tested. To do this, determine the last dilution of the blood serum being tested, which still shows a positive result. The main reason for the formation of anti-Rhesus antibodies is allo- less autosensitization (see Autoallergy). Anti-D, anti-C, and anti-E antibodies are most often formed.
There are two types of Rh antibodies: complete and incomplete. Complete anti-Rh antibodies have the ability to stick together Rh-positive red blood cells. They do not pass through the intact placenta, are predominantly IgM, are less common than incomplete ones, and therefore have less importance in medicine. Incomplete anti-Rh antibodies have the ability to agglutinate Rh-positive erythrocytes only in the presence of colloidal solutions (substances with a large molecular weight), after treatment with proteolytic enzymes or with the addition of specially prepared antiglobulin serum (see Coombs reaction). They are more common. than full antibodies. Their molecular weight is much smaller, due to which they penetrate the placental barrier more easily and are therefore more aggressive. Partial anti-Rhesus antibodies belong mainly to IgG. Autoimmune antibodies are, as a rule, incomplete antibodies against Rh0, hr" and other R.-f. antigens; relate mainly to IgG.
In simple words: what is blood group and Rh?
All people have approximately the same blood composition , which is determined by a basic set of elements.
However, there are eight different types of blood, called groups. They are distinguished based on a description of the individual characteristics of red blood cells. Blood types are determined by certain molecules called antigens. These molecules are arranged in combinations that are determined by genetic information and inherited from parents. There are four blood groups based on the type of antigens and two other groups, depending on the presence or absence of the Rh factor.
The protein found on the surface of red blood cells is called the Rh factor. If a person has this protein in his body, he is considered Rh positive. Accordingly, if the protein is missing, the person is defined as Rh negative.
The presence or absence of this protein does not depend in any way on blood type .
It is an immunological trait, it is inherited and remains the same throughout life, it is an individual genetic characteristic, just like skin tone or hair color.
Determination of Rh factor
The Rh factor can be determined using:
- anti-Rhesus serum (express method);
- zoliclone anti-D super.
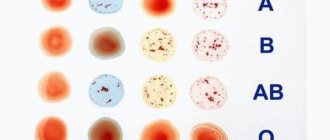
For testing using standard anti-Rhesus serum, the patient's blood or red blood cells obtained from it can be used. Standard anti-Rhesus serum is dripped into a test tube, then a drop of the patient's blood or red blood cells is injected. The test tube is rotated in your hands so that the blood mixes with the serum. A little saline solution is also added to the test tube. The results are assessed by the presence/absence of agglutination:
- Present – Rh positive.
- Absent – Rh negative.
The anti-D super zoliclone assay is performed on a plate. A reagent is applied to it, and a drop of blood is placed next to it. The plate is rocked so that the materials come together. Then, as in the previous method, the presence or absence of an agglutination reaction is assessed.
Rh factor: negative and positive
About 85% of all inhabitants of the planet have a positive Rh factor. The presence or absence of antigen D does not affect the patient’s well-being and health.
Rh species
Positive
According to statistics, about eighty percent of the population of our planet have a specific protein in their blood. People with a negative Rh factor are much less common. This is explained by the fact that Rh positive is a dominant trait, that is, if both parents have it, their children are likely to inherit this trait.
Negative
The absence of the Rh factor is associated with a certain gene , which is either carried on the chromosomes or not. If this gene is absent in the chromosomes of the mother and father, their child will be Rh negative. However, if the gene appears in at least one of the chromosome sets, the child will have Rh-positive status. Although there are much fewer Rh-negative people, they are practically no different from the rest.
Rules for decoding results
The results of the analysis are given to the patient in the following form:
- blood type (0, A, B, AB);
- Rh factor: Rh+ (positive) or Rh- (negative).
The results of the blood group test will remain relevant throughout your life. If the study has already been carried out, there is no need to repeat it again. Blood type is a “constant value” and a genetically inherited trait, that is, it does not change throughout life. Although once a young Australian Demi Leigh-Brennan changed her blood type after a liver transplant. But this case is an exception, and doctors have not been able to clearly explain this phenomenon.
Sometimes some patients claim that their blood type has changed due to some disease or during pregnancy. This can be explained by medical error. Both pregnancy and some pathologies can make it difficult to decipher test results, as a result of which they may turn out to be unreliable. There are cases that an error was made during a previous blood test.
How is it designated?
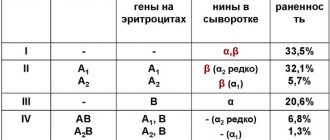
According to the accepted international system, there are four blood groups:
- A (or II) - antigen A is present.
- B (or III) - B antigen is present.
- AB (or IV) - has antigen A and B.
- 0 (or I) - contains neither antigen A nor antigen B.
The presence or absence of the Rh factor is indicated as follows:
- Availability – Rh +.
- Absence - Rh -.
Although the Rh factor remains unchanged throughout life, and modern medical devices are able to quickly and painlessly determine it, this does not exclude the occurrence of errors.
Errors can occur both due to the negligence of medical personnel and in the event of technical malfunctions. Some kidney and liver diseases can also distort test results . Therefore, you should take a second test to avoid unpleasant incidents.
Preparing for the study
No specific preparatory measures are required. However, it is recommended to eat food no later than 4 hours before blood sampling. Also, on the eve of the procedure, excessive physical activity should be avoided. It is better to come to the clinic in advance and sit quietly for 10-15 minutes before donating blood.
Since the results of the study can be influenced by certain diseases, the use of a number of medications, dietary habits and even the emotional state of the patient, it is recommended that the analysis be carried out twice to avoid obtaining unreliable results. You should provide your doctor with a list of all medications you are taking in advance.
Why is it important?
Rh status should definitely be taken into account when planning a pregnancy or in emergency situations when a person needs to become either a donor or a recipient of donated blood. Knowing your blood type and Rh status can save your life in a situation where minutes are counting and there is no time for tests.
The procedure for determining Rh is no different from taking blood for a general analysis; it is practically painless and takes only a few minutes.
When transfusing
The Rh factor is very important to consider when giving blood transfusions in order to avoid conditions called Rh conflict. The entry of Rh+ blood into the body of a patient with a negative Rh factor can lead to negative health consequences, including death. The recipient's body produces antibodies that attack foreign blood. If such a patient is given a repeated transfusion of inappropriate blood, this will lead to the destruction of red blood cells and transfusion shock.
Meaning
Differences between people according to R.-f. can lead to immunologically conflicting pregnancy (see Pregnancy, Immunological incompatibility). The basis of sensitization is the entry into the body of an Rh-negative woman of Rh-positive erythrocytes of the fetus, Ch. arr. through the vessels of the placenta.
The mechanism of development of Rh-conflict pregnancy is presented as follows. Immune antibodies formed in the body of a Rh-negative woman pregnant with a Rh-positive fetus, being predominantly incomplete IgG, penetrate the placenta into the fetus, causing hemolysis of the newborn's red blood cells and damage to its vital organs (hematopoietic tissue, liver, brain). Symptoms of immunological damage to a child are called hemolytic disease of the newborn. Due to extensive destruction of red blood cells, an increase in the amount of bilirubin, severe anemia with the release of a large number of erythroblasts into the blood, and a positive direct Coombs test are observed as a result of the presence of alloimmune antibodies on the fetal red blood cells. The main therapeutic measures to combat hemolytic disease of newborns are reduced to the rapid removal from the child’s body of the products of destruction of red blood cells. They primarily include exchange transfusions of Rh-negative blood. Other ways are also being developed in the fight against hemolytic disease of newborns - prevention of anti-Rh sensitization of Rh-negative women during the first pregnancy by administering anti-Rh gamma globulin.
Anti-Rhesus gamma globulin is prepared from the blood serum of an immune person containing anti-D(DC) antibodies in a titer of at least 1: 128-256. The introduction of anti-Rhesus gamma globulin in a dose of about 300 mg in the first 48-72 hours from the moment of delivery prevents the development of sensitization during the next pregnancy to R.-f. in 90-100% of cases. A smaller dose of anti-Rh gamma globulin (100 mg) is used when performing artificial termination of pregnancy in an Rh-negative woman. The mechanism of the immunosuppressive effect of anti-Rhesus gamma globulin is not fully understood. It is known that passive induction of anti-Rhesus immunity in an Rh-negative woman reduces the circulation time in the blood and the destruction of Rh-positive fetal erythrocytes by macrophages and other cells. Apparently, antigens of R.-f. after combining with anti-Rhesus antibodies, they lose their immunizing activity or T-suppressor activation occurs (see Immunocompetent cells).
Antigens R.-f. are important in forensic medicine when conducting an examination to exclude paternity (see Disputed paternity).
Bibliography:
Agranenko V. A. and Skachilova N. N. Hemotransfusion reactions and complications, M., 1979; Gavrilov O.K. A manual on transfusiology, p. IZ, M., 1980; Dosse S. Immunohematology, trans. from French, M., 1959; Zotikov E. A. Human antigenic systems and homeostasis, M., 1982; Kosyakov P. N. Human isoantigens and isoantibodies in health and disease, M., 1974; Guide to general and clinical transfusiology, ed. B.V. Petrovsky, p. 114, 216, M., 1979; Guide to the use of blood and blood substitutes, ed. A. N. Filatova, p. 86 and others, L., 1973; Solovyova T. G. Rh factor and its significance in clinical practice, L., 1963; Tumanov A.K. and Tomilin V.V. Hereditary polymorphism of isoantigens and blood enzymes in normal and pathological conditions in humans, M., 1969; Umnova M. A. et al. Isoimmunology and issues of blood transfusion complications, M., 1979; Allen FH a. R o-senfie 1 d RF Review of Rh serology, Haematologica, v. 6, p. 113, 1972; American hospital supply corporation, Dade division, Blood group immunology, theoretical and practical aspects, p. 47, Miami, 1976; G i b-1 ett EH Genetic markers in human blood, Philadelphia, 1969; I ssitt PD, Pavone BG a. Shapiro M. Anti-Rh39 - a “new” specificity Rh system antibody, Transfusion, v. 19, p. 389, 1979; Landsteiner K. a. Wiener AS Agglutinable factor in human blood recognized by immune sera for rhesus blood, Proc. Soc. exp. Biol. (NY), v. 43, p. 223, 1940; M o 1 1 is o n PL Blood transfusion in clinical medicine, Oxford, 1979; Race RR a. Sanger R. Blood groups in man, Oxford, 1975; Rosen-field RE ao A review of Rh serology and presentation of a new terminology, Transfusion, v. 2, p. 287, 1962; Z mievskij S. M. Immunohematology, NY, 1978.
E. A. Zotikov.
Pregnancy in cases of Rh incompatibility
The occurrence of an Rh conflict during the first pregnancy is unlikely: the baby's bloodstream is separated and protected from the mother's bloodstream. However, during the birth process this protection is disrupted, and mixing of the blood of different Rh factors can occur.
If this happens, and foreign blood enters the mother’s body, the likelihood of a conflict increases in subsequent pregnancies: if the second child also inherits the father’s Rh condition, the pregnant woman’s body will begin to produce antibodies much faster. This immune reaction is called sensitization (accumulation of a substance in the body, with the possibility of subsequent manifestation of an allergy to it).
Features of blood
Owners of the first blood group do not have agglutinogens, and the peculiarity of this group is versatility. The first group is suitable for each transfusion recipient. The fourth blood group contains an agglutinogen and does not have the ability to glue non-native red blood cells in the plasma.
Modern doctors have learned to perform blood transfusions of all groups and have reliably become familiar with the uniqueness of each of them. There is a certain definition scheme that helps to find out the group and rhesus belonging to the plasma. The developed serum, which reacts in a certain way when mixed with the sampling material, indicates the characteristics of a particular plasma.
Blood group determination scheme
Doctors refuse to use the universal characteristics of blood during transfusion and try to transfuse identical groups and Rhesus. Only in extreme cases do they violate generally accepted rules. This mainly applies to moments when emergency help is needed, but there is no time to select a donor. But even then there are rules that cannot be violated. So, those with the second (2) blood group can be transfused with the second and fourth, the third with the third and fourth, the fourth with only the fourth, and the first is suitable for everyone.
In addition to erythrocytes, group antigens are found in leukocytes, platelets, saliva, sperm, bile, gastric juice, and tissues. This is vital not only for transfusion, but also for transplantation of the heart and other organs and tissues. Compatibility of the donor group is necessary for the further success of the operation.
Inheritance
In the genetic code of each person there are two genes responsible for Rh-ness. They are inherited from both parents. Each of these two genes will either turn out to be a gene for the presence of Rhesus, or a gene for its absence. There are only three possible combinations:
- either the person is Rh positive;
- or Rh negative;
- or he is only a carrier of the negative Rh gene, which can appear in his children.
Since the gene responsible for the absence of Rh is recessive, an Rh-negative child is most likely to be born to the corresponding parents.
If the genetic background of the parents is different, then, with a probability of about seventy percent, a Rh-positive child will be born, which is impossible if both parents do not have a special protein on the surface of their red blood cells. It should be taken into account that the same parents can have children with different Rhesus characteristics .
Although Rh is only a manifestation of individual hereditary characteristics, awareness of it can save lives in an emergency. The analysis required to determine it can be taken free of charge at a medical center, district clinic or blood donation point.
Antigens and antibodies
The Rh antigenic system, in addition to the main factor (Rh), contains other varieties, subsequently isolated by Fischer and Reis and designated: rh´, rh´´, Hr0, hr´, hr´´. Meanwhile, this nomenclature caused some confusion, so it was decided to switch to mixed designations for Rh antigens:
- Rh0 (D);
- rh´(C);
- rh´´(E);
- Hr0(d);
- hr´(c);
- hr´´ (e).
Antibodies corresponding to these antigens are written as follows:
- anti-Rh0 (D);
- anti-rh´ (C);
- anti-rh´´ (E);
- anti-Hr0(d);
- anti-hr´ (c);
- anti-hr´´ (e).
Thus, the Rh system is represented by 6 antigens (D, d, C, c, E, e), the combination of which determines the Rh phenotype, numbering 18 combinations (to simplify perception, only letter designations are often used) and 6 types of directional ones (anti-D, anti-C, anti-E, etc.) immunoglobulins (M and G),
the Rh does not have
natural antibodies .