Inferior vena cava syndrome is one of the most severe stages of venous insufficiency regarding the clinical course and outcome of the disease. Diseases of the human cardiovascular system are now very “younger”. Unfortunately, they differ in a variety of forms and manifestations. The processes of blockage of blood vessels lead to a restriction of the flow of oxygen-enriched blood to the tissues, which provokes their oxygen starvation with subsequent disruption of trophism and degeneration up to gangrenous inflammation. The first symptoms of circulatory disorders can appear even at a fairly early age, and they cannot be ignored.
What is the inferior vena cava
The inferior vena cava is a wide vessel formed by the confluence of the right and left iliac veins in the human abdominal cavity. It is located at the level between the 4th and 5th vertebrae in the lumbar region. This is the widest vessel in the human body with a diameter reaching 4 cm. Penetrating the diaphragm, it enters the right atrium, collecting blood from neighboring veins and delivering it to the heart.
With the normal structure and operation of the inferior vena cava, it changes its parameters synchronously with the respiratory process. On inhalation, compression occurs, and on exhalation, expansion occurs. It is these signs that distinguish it from the aorta.
The inferior vena cava is responsible for collecting venous blood in the lower part of the human body. It is capable of concentrating up to 70% of the total venous blood circulating in the body.
Symptoms of superior vena cava syndrome
Depending on the cause of the syndrome, symptoms may develop slowly or quickly. Fast - for aggressive tumors such as malignant lymphoma and small cell lung cancer. Clinical signs gradually appear with metastases to the lymph nodes of cancer and venous thrombosis. The severity of the signs of superior vena cava syndrome depends on the level at which the vein is partially blocked and the degree of narrowing of its lumen.
At any rate of development of superior vena cava syndrome, there comes a time when it is impossible to do without emergency medical care.
Book a consultation around the clock +7+7+78
Until the middle of the last century, superior vena cava syndrome (SVVC), or to be precise, its compression syndrome, caused only tertiary syphilis, when gummas destroyed the wall of the thoracic aorta with the formation of aneurysmal sacs that compressed the mediastinal organs and the superior vena cava as well. Tertiary syphilis was eradicated with antibiotics, but since the beginning of the twentieth century, smoking has spread, and with it the incidence of lung cancer has increased a thousandfold, which became the main cause of an emergency condition caused by a violation of the blood circulation of a very large vein and the vessels flowing into it.
It is not known exactly how many people are affected by SVPV every year; medical statistics take into account only the etiological cause - lung cancer, but not its complications; however, in recent years, patients with SVPV are increasingly ending up in oncological intensive care due to the life-threatening severity of the condition. The majority of all diagnosed SVPVs are due to advanced lung cancer, with eight out of ten cases caused by a tumor in the right lung. If you look at the morphology, then predominantly venous syndrome initiates small cell lung cancer, less often squamous cell cancer, and very rarely adenocarcinoma. The last two are classified as non-small cell lung cancer.
In second place in terms of the frequency of induction of SVPV are oncohematological diseases - high-grade lymphomas or lymphosarcomas affecting the anterior mediastinum, most often lymphoblastic and diffuse large cell. As a rule, these are very aggressive tumors that grow in just a few days. The syndrome develops with metastases in the mediastinal lymph nodes of any cancer, but more often these are organs whose lymph collectors are located in the mediastinal tissue: the mammary gland, esophagus and stomach. Metastases of testicular germ cell tumors spread from the retroperitoneum to the supraclavicular zones mainly through the lymphatic tract, but they account for a small number of cases of SVST.
Vessel pathologies
Pathological conditions of the inferior vena cava are predetermined by a number of factors that subsequently give quite clear symptoms. It can be:
- tumor processes of the abdominal organs;
- vein compressions during pregnancy;
- inflammation of the lymph nodes;
- abdominal organ injuries;
- trophic ulcers on the lower extremities;
- constipation;
- a large accumulation of toxins in the intestines;
- portal vein thrombosis;
- peritoneal ascites;
- damage to the diaphragm;
- renal failure.
Inferior vena cava syndrome most often occurs in women during pregnancy, when polyhydramnios, a very large embryo, and arterial and venous hypotension occur. When the inferior vena cava is compressed by the uterus, normal blood flow to the kidneys, liver and uterus is reduced, which can have an extremely negative impact on the development of the embryo. Premature stratification of the placental tissue may occur, which will provoke thrombophlebitis and varicose veins on the lower extremities of a pregnant woman. This is a fairly common case encountered in medical practice.
Also during childbirth, especially when the gynecologist is forced to resort to caesarean section, there is a risk of collapse.
Thrombotic blockage of the inferior vena cava is considered one of the most severe forms of venous insufficiency that has a chronic course. This is a dangerous condition that can be fatal. This disease mainly affects the lower extremities.
The symptoms of this condition are very characteristic and increasing:
- pain in the groin area;
- abdominal pain;
- increased swelling of the legs;
- swelling of the buttocks;
- swelling of the genital organs;
- varicose veins of small vessels in the thighs;
- trophic ulcerations of the lower extremities;
- increased body temperature;
- impotence;
- lack of libido;
- hair loss on the head;
- fragility of nail plates;
- bone fragility;
- increased pallor of the skin;
- increased blood pressure;
- disturbances in motor functions when walking;
- difficulties when covering short distances on foot;
- deep vein thrombosis of the leg.
Causes of vein compression
The SVC is located between tissues and organs with a dense structure. It is surrounded by the inner surface of the chest, trachea, bronchial branches, aorta, and a chain of lymph nodes. The vein itself is a vessel with thin walls and low blood pressure. Therefore, with increased external pressure or blockage, it easily loses patency.
When the outflow is disrupted, venous congestion spreads to the brain, neck, arms and entire upper chest. Despite the presence of bypass paths - venous collaterals, they are not able to compensate for the functions of the main vein, since there is intense blood flow in these areas.
The main factors that lead to the formation of cava syndrome:
- extravasal (external, outside the vessel) pressure;
- germination of a tumor node into the wall of the SVC;
- blockage by a blood clot.
Pathologies that provoke the development of the syndrome include:
- lung tissue cancer;
- tumors of the lymph nodes (lymphogranulomas, lymphomas, metastasis from malignant neoplasms of the mammary gland, genital organs);
- benign processes, purulent inflammation of the thymus gland, trachea, esophagus;
- silicosis (occupational lung disease);
- compressive (constrictive) pericarditis;
- complications after radiation therapy (fibrous nodules, adhesions);
- aneurysmal dilatation of the aorta;
- enlargement of the thyroid gland (retrosternal goiter);
- tuberculosis and syphilitic infections;
- fungal infection of lung tissue (histoplasmosis).
The occurrence of cava syndrome is often noted after prolonged catheterization of a vessel or cardiac pacing.
We recommend reading the article about thrombophlebitis of the veins of the face and neck. From it you will learn about the causes of the disease, symptoms, methods of diagnosis and treatment.
And here is more information about internal varicose veins.
Treatment methods
In cases of dysfunction of the inferior vena cava caused by pregnancy or difficult childbirth, there is a chance for complete restoration of the functioning of the internal organs of the abdominal cavity and normalization of blood flow without the use of additional medications.
Drug therapy in such cases is aimed at thinning the blood, relieving pain syndromes, cleansing blood vessels, saturating the body with nutrients, and supporting the immune system.
We present several accessible simple folk methods of cleansing blood vessels here.
Infusion of rose hips. Mash the rose hips and pour in hot water, the temperature of which does not exceed 60 ºC, so as not to destroy the vitamins and microelements. Let sit for at least 30 minutes. Drink as tea in large quantities.
2 tbsp. l. clover flowers pour 500 ml of vodka. Leave for 2 weeks in a dark place at room temperature. Drink 1 tbsp at night. l. the resulting tincture for 2-3 months. The course can be conducted 2 times a year.
Pour 0.5 kg of peeled garlic into 1 liter of vodka. Infuse for 2 weeks in a dark room at room temperature. Take the resulting tincture 1 tsp. 3 times a day half an hour before meals.
Inferior vena cava syndrome: features, treatment, prevention
NVP is part of the circulatory system.
It is the largest vessel in the human body. There is no valve system. Venous blood circulates in the lumen of the vessel. It is sent to the right atrium for further distribution throughout the pulmonary circulation.
Thrombosis leading to compression of the ventricle veins causes circulatory disorders.
IVC syndrome is a blockage of a vessel for one reason or another.
According to statistics, the syndrome is diagnosed in most cases in women. This is due to reproductive function.
Where is it located and its functions
Originates from two iliac veins. Located behind the organs.
Formed at the level of 4-5 lumbar vertebrae on the posterior wall of the abdomen. The abdominal aorta passes on the left. Then it passes through the diaphragm, penetrating through a special opening, and flows into the pericardium.
The flap or Eustachian valve prevents venous blood from flowing back into the vein.
Functions:
- collection of waste blood from the pelvis, lower extremities and abdominal organs;
- delivery of blood to the heart muscle for further conversion;
- participation in the respiratory process - a distinctive feature from the aorta is the ability to expand during exhalation.
What is thrombosis of the inferior vena cava?
A pathological condition in which blood circulation is completely or partially disrupted. Compression of the lumen leads to stagnation - the walls of the blood vessel thicken.
Compression of the inferior vena cava is a rare phenomenon that becomes chronic.
IVC thrombosis is a dangerous condition that requires emergency hospitalization and medical care.
In most cases, it occurs in pregnant women and is associated with an enlarged uterus, which compresses the vein as the fetus grows.
An increase in pressure leads to blockage and is expressed by a sharp drop in blood pressure and fainting.
There are primary and secondary phases of IVC blockage.
The lesion can be observed on one of the vein segments and is classified according to the location of the thrombus:
- infrarenal;
- renal;
- suprarenal.
Causes
The underlying cause is unknown, but there are factors that increase the risk of thrombosis.
Provoking factors:
- pregnancy over 25 weeks of pregnancy.
- allergic processes;
- acute endocrine disorders;
- varicose veins;
- blood pathologies: increased coagulability, changes in biochemical composition;
- hereditary predisposition;
- less often: echinococcosis of the liver and tumors of the abdominal organs.
Inflammation of the venous wall with the formation of thrombophlebitis is also a provoking factor.
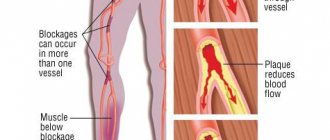
When a blood clot breaks off, blockage can occur in any vessel and the inferior vena cava is no exception.
Symptoms
Signs depend on the degree of compression of the venous lumen and the localization of the pathological process.
Thrombosis of the renal segment is characterized by the following symptoms:
- pain in the lumbar region and lower abdomen;
- nephrotic syndrome;
- uremia;
- a sharp increase in the amount of urea in a biochemical blood test;
- the appearance of protein in the urine.
Blockage of the liver segment is characterized by the presence of such signs as:
- swelling of the lower extremities;
- bruising;
- yellowness of the skin in the abdominal area;
- pronounced expansion of the veins of the chest and abdomen;
- pain syndrome.
At the beginning of the disease, the presence of “goosebumps” crawling from the legs is noted. The limbs gradually become numb.
Blood pressure rises, heart rate increases and a feeling of anxiety and restlessness appears.
Complications
The consequences and complications are variable. Depends on several factors:
- pregnancy;
- age;
- localization.
Compared to other causes of thrombosis, pregnancy occupies a leading position.
Poor blood circulation contributes to thrombosis and placental abruption.
Blockage of the kidney leads to serious problems.
Severe renal failure develops. If left untreated, death can occur.
Thrombosis of the hepatic segment: complications:
- hepatosplenomegaly;
- pressure on the fibrous membrane of the liver;
- increased risk of internal bleeding;
- jaundice.
Diagnostics
To identify the disease, a number of diagnostic procedures are carried out to determine the severity and localization of the process.
The main type of diagnosis is the use of instrumental methods:
- Phlebography or angiography is a type of X-ray diagnostic that allows you to determine the narrowed area;
- Doppler ultrasound;
- radiotracer method;
- venocavography or arteriography to identify tumor renal processes;
- computed venography or MRF.
To determine the composition of the blood, laboratory tests are carried out:
Which doctor should I contact?
The problem of IVC syndrome is dealt with by a phlebologist and a vascular surgery doctor.
treatment
There is no clear treatment plan for the pathology.
In most cases, conservative treatment is carried out in combination with various procedures.
Drug therapy
The main pharmaceutical group used in the treatment of thrombosis. These include anticoagulants, which thin the blood and prevent increased thrombosis.
Treatment is carried out based on the symptoms of the disease and the causes that led to it.
Prescribed medications:
- Warfarin is an anticoagulant for oral administration;
- Fraxiparine - intramuscular injections;
- Refortan - for plasma replacement in case of blood loss;
- Chimes - to thin the blood.
Antibiotic therapy is required in small doses to eliminate a possible microbial infection.
To strengthen the vascular walls and increase their elasticity, vitamin therapy is prescribed: E and C.
You can eat foods containing these vitamins, or take pharmaceuticals: Aevit and Ascorutin.
Dietary recommendations
To increase elasticity, it is necessary to give preference to such products as:
- cereal crops;
- beans;
- vegetable olive oil;
- beef or chicken liver;
- cabbage - broccoli.
In large quantities: grapes, kiwi, berries (currants, raspberries, blackberries). Citrus fruits include oranges and grapefruit.
Prohibited: spicy foods and carbonated drinks, in particular mineral salt water.
Homeopathy
Homeopathy is used quite often.
Treatment is carried out with drugs based on thrombin and fibrinogen.
Among the frequently prescribed drugs, the leading positions are occupied by drugs based on the venom of the viper and the striped rattlesnake.
Surgery and contraindications to it
Indications for thrombectomy:
- floating thrombus, contributing to the development of thromboembolism;
- coarctation;
- blocking the blood supply to the vessels of vital organs;
- long-standing thrombosis from 14 to 20 days;
- ineffectiveness of conservative treatment;
- frequent relapses of the syndrome.
The operation is contraindicated for persons with an acute infectious process, decompensated cardiac pathology and a recent history of stroke.
Surgical intervention is based on balloon dilatation followed by stenting of the vessel.
ethnoscience
Alternative medicine recipes are taken after consultation with a doctor and in the absence of an allergic reaction. Decoctions are prepared from medicinal herbs that help boost immunity and thin the blood.
Herbal infusion No. 1
- Yarrow – 25 g;
- Immortelle – 100 g;
- Lingonberry leaves – 50 g;
- Birch and buckthorn leaves - 50 g each.
Stir and pour 1 tablespoon of the mixture with boiling water (200 ml). Leave in a warm place for 4 hours. During the day, the infusion is drunk.
Infusion of verbena leaves with honey
Verbena leaves -15 g are poured with a glass of boiling water, add a spoonful of honey and leave for about 2 hours.
It is recommended to take 1 tablespoon before meals.
Prevention
Do not self-medicate.
Monitor blood clotting by taking tests for a hemostasiogram.
During the treatment of varicose veins of the extremities and heart pathologies.
Monitor your diet and give up bad habits.
Strong alcohol and tobacco increase hemoglobin, which leads to blood thickening.
: Features of inferior vena cava syndrome
Source: https://venaprof.ru/sindrom-nizhney-poloy-veny/
General information
Inferior vena cava compression syndrome (IVC, aortocaval compression syndrome, postural hypotensive syndrome, hypotensive back syndrome) is one of the most common hemodynamic disorders detected during pregnancy. According to various authors, in the third semester, subclinical manifestations of the disorder of varying severity are detected in 70% of pregnant women, while only about 10% of patients complain of disturbances in well-being. The relevance of timely diagnosis of NSAIDs is associated with an increased risk of gestation interruption and other serious obstetric complications, accompanied by disruption of the normal development of the child and an increase in perinatal mortality.
Diagnostic methods
The examination reveals dilated veins in the neck and chest, persistent swelling in this area, redness or cyanosis of the face and upper chest, hoarseness, and enlarged tongue. These manifestations become stronger when bending over and lying on your back. To clarify the location and cause of compression or blockage of the SVC, instrumental diagnostics are prescribed:
- radiography,
- CT or MRI,
- phlebography,
- Ultrasound of neck vessels,
- measurement of venous pressure.
When examined by an ophthalmologist, dilated and tortuous veins on the retina, congestion and swelling in the optic disc area, and high intraocular pressure may be detected. If there is a suspicion of a lung tumor, then bronchoscopy is prescribed, during which bronchial tissue and sputum are taken for examination. A biopsy of lymph nodes, bone marrow, and mediastinal organs is performed.
Causes
Aortocaval compression during gestation is usually caused by mechanical compression of the venous vessels by the enlarged uterus and a general increase in intra-abdominal pressure. It is extremely rare that blood flow in the inferior vena cava is disrupted due to a combination of pregnancy with other causes - congenital narrowing, thrombophlebitis, volumetric neoplasia of the abdominal organs, retroperitoneal space, liver diseases. By the end of pregnancy, the weight of the uterus increases 10-20 times, the weight of the fetus reaches 2.5 kg or more, the volume of amniotic fluid is 1-1.5 liters. As a result, the elastic vascular wall, when the patient is positioned on her back, experiences a pressure of 6-7 kg, which leads to a decrease in the lumen of the vein.
Although this situation occurs in almost all pregnant women, the typical clinical picture of SNPV is observed only in 9-10% of patients, and in another 17-20% of women the disease is subclinical. In the course of research, specialists in the field of obstetrics and gynecology have found that the following predisposing factors increase the likelihood of developing the disorder during pregnancy:
- Insufficiency of collateral circulation
. Normally, to compensate for impaired blood flow in the IVC system, a network of paravertebral and innominate venous plexuses is formed, providing blood discharge above the site of compression or into the superior vena cava. With insufficient development of collaterals or their accelerated reduction under the influence of unknown causes, hypotensive postural syndrome occurs. - Undifferentiated connective tissue dysplasia
. With a genetically determined disorder of collagen synthesis and its spatial organization, the middle tunic of the veins is less resistant to external compression. The situation is aggravated by gestational hormonal changes. An increase in progesterone concentration by 10 times or more leads to relaxation of the smooth muscle fibers of the outer shell of the vena cava. - Pathological gestation
. The IVC is more compressed during multiple pregnancies, polyhydramnios, gestation of a large fetus arising from a Rhesus conflict, congenital anomalies of the child, extragenital diseases (diabetes mellitus, cardiac pathology), etc. Almost a third of pregnant women with IVC suffer from vegetative-vascular dystonia, 15% from arterial hypertension, 17% have gestosis, 22% are overweight.
Kava syndrome - basic information
To better understand what superior vena cava syndrome is, we need to delve into the anatomy of the chest. The superior vena cava (SVC) is an important blood vessel, which is located in the middle mediastinum, and around it there is the chest wall, trachea, bronchi, aorta, and lymph nodes. The SVV takes blood from the head, neck, arms, and upper half of the torso. There is low pressure in this vessel, and this is quite normal. It is for this reason that any pathology of nearby tissues can damage the thin wall of the venous vessel and seriously disrupt blood flow.
Thanks to the system of anastomoses (the junction of two blood vessels), the body independently copes with impaired patency of the SVC. But when the pressure rises to 250 mm Hg, then a crisis occurs. This is a very dangerous condition, so the patient requires urgent medical attention, otherwise death is inevitable.
SVPV is a secondary disease that complicates many pathologies associated with damage to the organs of the thoracic cavity. The pathology is based on compression or SVC, as a result of which the outflow of blood through the veins from the head, neck, arms and organs of the upper half of the torso is disrupted. Such a violation can lead to dangerous complications. The risk group includes men aged 30 to 60 years.
The superior vena cava is located in the middle mediastinum, next to the aorta, trachea and bronchi
Pathogenesis
With caval compression, the outflow of blood from the lower extremities, abdominal and pelvic organs is complicated. Venous return is reduced, and accordingly, less blood enters the pulmonary alveoli, its oxygenation decreases, and hypoxemia develops. At the same time, cardiac output and the vascular pressure that depends on it decrease. Due to the entry into the systemic circulation of a smaller amount of blood that is not sufficiently saturated with oxygen, tissue hypoxia develops in various organs of the pregnant woman and child. Part of the plasma is deposited in the vascular bed of the lower extremities and loose tissue of the genitals, which contributes to varicose veins.
Features of “pregnant” anatomy
Although such a nuisance often happens to expectant mothers, especially closer to the third trimester, the syndrome has not been discussed in detail in popular literature and special publications, since it does not per se relate to pregnancy pathologies or diseases. These are features of the anatomy of the expectant mother and the location of her vessels and uterus in the abdominal cavity, which creates such sensations. To understand the mechanism, it’s worth getting a little more familiar with the anatomy.
Everyone knows that from the heart to the tissue, blood flows through arteries that branch to capillaries in the tissues, and back it collects into veins, inside which it eventually flows to the heart. The vena cava is the largest vessel in the body through which blood flows to the heart and then goes to the lungs to be enriched with oxygen. There are two parts in its structure - lower and upper, and in relation to our conversation, it is the inferior vena cava that is most interesting.
It collects blood from the lower abdomen, pelvic organs and extremities, and is located along the right side of the spine. In its structure, it is relatively soft and pliable, in contrast to the more elastic and dense artery, where blood flows under pressure. Therefore, it is easier to clamp or squeeze a vein in various situations, including during pregnancy. This is due to changes in blood circulation that occur during pregnancy, growth of the uterus and changes in anatomical relationships in the abdominal cavity.
Symptoms of NSAIDs during pregnancy
In two thirds of patients, the disorder is asymptomatic or with increased motor activity of the fetus when the woman’s body position changes. Signs of postural hypotension usually first appear at 25-27 weeks of gestation. Pathological symptoms appear 2-3 minutes after the pregnant woman lies down on her back, and reaches a maximum within 10 minutes. It is extremely rare for SNVP to occur in a sitting position. More than half of the patients with a clinically significant disorder complain of dizziness, a feeling of shortness of breath, difficulty breathing, sudden weakness, increased heart rate, and more frequent and violent movements. 37% of patients experience a spontaneous desire to roll over or stand up. Sometimes precordial pain, noise or ringing in the ears, sparks before the eyes, loss of visual fields, anxiety, and fear occur. In 1-3% of patients, there is a significant drop in blood pressure (up to 80 mm Hg and below), leading to fainting. Symptoms quickly disappear after changing body position.
Complications of the syndrome in pregnant women
According to doctors, at least once during the entire pregnancy, up to 80% of women experienced discomfort associated with vein compression syndrome, but severe situations with frequent attacks of dizziness and malaise are typical for no more than 10%.
This syndrome also has dangerous complications that arise during prolonged episodes of compression. So, in some cases, this threatens premature abruption of the placenta, which suffers from hypoxia. The main symptom of this will be bleeding, not accompanied by any pain. In this case, emergency medical assistance is needed.
An equally important consequence of the syndrome is an increase in venous pressure in the veins of the legs and in the pelvic area, which threatens the formation of varicose veins or the progression of pathology. The development of hemorrhoids against the background of periodic compression of the veins is also dangerous due to the fact that the pressure in the area of the rectal veins increases sharply.
What is also dangerous for this pathology is that even against the background of changes that are barely noticeable for the mother, the fetus can suffer significantly. According to CTG data, performed at the time of compression of the vein, if the mother is lying on her back, the fetal heartbeat can sharply slow down within a few minutes after compression, which threatens him with hypoxia and serious developmental problems .
Complications
SNPV is often complicated by disruption of placental blood flow with the occurrence of chronic or acute fetal hypoxia and delayed fetal development. In women with compressed inferior vena cava, the placenta is significantly more likely to experience premature abruption of the placenta. Venous stagnation provokes the onset of hemorrhoids, varicose veins, thrombosis, thrombophlebitis. When large volumes of blood are deposited in the vessels of the lower extremities, hypovolemic shock is possible with multiple organ damage - impaired renal glomerular filtration, respiratory distress syndrome, cerebral and cardiovascular failure.
Diagnostics
Inferior vena cava syndrome during pregnancy is usually diagnosed on the basis of a decrease in blood pressure and characteristic symptoms that occur when a woman is lying on her back. If a subclinical course of the disorder is suspected, a comprehensive examination is prescribed to identify changes in hemodynamics and disturbances in the blood supply to the fetus. To confirm the diagnosis it is recommended:
- Echocardiography
. During the echocardiography study, changes in indicators are assessed when the pregnant woman turns from the left side to the back. The presence of a latent postural hypotensive syndrome is indicated by a 15-20% drop in stroke volume, minute blood volume, cardiac index, increased heart rate, and disturbances in other indicators that reflect the pumping function of the heart. - Dopplerography
. The results of ultrasound scanning of the uteroplacental blood flow are also assessed taking into account the patient’s body position. When a woman turns onto her back as a result of caval compression, the resistivity index (RI) in the umbilical artery is 1.15-1.29 times higher than the normative values. At the same time, IR in both uterine arteries decreases by 10-19%. - Integral rheography
. Non-invasive recording of changes in tissue resistance to high-frequency current allows you to quickly assess the blood supply to the vascular bed. Rheographic determination of stroke and minute blood volumes, heart rate, cardiac index confirms the results of an echocardiographic study or, if necessary, replaces it.
Taking into account the increased risk of fetal hypoxia, dynamic monitoring of its condition using CTG and phonocardiography is recommended. According to indications, a spectrophotometric analysis of the blood gas state of a woman and, in exceptional cases, a child is performed. Typically, this method reveals a decrease in the partial pressure of oxygen, an increase in the partial pressure of carbon dioxide, and signs of metabolic acidosis.
Differential diagnosis is carried out with other disorders in which the inferior vena cava is compressed - stenosis, thrombosis, neoplasia of the liver, pancreas, uterus, ovaries, kidneys, bladder, retroperitoneal lymph nodes, retroperitoneal fibrosis, Budd-Chiari syndrome with thrombus growth in the inferior vena cava vein. Pathological conditions that can provoke collapse are excluded: vegetative-vascular dystonia, arterial hypotension due to food or drug poisoning, acute infection, arrhythmia, heart failure. According to indications, the patient is consulted by a cardiologist, phlebologist, gastroenterologist, hepatologist, urologist, and oncologist.
Treatment
In case of secondary superior vena cava syndrome, treatment is symptomatic. It is used together with the main therapy. The purpose of auxiliary treatment is to maintain the body's internal reserves. Conservative therapy includes:
- oxygen inhalations;
- diuretics;
- cortecosteroids.
Diuretics in the treatment of this syndrome
A low-salt diet, bed rest, and thrombolytic therapy are recommended. The head end of the bed should be raised.
Severe cases of superior vena cava syndrome will require surgery. The patient may be prescribed:
- thrombectomy;
- resection of the damaged section of the vena cava (a homoimplant is installed in its place);
- shunting (bypass of blood outflow);
- removal of mediastinal cysts;
- stenting of the greater vena cava.
Long-term catheterization will require balloon dilatation of the damaged area.
Treatment of SNSAIDs during pregnancy
As a rule, postural hypotension caused by caval compression resolves spontaneously when the patient turns on her side or stands up. Pregnant women with clinical signs of the disorder should sleep on their left side with a pillow between their legs or under their upper leg. Some women feel better when resting in a semi-sitting position. To reduce venous stagnation and improve hemodynamic parameters, moderate physical activity is recommended - walking, exercises in water, yoga for pregnant women. If intrauterine hypoxia occurs, drugs are prescribed that improve blood flow in the uteroplacental complex.
The presence of SNPV must be taken into account when planning the method of delivery. In the absence of obstetric and extragenital indications for cesarean section, patients are recommended to have a natural birth in an upright, standing, sitting or squatting position. This can significantly reduce the risk of fetal hypoxia. If a woman insists on the traditional method of childbirth, she is placed on her left side, and during the period of exile she is transferred to a maternity chair with her head raised high. During operative delivery, caval compression more often provokes critical hemodynamic disturbances, which is important to remember when preparing for and during the intervention.
Symptoms
Symptoms of superior vena cava syndrome are caused by impaired venous blood flow in the SVC system. The clinical picture is influenced by the rate of development of cava syndrome, as well as the degree of blood flow disturbance. Depending on these indicators, SVVC can develop slowly (with compression or invasion of the vessel) or quickly (with blockage of the SVC with blood clots).
The patient's upper body swells, the skin of the face and neck turns blue
The clinical picture of SVPV includes swelling of the face, neck, arms, and upper torso due to dilation of superficial venous vessels, as well as bluish discoloration of the skin and mucous membranes. In addition, patients complain of shortness of breath, a feeling of lack of air, hoarseness, difficulty swallowing, coughing attacks and chest pain. An increase in these signs is observed when the patient takes a horizontal position, so they are forced to be in a semi-sitting position. Due to swelling of the larynx, stridor appears (wheezing, noisy breathing, rough and hoarse voice).
Often SVPV is accompanied by nasal, pulmonary, gastric, and intestinal hemorrhages due to increased venous pressure and rupture of thinned vessels. Disturbed venous outflow from the cranium provokes headaches, noises, drowsiness, convulsions, and fainting. The functionality of the oculomotor or auditory nerves is impaired, double vision, protrusion of the eyeballs, excessive secretion of tear fluid, and various hearing disorders develop.
Prognosis and prevention
The outcome of pregnancy and childbirth with timely detection of SNPV is favorable and becomes serious only if the patient does not comply with the recommendations of the obstetrician-gynecologist for lifestyle correction. For preventive purposes, all pregnant women after 25 weeks are advised to avoid sleeping and resting on their back, reduce excess weight, and have sufficient physical activity to maintain normal hemodynamics. Women with polyhydramnios, multiple pregnancy, obesity, varicose veins of the lower extremities, genital organs, if signs of intrauterine hypoxia of the child appear (increased or slowed movements, changes in their intensity), in order to prevent possible complications, need to undergo examination to exclude hidden forms of postural hypotension on the back.