Renal agenesis is a rare condition in which babies are missing one or both kidneys at birth. In the past, many people born with one kidney lived their lives unaware of the abnormality. Today, prenatal ultrasound examination greatly facilitates the diagnosis of pathologies of the paired organ, informing parents in advance about the characteristics of the body of their unborn child. This makes it possible to take timely care of the health of the baby’s only kidney.
- 2 Causes of congenital pathology
- 3 Symptoms and signs
- 4 Diagnostics
- 5 Treatment and prospects
- 6 Consequences and complications
- 7 Features of aplasia during pregnancy
- 8 Video: how to treat renal agenesis
- 9 Reviews
Renal agenesis: definition and features
Normally, the fetus's kidneys develop between the 5th and 12th weeks of pregnancy. By the 13th week they are usually producing urine. If an intrauterine ultrasound after this period reveals a lack of amniotic fluid (oligohydramnios), this may indicate a violation of the baby’s kidney development.
Renal agenesis (aplasia) is a congenital pathological condition that represents the absence of one or both kidneys. Unilateral agenesis occurs in 1 in 1,000 to 2,000 babies and means that the baby develops only one kidney: the left or the right. It is not fatal and often does not cause any consequences, but is associated with abnormal development of the genital organs in 12% of boys and 40% of girls.
Kidney agenesis is a congenital anomaly consisting in the complete absence of one or both kidneys in a newborn.
Often, the absence of a kidney in adulthood is discovered accidentally during X-rays taken for another reason. A single kidney increases in size due to accelerated cell division and takes over the function performed by two kidneys.
The absence of both kidneys at birth—bilateral agenesis—is a pathology incompatible with life. Occurs in 1 in 4,500 live births, usually boys. About 40% of babies with bilateral renal agenesis are stillborn, and the rest will live only a few hours.
VC development options
Completely closed VC, in which there are no missing or underdeveloped (hypoplastic) components, occurs in only 20–25% of people.
There are a huge number of possible variants of the anatomical structure and development of the VC. The most common ones are:
- hypoplasia of one or two PCAs; hypoplasia or absence of the ACA segment; PSA hypoplasia; absence of one of the SSAs.
B - hypolasia of the right posterior communicating artery
C - hypolasia of the left posterior communicating artery
D - bilateral hypoplasia of the posterior communicating arteries
E – the right posterior cerebral artery is absent or not developed
F - the left posterior cerebral artery is absent or not developed
G - hypoplasia of the left communicating artery and the right posterior cerebral artery is absent or not developed
H - hypoplasia of the right communicating artery and the left posterior cerebral artery is absent or not developed
I – hypoplasia of the anterior communicating artery
J - anterior communicating artery and hypolasia of the left posterior communicating artery
K – hypoplasia of the right anterior cerebral artery and hypoplasia of the right posterior communicating artery
Causes of congenital pathology
The exact cause of renal agenesis in newborns is not known. Most cases of the anomaly are not inherited from the parents and are not the result of any behavior on the part of the mother. In approximately 25% of cases there is a genetic component. These are mutations that are passed on from parents who have a similar disorder or are carriers of a mutant gene. The presence of these mutations helps to determine the so-called prenatal testing - fetal DNA analysis.
The risk of having renal aplasia during a repeat pregnancy is about 3–4%. If the condition was accompanied by multiple developmental anomalies, the likelihood of the scenario repeating during a future pregnancy reaches 8%.
Although the exact cause of the pathology is unknown, unilateral renal agenesis is more common with intrauterine growth retardation and often leads to premature birth. The anomaly is more common during pregnancy with twins or triplets.
Symptoms of circulatory disorders in the PCA
Clinical manifestations of impaired blood flow in the PCA depend on the location of the damage. These may be symptoms of damage to the midbrain, thalamus, occipital and parietal cortex.
Also, the clinic varies depending on the type of pathology. So, a stroke is an acute circulatory disorder, so symptoms develop suddenly and rapidly. And dyscirculatory encephalopathy, in turn, is a chronic disease. Consequently, the clinic progresses slowly, and for a long time no symptoms are observed at all.
The most specific disorder of blood flow in the posterior cerebral artery is ischemic stroke. This is a disease in which a vessel is blocked by a thrombus or embolus, which impedes blood circulation. As a result, necrosis (death) of a part of the brain occurs.
The following groups of symptoms are distinguished:
- apical basilar artery syndrome;
- visual disturbances;
- mental disorders;
- motor disorders.
Apex basilar artery syndrome occurs when blood flow is disrupted in the distal part of the vessel, before it divides into the right and left PCA. In this case, all brain structures that receive blood from the PCA are affected. The patient's consciousness is impaired, to the point of coma, his vision and psyche suffer. Motor function is often preserved.
Symptoms and signs
In children with unilateral aplasia with a healthy solitary kidney, symptoms and signs of pathology, as a rule, are absent. But, unfortunately, this does not exclude the possibility of their manifestation in the future, more often after 25–30 years. Less commonly, both types of renal agenesis may be associated with other birth defects, including problems with the lungs, reproductive system (usually the missing kidney), and urinary tract problems.
Associated symptoms may include:
- high blood pressure;
- the presence of protein or blood in the urine (when the kidney is not working well);
- swelling of the face, arms or legs.
Children born with bilateral agenesis have various physical features, such as:
- wide-set eyes with skin folds above the eyelids;
Potter syndrome is a set of signs in an infant acquired as a result of the congenital absence of both kidneys and a small amount of amniotic fluid.
- low-set ears;
- flat and wide nose;
- small chin;
- limb defects.
This group of defects is known as Potter syndrome. Urine makes up most of the amniotic fluid (amniotic fluid) that surrounds and protects the fetus. An organism without kidneys or with an underdeveloped organ does not produce urine, which leads to a decrease in the level of amniotic fluid and incomplete development of the lungs, as well as to fetal compression.
Circle of Willis and variants of its structure
The circle of Willis is an anatomical formation of blood vessels, localized at the base of the brain, which ensures the redistribution of blood between different vascular areas in the presence of insufficient blood supply to the brain. It is a closed polygon representing a vascular anastomosis.
The circle of Willis is formed from the anterior and posterior communicating arteries (ACA and PCA), the initial segments of the anterior and posterior cerebral arteries (ACA and PCA), the supracuneiform segment of the internal carotid artery (ICA) and the distal basilar artery (BA).
In its anterior section, collateral circulation occurs between the carotid artery systems (for example, the ICA and ACA of the right side - PSA - ICA and ACA of the left side), and in the posterior section - between the carotid artery system and the vertebrobasilar system (ICA - PCA - PCA - OA ).
It is worth noting that a normally developed and completely closed circle of Willis is found in only half of the planet's population. Hypoplasia or aplasia of the PCA and ACA, as well as hypoplasia of the PSA and PCA, are widespread. In the anterior section, deviations from the norm are detected slightly less frequently than anomalies in the structure of the posterior section.
The PSA is very variable in its structure, size and location: options range from complete absence to the formation of a wide fistula at the site of contact of the ACA, and doubling or tripling of the PSA is also possible. “Anterior trifurcation” of the anterior cerebral artery is very rare: both ACAs arise from the same ICA. In this case, the circle of Willis is open in the anterior section. A fairly rare anomaly is the presence of an additional ACA called Wilder's artery.
The posterior region is normally found in only about half of the world's population. Anomalies of the posterior section can be very diverse: a wide range of sizes, asymmetry in the origin of arterial branches, absence of segments or even arteries. The most common anomaly is the difference in the diameters of the vertebral arteries: hypoplasia of one with simultaneous hypertrophy of the other. At the present stage, it is believed that one vertebral artery is dominant and the second is recessive based on their overall contribution to the blood flow of the vertebrobasilar region. Permissible asymmetry 50%. The diameter of the SSA is usually slightly smaller than the PSA. PCA hypoplasia is also quite common.
A variant of the development of the circle of Willis is a pronounced anomaly in the structure of the intracranial vertebrobasilar system: the vertebral arteries of both sides do not completely unite into the main artery, anastomoses of irregular structure are possible or the arteries run in isolation. In the case of aplasia of the basilar artery or PCA, an openness of the posterior part of the arterial circle of the brain is formed. It is from the posterior part that the perforating branches go to the midbrain and diencephalon. It turns out that an open circle of Willis can exist in both the anterior and posterior segments. Moreover, it can be opened completely (there are no connecting arteries) or incompletely (with hypoplasia or narrowing).
Changes in the normal structure of the arterial circle of the brain can be both congenital and acquired - the result of the adaptation of certain parts of it to changed hemodynamic conditions in various pathologies of the great vessels of the head, which often develop in these cases. Assessment of individual characteristics in the structure of the vascular bed is carried out according to angiography and is very important in neurological practice. When making a diagnosis, it is necessary to distinguish between changes in the arteries: which are the cause and which develop as a result of pathological changes.
Diagnostics
Both types of agenesis can be diagnosed by ultrasound. Unilateral aplasia is found when one developed kidney is abnormally enlarged for the gestational age of the fetus. For the same reason, hypertension may develop, requiring subsequent postpartum examination.
Bilateral renal agenesis can be observed using ultrasound findings, which indicate complete or severe depletion of amniotic fluid levels after 14–16 weeks. Failure to visualize the fetal bladder after 16 weeks of gestation should prompt clinicians to further investigate bilateral renal agenesis.
What consequences can have improper development of the Circle of Willis?
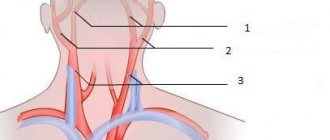
The main task of this system is to ensure sufficient blood supply to certain areas of the brain. This is especially important in case of impaired blood flow in the arteries of the neck. Obstruction of blood flow through the cervical arteries threatens oxygen starvation of the brain, which provokes various abnormalities. To prevent this from happening, the Circle of Willis is provided.
Ensuring the functionality of the circle is achieved due to the fact that the carotid arteries are connected not only to each other, but also to the vertebral arterial system. This scheme allows you to constantly supply the brain with nutrients.
According to statistical data, the classic version of the development of the Circle of Willis is observed only in 50% of cases. For many people, its symmetry is broken.
In the normal state, the circle of Willis is closed. It acts as a backup system. If no deviations in the functioning of the cervical arteries are observed, then it is not used. Therefore, even if there are deviations from normal development in it, they do not manifest themselves in any way.
When there is a problem with the supply of nutrients to the brain, the Circle of Willis is activated. It helps pump blood from other parts. In this case, its pathology can have negative consequences for health.
Unlike other arteries of the brain, there is no pressure difference in parts of the circle. This is due to a lack of pressure balancing from the brain tissue. This can lead to the following negative consequences:
- Frequent dizziness.
- Unpleasant sensations when suddenly changing the position of the head.
- Severe headaches that cannot always be relieved even with painkillers.
- Migraine attacks, which are accompanied by photophobia, nausea, and reaction to sounds.
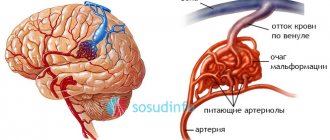
Aneurysm is considered one of the most dangerous pathologies. It appears due to thinning and increased elasticity of the artery wall. Moreover, this process is completely asymptomatic. Any impact on the head area leads to instant rupture of the aneurysm. If measures are not taken in a timely manner, the person will simply die.
The anatomy of the structure normally assumes the formation within the circulatory system of a closed ring - the Circle of Willis. The main arteries that make up the Circle of Willis:
- Forebrain (primary section).
- Front connecting.
- Internal carotid (supracuneiform department).
- Rear connecting.
- Posterior brain (primary section).
Numerous arteries branch off from the Circle of Willis, forming a branched network, the anatomical structure of which allows, if necessary, to nourish any part of the brain. Various deviations in the formation of the structure of the system are more often congenital anomalies, less often they arise as a result of previous infectious diseases, traumatic brain injuries, vascular pathologies (atherosclerosis, impaired neurohumoral regulation).
The main function of the system is the regulation of cerebral hemodynamics. If there is a decrease in the blood supply to a certain area of the brain, the system represented by the VC redirects blood flow in such a way as to replace the blood lost in areas that are deficient.
Thanks to the system, many anomalies in the development of cerebral vessels (aplasia, hypoplasia) are not accompanied by neurological symptoms and often become an incidental finding during a diagnostic examination prescribed for another reason.
Treatment and prospects
The need for treatment of renal agenesis depends on the severity and type (unilateral or bilateral) of the pathology. For both types of agenesis, the standard treatment protocol includes monitoring the baby with multiple ultrasounds and planning the birth in a center where there is a team of intensive care specialists and the necessary equipment to support the life of the newborn if necessary. A caesarean section is usually not required when delivering a baby with renal aplasia.
Most newborns with a single kidney, as long as it is healthy, do not have any lifestyle restrictions compared to their peers with two kidneys. Quality of life depends on the health of the remaining kidney and the presence of other pathologies. To avoid damaging the only kidney, children with renal agenesis may need to avoid contact sports as they get older. In general, physical activity is beneficial for the health of people with unilateral aplasia. Fortunately, the kidneys are located deep in the body and are less likely to be injured compared to the head, spleen or liver.
Once diagnosed, patients of any age with a solitary kidney should have their blood pressure monitored annually and have urine and blood samples tested to check the function of the main organ of the urinary system. Otherwise, children with a single working kidney should be treated no differently than healthy children. They do not need special diets.
Bilateral agenesis is usually fatal within the first few days of a newborn's life. Babies usually die from underdeveloped lungs soon after birth. However, a small percentage of newborns with this pathology survive. But the only treatment available for them is experimental. They are indicated for long-term dialysis, which replaces the function of missing kidneys. Dialysis is the procedure of filtering and purifying blood using a machine.
The first case of survival of a child with bilateral renal agenesis was recorded in the United States in 2013 thanks to new treatment methods. After birth, the child was dependent on dialysis for three years, after which he received a kidney transplant from his father.
Hemodialysis is the purification of the blood from waste accumulated during the metabolic process using an “artificial kidney” device.
Factors such as lung development and overall health determine the success of this treatment. Once diagnosed by prenatal ultrasound, this defect can be corrected in utero through a series of amnioinfusions. Doctors inject saline into the amniotic sac (the sac of amniotic fluid) to help the baby's lungs develop. Once the lungs begin to develop, the baby is able to survive outside the womb. The goal of this treatment is for the child to live through dialysis until he is strong enough to receive a kidney transplant.
Diagnostics: identifying structural variants of the Circle of Willis
In most people, open VC does not manifest itself in any way. The development of the circle of Willis and its variants are most often detected accidentally, during examination of cerebral vessels for other reasons.
If the patient has symptoms of an unruptured cerebral aneurysm, the following examinations are performed:
- CT angiography is a non-invasive (that is, without penetration into the body) X-ray examination, during which a contrast agent is injected into the bloodstream to visualize the blood vessels of the brain, and then a computed tomography is performed. Magnetic resonance imaging is a non-invasive technique that uses a magnetic field and radiofrequency waves to produce detailed images of the blood vessels in the brain. Cerebral angiography is an invasive examination during which a special catheter is inserted into the brain artery. After this, contrast is injected through the catheter and an x-ray is taken.
Consequences and complications
Babies born with one kidney usually live relatively normal lives, provided they receive good medical care and treatment (if necessary). However, as they age—usually after 25–30 years—such patients are at increased risk of:
- proteinuria (abnormal presence of protein in the urine) - develops in approximately 19% of examined patients;
- hypertension (sustained increase in blood pressure) - observed in 47%;
- renal failure (decreased renal function) - observed in 13% of patients.
Treatment of cerebrovascular accidents
Drug therapy for disorders of blood flow in the vessels of the brain depends on several factors:
- severity of the process (acute, subacute or chronic);
- type of circulatory disorder (ischemic or hemorrhagic);
- the presence of concomitant diseases (atherosclerosis, diabetes, arterial hypertension, etc.).
All vascular drugs to improve blood circulation in the brain can be divided into several groups:
- vasodilators, or vasodilators;
- anticoagulants and antiplatelet agents;
- nootropics;
- herbal remedies.
Vasodilators are used for both chronic and acute circulatory disorders. They effectively lower blood pressure and increase the supply of oxygen and nutrients to brain tissue.
The use of vasodilators for stroke should be very careful. The doctor prescribes them only for extremely high blood pressure numbers. A sharp decrease in pressure is contraindicated, as it can further aggravate the patient's condition.
Calcium antagonist drugs are widely used to dilate blood vessels. They cause relaxation of the vessel wall and an increase in the diameter of its lumen. There are two generations of drugs. The first includes “Verapamil”, “Nifedipine”, “Dilacor”. Second generation: “Felodipine”, “Clintiazem”, “Nasoldipin”.
Antiplatelet agents and anticoagulants are prescribed for the treatment and prevention of acute cerebrovascular accidents. They are not able to resolve an existing blood clot, but prevent the formation of new ones. Thrombolytic therapy is becoming increasingly popular in modern neurology. The use of drugs in this group is more effective, as they can dissolve existing blood clots. Due to the high cost, these drugs are still not available in some medical institutions.
The most common antiplatelet agents are:
- "Acetylsalicylic acid";
- "Courantil";
- "Akuprin";
- "Ticlopidine";
- "Aspilate."
The following anticoagulants are most often used in medical practice:
- "Heparin";
- "Warfarin";
- "Clexane";
- "Fragmin."
Nootropics are another group of vascular drugs for improving blood circulation in the brain. These drugs improve metabolism in its cells and increase their resistance to oxygen deficiency. With constant use of tablets, memory improves, fatigue goes away, and cognitive functions increase.
The most effective nootropics are:
- "Piracetam";
- "Phenibut";
- "Pantogam";
- "Phenotropil";
- "Cerebrolysin";
- "Glycine".
To improve blood circulation in the brain, herbal medicines are actively used. Preparations based on Ginkgo Biloba are considered especially effective. They reduce tissue swelling, dilate brain vessels, and increase the elasticity of their walls. Being strong antioxidants, these agents reduce the negative effects of free radicals on brain tissue. The effect of taking Ginkgo Biloba develops slowly and gradually, so the treatment should last at least three months.
What laboratory tests should you undergo to help confirm the diagnosis?
· The primary goal after diagnosis is to identify the entity and prevent ongoing damage to the remaining nephrons.
Bone abnormalities
Complete absence of the tibia occurs most often in the male half of patients. Bone aplasia in this case is characterized by a shortened lower leg or reduced volume in comparison with a healthy limb. The fibula itself is thickened and shortened. The foot may be in a supinated state or even in a dislocated state, with an inward position.
Problems with the patellas or their complete absence rarely occur as a separate anomaly. Most often, the patient still has extramelia, that is, the hips are underdeveloped, and the tibia has tubercles.
Anomalies of the hands most often occur with aplasia of the bones of the forearm - the ulna may be completely absent. Aplasia of the radius occurs in 50% of all bone development anomalies. Most often, the patient is missing 1 finger and wrist bones.
The described ailment can also be expressed in the form of shortened fingers, legs and arms. This disease is called brachydactyly. In this case, dysfunction of the hands is possible if the terminal or main phalanx is missing, and the muscles of the hands are not sufficiently developed.
An anomaly in the development of the hips is noticeable almost immediately, since the patient, as a rule, limps. The prognosis for patients is disappointing - the disease usually progresses with age and causes a person a lot of discomfort and pain.
Stages and forms of uterine aplasia
The stages of the disease are determined in accordance with the severity of the pathology. With uterine aplasia, the following signs of anatomical underdevelopment of the uterus are determined:
- with grade 1, deviations do not go beyond 1-2 cm from the normal size of the uterus;
- at grade 2, the uterus is reduced to 3 cm;
- at grade 3, the uterus is already completely absent, representing a rudiment.
The stage of aplasia is determined by a detailed examination.
The forms of uterine aplasia depend on how other organs are involved in the pathology. Most often, with aplasia of the uterus, aplasia of the vagina also occurs, when this organ has a significant narrowing. With cervical aplasia, the underdevelopment of the uterus is most pronounced in the cervical area, which does not allow pregnancy to occur.
The most favorable course of the disease occurs with aplasia of the cervical canal, since this type of disease allows a woman to conceive and bear a baby.
Causes of development of thyroid aplasia
During pregnancy, a woman’s body undergoes many changes in the functioning of its organs and systems. He needs support in the form of a full supply of vitamins and minerals that will participate in the construction of the tissues of the little man’s future organs. Therefore, every woman should be very attentive to her health during this period, undergo timely diagnosis and tests, since the cause of many pathologies, including aplasia of the left lobe of the thyroid gland, is iodine deficiency and the presence of hypothyroidism. These factors influence the absence of thyroid tissue precisely during the period of fetal development when it is forming.
What tests for thyroid hormones should women take during pregnancy? How does the thyroid gland affect conception?
As a result, only one lobe of the endocrine gland can form. In rare cases, agenesis is diagnosed, which means the absence of the isthmus or right lobe of the thyroid gland.
Genetic disorders or predispositions also play a major role among the causes of pathology. If a relative in the family had an underdeveloped thyroid gland, then there is a chance that the child will also get it.
Some medications that a pregnant woman takes have side effects. One of them is the phenomenon of complete absence of the thyroid gland.
The toxic effects of various pathogenic microorganisms can cause disturbances in the development of this gland. Therefore, during the period of exacerbation of epidemics, all pregnant women are advised to beware of large crowds of people in transport, on the street, so as not to become infected with viruses.
A visit to an endocrinologist during pregnancy is an indispensable condition: only a doctor will be able to identify the pathology in time and protect the expectant mother and child from negative consequences.