Takayasu's disease (Takayasu syndrome, aortic arch syndrome, nonspecific aortoarteritis) is a granulomatous inflammation of the aorta and its large branches and their stenosis. The disease was first described by Japanese ophthalmologist Mikito Takayasu in 1908. The disease mainly affects women. The average age of cases in Europe reaches 41 years, in Japan - 29, in India - 24. It is most common in Japan, Southeast Asia, India and Mexico. There are no exact data on the prevalence in Russia. In children, the disease has a more acute and aggressive course.
Story
In the first descriptions, nonspecific aortoarteritis was called “pulseless disease” - because due to obliteration of the large branches of the aorta, patients often had no pulse in the upper extremities.
Before the official discovery, the most similar disease was described by the professor of anatomy at the University of Padua Giovanni Batista Morgagni (1682–1771) in 1761: in a woman aged about forty years, an autopsy revealed dilation of the proximal part of the aorta in combination with stenosis of the distal parts, the inner layer of the aorta was yellow in color and contained calcifications. During life, the patient had no pulse in the radial arteries.
In 1839, British military doctor James Davy described another similar case. A 55-year-old soldier at the age of 49 developed pain in his left shoulder, and four years later the pulse in his hand weakened, for which he consulted a doctor. A year later, the man suddenly died; an autopsy revealed a large rupture of the aortic arch aneurysm and complete occlusion of the vessels extending from the aortic arch.
In 1854 in London, surgeon William Savory (1826–1895) also reported a disease very similar to Takayasu's disease. In a 22-year-old woman, no pulse was detected in the vessels of the neck, head and upper extremities for five years; seizures began to occur during the course of the disease, and the patient died. An autopsy revealed thickening and narrowing of the aorta and arch vessels - they felt like a thick rope to the touch, there were no aneurysms.
Finally, in 1908, the Japanese ophthalmologist Makito Takayasu, at the Twelfth Annual Conference of the Japanese Society of Ophthalmology, reported on two annular anastomoses around the optic disc in a young woman without pulses in the peripheral arteries. These were arteriolovenular shunts. In addition, the blood vessels surrounding the optic disc were slightly elevated. Japanese colleagues associated changes in retinal vessels with the absence of pulses in the patient’s radial arteries.
Pulselessness syndrome has been called by many names, leading to confusion. It was only in 1954 that Japanese doctors William Caccamise and Kunio Okuda introduced the term “Takayasu disease” (TD) into the English literature.
Methods for diagnosing Takayasu arteritis
A general blood test may show nonspecific signs of inflammation - a moderate increase in the number of leukocytes (up to 15x109), erythrocyte sedimentation rate. In a biochemical blood test, you can see the appearance (or increase) of the amount of C-reactive protein, the appearance of seromucoid, haptoglobin. The levels of albumin and blood globulins and cholesterol decrease.
Diagnosis of nonspecific aortoarteritis is inextricably linked with the use of radiation research methods. The most significant of them include:
- Angiography is simple (using conventional x-ray).
- Computed tomography with the introduction of a contrast agent.
- Multispiral computed angiography (using an MRI machine).
Angiography is extremely important not only for making a diagnosis, but also for assessing the dynamics of the spread of the pathological process. This study allows the doctor to make a prognosis for the patient’s life and evaluate the effectiveness of the therapy used.
Ultrasound, namely Dopplerography, can also be used. It allows you to evaluate the speed of blood flow and the narrowing of the lumen of the arteries. This study also allows you to evaluate the vessel wall.
It is not always possible to conduct a complete diagnosis. However, it is not always required. There are certain criteria that allow a diagnosis of Takayasu arteritis to be made:
- The appearance of signs of the disease before the age of 40 years.
- Changes in the muscles of the lower extremities - the occurrence of pain or weakness even when walking normally, a symptom of intermittent claudication.
The appearance of noise during auscultation in the projection of the abdominal aorta or on the subclavian arteries.- Absence of pulse in the radial artery of the hand (or in both hands).
- Blood pressure when measured on the brachial arteries is different - more than 10 mm Hg.
- Angiography visualizes a narrowing of the lumen of the aorta and its large branches, a narrowing of the branches of the aorta that supply blood to the lower or upper extremities (the changes are not associated with atherosclerosis or fibromuscular dysplasia).
To be diagnosed with Takayasu disease, at least three symptoms must be present.
Etiology and pathogenesis of Takayasu syndrome
Most often, the cause of BT cannot be determined; a connection with tuberculosis and streptococcal infections is assumed. There is evidence of an increased frequency of a number of histocompatibility antigens in patients in various populations:
- India - HLA B5, B21;
- USA - HLADR4, MB3;
- Japan - HLADR2, MB1, Bw52, DW2, DQW1 HLA Bw52‑CAD, AR, HLA B39.
Autoimmune mechanisms play a certain role in the pathogenesis: there is an increase in the level of IgG and IgA and fixation of immunoglobulins in the wall of the affected vessels. Also characteristic are changes in the cellular component of immunity and disturbances in the rheological properties of blood with the development of chronic disseminated intravascular coagulation syndrome.
The course of Takayasu disease (TD) has a certain stage. At an early stage of the disease or during exacerbations, nonspecific symptoms of systemic inflammation occur. During this period, up to 10% of patients do not have any complaints at all. As it progresses, there is inflammation of the vessel walls and the development of stenosis, which almost always occurs, even in patients with aneurysms. Bilateral vascular stenosis predominates.
Principles of treatment
To eliminate the exacerbation of the disease, the patient will have to be hospitalized in a rheumatology hospital.
If the patient has just been diagnosed and needs to select adequate treatment, he is hospitalized in the rheumatology department of the hospital. Also, persons with exacerbation of Takayasu's disease or in case of the development of its complications require inpatient treatment. In the period between exacerbations, when the patient's condition is stable, he receives therapy on an outpatient basis.
So, a person suffering from this pathology may be prescribed drugs from the following groups:
- glucocorticosteroids (prednisolone or methylprednisolone in tablet form, in very severe cases - pulse therapy with methylprednisolone and cyclophosphamide (administration of large doses of these drugs by intravenous infusion));
- cytostatics (methotrexate, cyclophosphamide);
- nonsteroidal anti-inflammatory drugs (diclofenac, ibuprofen, meloxicam, etc.);
- aminoquinolone drugs (plaquenil or delagil);
- with rapid progression of ischemia - direct anticoagulants (heparin subcutaneously or intravenously);
- antiplatelet agents (in parallel with anticoagulants; chimes);
- drugs that improve metabolism in the vascular wall - angioprotectors (Prodectin);
- vasodilators or drugs that dilate blood vessels, improve microcirculation (complamin, prodectin and others);
- for arterial hypertension - ACE inhibitors and antihypertensive drugs of other groups;
- with a pronounced increase in the concentration of renin in the blood - antagonists of this hormone;
- with a long history of illness and a high risk of developing cardiovascular complications - statins (atorvastatin, simvastatin and others).
Depending on the clinical situation and what other organs are affected, the patient may be prescribed other drugs to correct existing disorders.
In severe cases, when there is a pronounced narrowing of the lumen of the vessels, which is not eliminated by drug treatment, the patient is indicated for the intervention of an angiosurgeon in order to restore the patency of the arteries.
Against the background of a correctly selected treatment regimen, in most cases, regression of the clinical manifestations of the disease is soon observed, general and biochemical blood tests return to normal, and positive dynamics are determined in instrumental studies. However, even with complete normalization of the patient’s condition and well-being, treatment is not completely canceled. A person needs to take low doses of prednisolone for the next two years, and then depending on the situation.
Glucocorticoids and cytostatics are very serious medications, so the patient should strictly adhere to the dosage prescribed by the rheumatologist and undergo regular examinations to promptly identify possible complications of such treatment. Unauthorized refusal to take medications is unacceptable and extremely dangerous, since it will certainly lead to a worsening of the patient’s condition and an acceleration of the rate of progression of nonspecific aortoarteritis.
Clinical picture: symptoms of Takayasu's disease
In the acute stage, patients are most often bothered by nonspecific symptoms of systemic inflammation. These are fever, night sweats, malaise, weight loss, joint and muscle pain, and moderate anemia. But already at this stage there may be signs of vascular insufficiency, especially in the upper extremities - absence of pulse. The absence of a pulse or a decrease in its filling and tension in one of the arms, asymmetry of systolic blood pressure in the brachial arteries is recorded in 15–20% of cases. Much more often, in 40% of cases, patients complain of a feeling of weakness, fatigue and pain in the muscles of the forearm and shoulder, often unilateral, aggravated by physical activity. At this stage, BT is diagnosed extremely rarely.
The chronic stage, or the full picture stage, begins after 6–8 years. Symptoms of damage to the arteries extending from the aortic arch predominate due to the progression of inflammation of the vessel walls and the development of stenosis, usually bilateral. Even in the presence of an aneurysm, in almost all cases there is also stenosis. As stenosis progresses, symptoms of ischemia of individual organs appear. Vascular inflammation can occur without systemic inflammatory reactions, then pain is observed at the site of projection of the affected vessel or tenderness upon palpation.
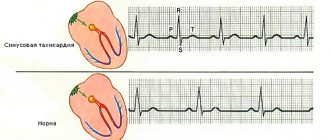
On the affected side, increased fatigue of the arm develops during exercise, its coldness, a feeling of numbness and paresthesia, the gradual development of atrophy of the muscles of the shoulder girdle and neck, weakening or disappearance of the arterial pulse, a decrease in blood pressure, in 70% - a systolic murmur is heard in the common carotid arteries. 7–15% of patients experience neck pain, dizziness, transient moments of visual impairment, shortness of breath and palpitations, and 15% of patients experience pain on palpation of the common carotid arteries (carotidynia).
During this period, compared with the early stage of the disease, symptoms of vascular insufficiency of the upper extremities and intermittent claudication, damage to the cardiovascular system, brain and lungs are much more common (50–70%).
Damage to internal organs
In the chronic stage, symptoms sometimes appear due to damage to the arteries arising from the abdominal aorta, most often with anatomical types II and III of the disease. Vasorenal arterial hypertension of a malignant course, attacks of “abdominal toad” caused by damage to the mesenteric arteries, intestinal dyspepsia and malabsorption may develop.
Clinical signs of lung damage (chest pain, shortness of breath, nonproductive cough, rarely hemoptysis) are observed in less than a quarter of patients.
Damage to the coronary arteries occurs in ¾ of patients, in 90% of cases the mouths of the coronary vessels are affected, and the distal parts are rarely affected. Damage to the ascending aorta is often described - compaction combined with dilatation and the formation of aneurysms. Arterial hypertension occurs in 35–50% of cases and can be caused by involvement of the renal arteries or the development of glomerulonephritis, less often by the formation of coarctation of the aorta or ischemia of the vasomotor center against the background of carotid vasculitis. As a result of arterial hypertension, coronaryitis and aortic regurgitation, chronic heart failure develops.
Complications
Aortic arch syndrome can vary in severity. In some people, the disease is mild and is not accompanied by complications. However, in other cases, prolonged or repeated cycles of arterial inflammation and healing can lead to one or more of the following:
Reduced elasticity and narrowing of blood vessels, which can lead to a decrease in blood supply to organs and tissues. Arterial hypertension, which usually develops as a result of decreased blood supply to the kidneys. An inflammatory process in the heart that can affect the heart muscle (myocardium), the heart valves (valvulitis) or the sac around the heart (pericarditis). Heart failure due to hypertension, myocarditis, or aortic regurgitation—a condition characterized by blood leaking back into the heart due to a leaky aortic valve—or a combination of these conditions. Ischemic stroke is a type of stroke that occurs when blood flow in the arteries leading to the brain is reduced or blocked. Transient ischemic attack, a temporary disorder of cerebral circulation, the symptoms of which are identical to those of an ischemic stroke, but does not cause long-term damage. An aortic aneurysm, which occurs when the walls of a blood vessel weaken and bulge, forming a bulge in the vessel that can rupture. A heart attack (myocardial infarction) is an uncharacteristic phenomenon that can develop as a result of a decrease in blood supply to the heart. Damage to the lungs when the disease develops in the arteries leading to the lungs (pulmonary arteries) Pregnancy
In women with aortic arch syndrome, uncomplicated pregnancy is possible. However, the disease can negatively affect a woman's reproductive ability and the course of pregnancy. If you have aortic arch syndrome and are planning a pregnancy, it is important to work out a detailed action plan with your doctor before becoming pregnant to prevent possible complications. In addition, during pregnancy it is necessary to be under close medical supervision.
Anatomical variants of Takayasu's disease:
Type I - the lesion is limited to the aortic arch and its branches (8% of patients); Type II - the descending part (thoracic and abdominal sections) of the aorta is affected (11%); Type III (mixed) - the most common, includes damage to the aortic arch and its descending section (65%); Type IV - includes lesions characteristic of the first three options in combination with arteritis of the branches of the pulmonary artery; occlusion of the brachial and iliac arteries, damage to the aortic arch and renal arteries is also observed (Takayasu-Denerey syndrome, 16%).
Causes and mechanism of development of the disease
The autoimmune process plays a major role in the mechanism of development of this disease.
Today, researchers are still continuing to study the etiology of Takayasu’s disease; they cannot yet say with certainty the reasons for its development.
- There may be a connection between aortoarteritis and infections previously suffered by the person. In particular, we are talking about bacteria such as streptococci and Mycobacterium tuberculosis. However, in many cases of this pathology, no infectious factor can be detected.
- Genetic predisposition to the disease probably plays a role. Scientists came to this conclusion after discovering it in monozygotic twins. Also in favor of this theory are the facts of the predominant incidence of young women and the identification of certain histocompatibility antigens in people suffering from Takayasu's disease.
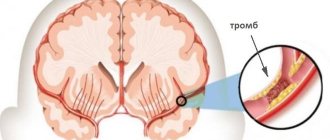
The leading role in the pathogenesis of this disease belongs to the autoimmune process, which most likely originates in small vessels supplying blood to large vessels (the aorta and its branches). The level of immunoglobulins G and A in the blood increases, and the concentration of complement also increases. The lining of the inflamed vascular wall gradually loses its muscle layer, thickens and is replaced by connective tissue, which leads to a narrowing of the lumen of the vessel. If the inflammation progresses faster than this tissue is formed, the wall of the vessel in certain places becomes thinner and bulges out in a bag-like manner - an aneurysm is formed.
Pathomorphology
In the chronic phase, the aorta is thickened due to fibrosis of all three layers of the vessel. The lumen often narrows in several places. If the disease progresses quickly, fibrosis does not have time to lead to the formation of an aneurysm. The intima may be ribbed, with a “tree-bark” appearance; this feature is characteristic of many aortoarteritis. These changes usually occur in the aortic arch and its branches, but the thoracic and abdominal parts of the aorta and their corresponding branches may be involved in the process.
Recent studies of the cellular composition of the aortic walls have shown that the formation of new vessels occurs in the deep intima associated with the adventitia. T cells and dendritic cells are also observed in the vascular environment, with small numbers of B cells, granulocytes and macrophages. Inflammation is most noticeable in the adventitia, with infiltration of B and T cells.
As a result, ischemia, hypertension, and atherosclerosis develop. With a slow course, there is a pronounced development of collateral circulation.
Variants of the course of Takayasu's disease - classification of nonspecific aortoarteritis
Based on anatomical characteristics, this disease is divided into several types:
- Type I - degenerative phenomena are recorded in the aortic arch, as well as the arteries that extend from it.
- Type II - pathological changes are recorded in the thoracic or abdominal arteries.
- Type III – combines the types listed above.
- Type IV – the pulmonary artery and its branches are included in the pathogenic process.
Depending on the nature of vascular damage, nonspecific aortoarteritis is of 3 types:
- Stenotic. Characterized by a narrowing of the diameter of blood vessels.
- Deforming. The structure of blood vessels changes significantly. A similar phenomenon is observed in advanced stages of Takayasu's disease.
- Aneurysmal. Aneurysms form.
In its development, nonspecific aortoarteritis goes through two stages:
Spicy
The symptoms of the disease are very similar to those found in other infectious pathologies.
In particular, this applies to the following complaints:
- Unstable body temperature.
- Frequent fatigue.
- Unexplained weight loss.
- Increased sweating, especially at night.
- Pain in the hip, elbow, knee joints.
These phenomena are present in a number of other infectious diseases, which causes inaccuracy in diagnosis.
One of the early manifestations of nonspecific aortoarteritis is an increase in body temperature
Chronic
It makes itself felt 7-8 years after the onset of manifestation of the disease in question.
The symptomatic picture in the most general terms is manifested by the following pathological conditions:
- Weakness in the muscles, which is chronic in nature.
- Difficulties with coordination of movements.
- Regular pain in the area of large joints.
- Memory impairment.
- Headache.
Such negative phenomena, as a rule, contribute to the detection of nonspecific aortoarteritis.
Treatment of nonspecific aortoarteritis
Taking steroid medications is the main treatment for Takayasu's disease. Data on its effectiveness vary, which may be related to the stage of the disease. Data obtained in the USA in 1985 showed that in six out of 29 patients, steroid treatment led to a decrease in ESR, inflammatory symptoms. Eight of the 16 patients with absent pulses experienced their return after a delay of several months. Later (1994) American studies showed that remission was achieved in 60% of cases (out of 48 patients).
It is now generally accepted that approximately half of patients treated with steroids experience improvement. The lack of universal treatment and the side effects associated with steroid use have led to the search for more effective treatments.
As with other systemic vasculitides, immunosuppressive drugs can be used, including cyclophosphamide, azathioprine, and methotrexate. American researchers in 1994, using the example of 25 patients who were not amenable to treatment with steroid drugs, showed that taking cytostatic drugs (cyclophosphamide, azathioprine or methotrexate) leads to remission in 33% (Takayasu arteritis. Ann Intern Med 1994;120:919– 29).
Since methotrexate is easily tolerated, its effectiveness in combination with steroids was further studied. Thirteen of 16 study participants with aortic arch syndrome taking methotrexate (81%) experienced remission. However, 7 of them experienced relapses when they completely stopped taking steroid drugs. Ultimately, eight patients experienced sustained remission for four to 34 months, and four of them were able to stop treatment completely. In three of the 16, the disease progressed despite treatment.
Thus, about a quarter of patients with active disease do not respond to current treatments.
Treatment of the disease
If a patient has been diagnosed with Takayasu syndrome, then proper treatment is essential. Otherwise, the person’s blood circulation level will begin to decrease, and exacerbations will periodically occur. Treatment involves relieving inflammation in the affected areas. The patient is prescribed the following medications:
- "Prednisolone"
- "Methotrexate"
- "Cyclophosphamide"
- "Azathioprine"
- antihypertensive drugs.
If a person does not have thrombosis, then to prevent this phenomenon, Acetylsalicylic acid, indirect anticoagulants and Dipyridamole are prescribed.
Extracorporeal hemocorrection plays an important role in the treatment of the syndrome. She:
- improves blood flow;
- improvement of vascular function;
- cleanses the blood of blood clots and immune complexes.
Treatment for Takayasu syndrome may include surgery. But indications for surgery are serious concomitant diseases.
If you follow the doctor's recommendations, the patient will quickly feel improvement. After a couple of weeks of therapy, the patient can already be diagnosed with positive dynamics. But, despite the fairly rapid improvement in the patient’s condition, treatment for Takayasu syndrome is long-term and should take at least a year.
Surgery
It is advisable to perform surgical intervention on the aorta and great vessels in the first five years after diagnosis.
- Endarterectomy is indicated for small occlusions.
- Bypass surgery with special prostheses is performed when the lesion is large.
Indications for surgery are determined by the extent of the process and the degree of obstruction of peripheral vessels. Surgery is performed outside the active stage of BT.
Clinical example
A 13-year-old girl was admitted to the pediatric department on the referral of a cardiologist with complaints of headaches, nosebleeds, and increased blood pressure to 220/110 mm.
rt. Art. She did not suffer from childhood infections. Vaccinated according to age up to three years. From the age of nine she was in a boarding school (her mother and father abused alcohol and were deprived of parental rights). At the age of ten, myopia was detected (wears glasses). For the last two years, the child has been under the care of her aunt, who considers the girl sick since she was nine years old, when the above-described complaints appeared. Upon admission to the department, the girl’s condition was of moderate severity, the child had an asthenic build and poor nutrition. During auscultation of the heart, a systolic murmur is heard at the V point. The liver is 1 cm below the edge of the costal arch, blood pressure is at the level of 180–150/85–80.
The hemogram shows slight neutrophilia, ESR - 43 mm/h. In a biochemical blood test, C-reactive protein was elevated, the rest was without pathology, antistreptolysin-O and rheumatoid factor were not detected. Coagulogram - decreased prothrombin index. ECG without pathology. EchoCG revealed moderate hypertrophy of the interventricular septum and posterior wall of the left ventricle, left-sided aortic arch, narrowing of the aorta in a typical location to 5–6 mm. According to CT/MRI, there are signs of Takayasu's disease (type IV): intimal detachment of the ascending aorta with transition to the arch, segmental stenosis of the thoracic descending aorta, damage to long segments of the great vessels of the brain, CT data in favor of segmental narrowing of the left renal artery.
Metipred and methotrexan were prescribed. Symptomatic therapy included aspirin, atenolol, chimes, and captopril. During therapy, regression of general inflammatory signs was noted, but hypertension could not be completely suppressed. Three months later, the dose of metipred was increased, antihypertensive therapy was adjusted, but the pressure remained high. Taking into account the nature of vascular damage (type IV), the unstable and partial anti-inflammatory effect of the therapy, in this case the prognosis for life is very unfavorable.
Adapted from: Okhotnikova E.N. et al.: Takayasu’s disease (nonspecific aortoarteritis) is a fatal systemic vasculitis in children. "Clinical immunology. Allergology. Infectology", No. 2, 2011.
Diagnostic methods
Diagnosis of Takayasu's disease is difficult due to the primary chronic course of the pathology in more than half of people and the nonspecificity of a number of symptoms. During the history and examination, the therapist will pay special attention to clinical manifestations.
A diagnosis such as nonspecific aortoarteritis is obvious if the following criteria are present:
- age up to forty years;
- absent or weakened pulse in the peripheral arteries;
- the patient has intermittent claudication;
- difference in pressure levels on symmetrical limbs;
- the appearance of noise due to auscultation over inflamed vessels.
When establishing a primary diagnosis, the attending physician will definitely prescribe laboratory tests for the patient (biochemical blood test, general urine and blood tests, and in some situations, a biopsy of inflamed vessels).
If the disease is present, blood sampling will reflect a decrease in hemoglobin levels, a slight increase in the white blood cell count, and a moderate increase in ESR. In addition, immunological tests will show an increase in the content of immunoglobulins and the presence of HLA antigens. It should be noted that an autoimmune disease cannot be diagnosed by urine and blood tests alone.
To confirm the diagnosis, instrumental diagnostics should be performed, including:
- phonocardiography;
- echocardiography;
- encephalography;
- ultrasonography.
But one of the most important instrumental research methods is magnetic resonance angiography. Its high sensitivity makes it possible to easily determine stenosis of vascular areas and detect subtle pathological and morphological changes in the arterial wall. This research method is extremely important both for making a precise diagnosis and for assessing the spread of the inflammation process. Magnetic resonance angiography makes it possible to make a prognosis for the patient’s life and evaluate how effective the treatment used is.
How to cure Takayasu's disease?
Exodus
The 5- to 10-year survival rate for Takayasu disease is about 80%, and the five-month to one-year survival rate is close to 100%. The most common cause of death is stroke (50%) and myocardial infarction (about 25%), less often - rupture of an aortic aneurysm (5%). With damage to the coronary arteries in the first two years from the onset of symptoms of cardiac pathology, mortality reaches 56%. An unfavorable prognosis in patients whose disease is complicated by retinopathy, arterial hypertension, aortic insufficiency and aortic aneurysm. Patients with two or more of these syndromes have a 10-year survival rate from diagnosis of 59%, with most deaths occurring in the first five years of the disease.
Contraindications to surgery for aortoarteritis are the acute period of myocardial infarction, stroke, chronic renal failure, sepsis, diabetes mellitus and obliteration of distal vessels.
Classification
The classification of Takayasu's disease depends on the characteristics of the disease, and it is usually divided into four types:
- The first type of disease affects the aortic arch and those arteries that arise from it.
- The second applies to the abdominal and thoracic regions.
- The third combines the previous two.
- The fourth involves the pulmonary artery.
Anatomical classification of Takayasu's disease