Medical editor: Strokina O.A. - therapist, functional diagnostics doctor. September, 2020.
Synonyms: effusion in the pericardial cavity, pericardial effusion
ICD-10 code: I30, I31.3.
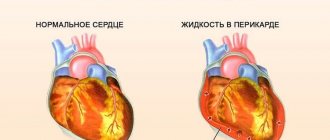
Effusion is an accumulation of fluid in the pericardial cavity. It can be acute or chronic. Acute cases occur with increasing chest pain and dry cough. The chronic form is often asymptomatic. There is no special treatment; therapy is aimed at eliminating the underlying disease.
The liquid accumulates in the form of:
- transudate - non-inflammatory effusion in chronic heart failure,
- with pulmonary hypertension,
In rare cases, air or other gas is found in the pericardial cavity, which occurs as a result of the activity of certain types of bacteria or due to an open chest injury.
The nature of the fluid (transudate or exudate) in the pericardial cavity is determined using laboratory tests by calculating its density, the amount of proteins and other elements. Based on the difference in these elements, the laboratory doctor makes a conclusion about the inflammatory or non-inflammatory nature of the effusion.
Fluid in the pericardium of the heart: what is it, permissibility and norm
Effusion (exudate) is an inflammatory fluid that accumulates in the pericardial cavity by sweating through its leaves.
The accumulation of effusion occurs as a result of an inflammatory response. Inflammation causes the release of biologically active substances and the attraction of blood cells to the site, which is accompanied by the release of fluid through the capillaries.
Can the effusion be physiological and how much free fluid in the pericardial cavity is normal?
The normal amount of fluid in the pericardium is up to 50 ml; it ensures gentle movement of the pericardial sheets, has a low density (1012-1018) and contains single cells. In contrast, exudate has a high protein content (more than 30 g), a density of more than 1018 and a significant content of leukocytes, platelets and fibrin.
Dependence of the patient’s condition on the amount of effusion:
- If there are only traces of fluid in the pericardium, the condition is satisfactory, there is often no temperature, complaints of paroxysmal pain;
- A small, insignificant amount of effusion (up to 150 ml) - moderate condition, fever, constant pain, weakness;
- Moderate (up to 500 ml) – severe condition, weakness, decreased blood pressure and physical activity;
- High (up to 2000 ml) – extremely serious condition, drop in pressure, rapid pulse, loss of consciousness, immobility;
- More than 2000 ml – critical condition, cardiac tamponade.
Rehabilitation
With proper treatment of effusion pericarditis and the absence of complications, recovery occurs after three months. Gradually the person will be able to return to normal life. Longer rehabilitation is necessary in the case of a recurrent form of the disease, when from time to time the effusion in the pericardial cavity accumulates again.
Recovery after surgery requires a longer period: the patient is kept in the hospital for 5 days. If a person’s life is not in danger, he is discharged under the supervision of a cardiologist at his place of residence. Usually, health improves after 3–4 months, and complete restoration of the functioning of blood vessels and the heart occurs after six months.
To speed up the rehabilitation process it is recommended:
- visit your doctor regularly and follow all his instructions;
- monitor your diet: it should be complete and healthy;
- gradually increase physical activity, but do not overload;
- completely eliminate smoking and drinking alcohol;
- monitor your health and immediately seek help if problems arise;
- carry out sanitation of foci of inflammation.
Clinical classification and codes according to ICD-10
- Spicy . ICD-10 code: I30. Characterized by a duration of up to 6 weeks. In the first days, symptoms are limited to increased breathing, tachycardia, fever, pain and decreased blood pressure. Subsequently, compression of the mediastinal organs occurs: the trachea (barking cough), the esophagus (pain when swallowing), and the nerves (hoarseness).
- Subacute . ICD-10 code: I31. It is characterized by a duration of 1.5-6 months and an undulating course. The clinical picture resembles the acute form. The fever is often low-grade (up to 38 degrees). Complaints of palpitations, interruptions in heart function, decreased blood pressure, insomnia. The condition worsens when lying down. Due to coughing and pain when swallowing, patients often refuse to eat.
- Chronic exudative pericarditis . ICD-10 code: I31.9. It is characterized by a duration of more than 6 months and alternating remissions and exacerbations. Symptoms erased due to a decrease in the amount of effusion, manifested by paroxysmal shortness of breath, cough, and change in voice. Patients complain of chest pain, a feeling of fullness in the epigastrium, deterioration of well-being when lying down, and insomnia.
Disruption of metabolic processes in the heart leads to the accumulation of fluid in a volume of up to 1-2 liters (the norm is 20-30 ml) , which significantly compresses the nerve endings and adjacent organs.
Effusive pericarditis is more dangerous than dry pericarditis (which heals spontaneously in some cases), but is more favorable than constrictive pericarditis, which forms dense adhesions with tissue mineralization and prevents healthy contraction of the heart.
Unlike hemorrhagic and serous-hemorrhagic types, it does not lead to an increase in the number of red blood cells.
Sad data: among the total number of autopsies, about 5-6% indicate the presence of problems with the pericardium . The detection of these pathologies is lower, which indicates a low proportion of citizens calling in the presence of the first signs of the disease.
The course of particular types of pericarditis
There are two main forms of the course of developing inflammation of the cardiac membrane - acute and chronic. Fibrinous, infectious, exudative pericarditis with an acute course is often diagnosed.
There are chronic exudative, adhesive and constrictive types of the disease. Among infectious inflammations of the membrane, tuberculous pericarditis is the most common.
Acute fibrinous pericarditis
Fibrinous pericarditis is the most diagnosed type of inflammatory lesion of the pericardial sac. It is difficult to detect, but easy to treat. Young people get sick more often. In this case, fibrinogen from the pericardial fluid of the heart is deposited on the layers of the membrane, causing inflammation. It can be completely cured or go into an exudative form.
Fibrin threads connect the pericardial layers, fluid (exudate) is absorbed, which leads to friction. The main symptoms of the pathology are chest pain in the heart, friction noise, and a slight increase in temperature. In the case of fibrinous disease, no significant circulatory disturbance is observed.
Acute infectious pericarditis
Infectious inflammation of the pericardium most often develops acutely and quickly. In half of all diagnosed cases, the viral origin of the disease is detected. It can manifest itself in a dry and exudative form.
In the first case, pressing pains arising in the heart are characteristic, which radiate and intensify with movement. With an increasing volume of exudative fluid, shortness of breath is expressed, which intensifies. A possible consequence of this disease is tamponade.
Exudative pericarditis
The decisive factor in the development of this disease is not the amount of fluid in the lining of the heart, but the rate of its accumulation. The gradual release of exudate does not cause a sharp deterioration in the patient's condition. Rapid filling of the pericardial sac provokes severe inflammation.
The pain in the heart area intensifies during swallowing. Severe shortness of breath torments, heart rhythms are disturbed, muffled tones are heard. There is pallor of the skin with a bluish tint and swelling.
The main symptoms of pericarditis are pronounced and increase with increasing amount of exudate. Compression of the heart intensifies, tamponade develops, which in some cases leads to cardiac arrest. With poor quality or incomplete treatment, the disease can develop into chronic exudative pericarditis.
Exudative purulent pericarditis
The disease is caused by pyogenic bacteria that penetrate the membrane with blood. Develops in severe form. Purulent contents accumulate in the pericardial sac. Signs of compression of the heart appear. Heart pain is accompanied by rapid heartbeat, shortness of breath, and bluish skin.
Intoxication develops, which is manifested by an increase in temperature and a deterioration in the general condition of the patient. The acute course of the disease in some cases leads to tamponade and cardiac arrest. This disease has a high mortality rate. Medical care is provided only in the form of surgery; medications are not effective.
We recommend further reading: Symptoms of pulmonary edema, as well as causes, treatment and consequences
Hemorrhagic pericarditis
This type of disease occurs due to tumor damage to the heart. It is characterized by the release of an increased amount of fluid in the pericardial sac. Exudate makes it difficult to fill the heart cavity. It has some blood in it.
Heart pain, shortness of breath and swelling occur, as with pericardial effusion. Skin color is gray, feeling of heaviness in the heart area. Laboratory tests reveal blood loss.
Tuberculous pericarditis
The course of the disease is often slow in progression. Pain in the heart is expressed in the initial stages. The accumulation of purulent fluid increases symptoms, and patients often complain of shortness of breath. The disease is difficult to detect.
The outcome of treatment is determined by the condition of the lungs. The prevalence of the disease among HIV-infected and AIDS patients is noted.
Causes
The accumulation of fluid in the pericardium occurs against the background of the influence of other pathologies - the disease itself rarely develops. The development of the disease occurs due to the entry of specific viral pathogens into the body and the appearance of infectious diseases. Typhoid fever, smallpox, tuberculosis, tularemia, pneumonia are diseases that negatively affect the pericardium.
Heart surgery similarly increases the risk of developing the disease. Other negative factors include rupture of a lung abscess, infective endocarditis, and immunosuppressive therapy. Radiation injury occurs under the influence of external radiation, and the degree of damage depends on the distance from the source of radiation.
All reasons can be divided into groups:
- infectious;
- tumor;
- allergic;
- radiation;
- traumatic.
Any cancer processes with metastases to adjacent organs (breasts, lungs) provoke disturbances in the heart sac. The process can be caused by injuries to the thoracic region, extensive myocardial infarction and chronic autoimmune and allergic processes (protective failures - the body begins to damage its own tissues).
Medical studies do not confirm a direct connection between the course of pregnancy and the development of pericardial effusion, however, in the later stages, moderate asymptomatic hydropericardium is possible in women. It does not cause compression of the heart and goes away after childbirth.
Symptoms in children appear after acute (streptococcal and meningococcal) inflammatory diseases.
Causes of fluid accumulation in the pericardial sac
There are many reasons for the formation of fluid in the pericardium, associated with increased production, stagnation of water in the body and increased permeability of the vascular wall. The main diseases accompanied by exudation into the pericardial sac:
- tuberculosis;
- pleurisy is an inflammatory pathology of the membrane lining the chest cavity from the inside;
- pneumonia;
- sepsis is a systemic inflammatory response to the penetration of infectious pathogens into the bloodstream;
- angina;
- scarlet fever;
- endocarditis.
All these factors cause exudative pericarditis of infectious origin. If the contents become purulent, pyopericardium develops.
Aneurysm rupture, aortic dissection, trauma, abdominal interventions (including coronary artery bypass grafting) lead to hemorrhage into the pericardial sac, which is called hemopericardium. Fluid in the heart after surgery can be either hemorrhagic or serous.
Another specific type is chylopericardium, that is, an accumulation of lymph due to the formation of a fistula (pathological connection), trauma and compression of the thoracic duct by a tumor. Cholesterol pericarditis occurs with myxedema (severe deficiency of thyroid hormones).
The development of hydropericardium is not associated with infection. Most often, transudate (non-inflammatory fluid with a low protein content) accumulates when:
- reduced level of albumin in the blood (nephrotic syndrome);
- heart failure;
- kidney disease with the development of uremia;
- pericardial tumors.
Other nonspecific reasons are:
gout;- scurvy (low vitamin C);
- exposure to x-rays, radiation;
- blood diseases;
- allergies;
- systemic connective tissue diseases (lupus erythematosus, rheumatoid arthritis, scleroderma, Wegener's granulomatosis);
- hypothyroidism;
- pregnancy (rare);
- Dressler's syndrome (especially with transmural necrosis in elderly patients with immune disorders).
Sometimes pericarditis is diagnosed in a child who is in the womb. Hydropericardium in the fetus occurs against the background of serious abnormalities that threaten the full development and life of the baby. If this pathology is detected in a pregnant woman during an ultrasound, it is necessary to think about incompatibility of the blood of mother and child, intrauterine infection, immunopathy, hypoalbuminemia, as well as congenital heart disease.
Types of effusion and characteristics
Serous
Frequency - 30-40%. Characterized by the accumulation of serous fluid . The etiology is viral. This type is usually acute and more common in children. Complaints are dominated by fever and pain. Liquid rarely accumulates in quantities of more than 200 ml. Treatment is etiological (antiviral drugs).
Serous-fibrinous
Frequency – 12%. It is represented by an accumulation of serous fluid containing fibrin threads. Caused by a viral or autoimmune disease. The course is severe, symptoms are determined by the degree of adhesion of the pericardial layers . Substernal pain, interruptions in heart function, and fever predominate. Laboratory findings: increased levels of fibrinogen in the blood.
Hemorrhagic
Frequency – 5.6-7.0%. It is represented by the accumulation of fluid with blood in the pericardial cavity. It is characterized by a severe course due to traumatic etiology and the addition of anemia. Particular symptoms are due to the presence of injury. With this form there is a high risk of developing cardiac tamponade.
Purulent
Frequency – 23-25%. Characterized by accumulation of pus (dead neutrophils). Acute purulent pericarditis is accompanied by chills, fever up to 39 degrees, and muscle aches . Pain behind the sternum is transmitted to the back. Diagnosis is based on laboratory changes (increased ESR, leukocyte and neutrophil levels).
Putrefactive
Frequency - 5.5%.
With this type, the pericardial layers melt. The diagnosis is confirmed by puncture (destroyed elastic fibers are detected, and the level of putrefactive gas is found above the exudate). Clinical symptoms are dominated by hectic fever (debilitating: daily fluctuations of up to 3-5°C, temperature rises with rapid declines are repeated several times a day), a drop in pressure, and loss of consciousness. The course is extremely severe.
Cholesterol (xanthomatous)
Frequency – 1.2%. Develops with the slow dissolution of lipoprotein complexes. Cholesterol crystals are found in the effusion. In many patients, the cholesterol level in the blood is normal , so a puncture serves to confirm the diagnosis. The course is long, complaints are minimal. The prognosis is favorable.
Exudative-adhesive
Frequency - 3.3-3.5%. It is a common outcome of other forms of pericarditis, as well as tuberculosis, rheumatism, and sepsis. Adhesions develop between the sheets, which lead to closure of the pericardial cavity. The state of health remains satisfactory for a long time, since the edges of the lungs and the mediastinum are involved in heart contractions. Complaints are often absent at rest and appear during exercise. The prognosis is favorable.
Symptoms and signs
The development of the disease does not pass asymptomatically - the patient begins to be bothered by unpleasant sensations in the heart. The first bell is a feeling of heaviness, intensified by weak aching, dull pain.
What changes in well-being are characteristic of exudative pericarditis:
- pressing and bursting pain in the heart;
- shortness of breath increasing every day;
- distortion of swallowing functions;
- temperature rise to 38 degrees;
- the appearance of hiccups;
- cold sweat.
A barking cough is another indication of the presence of pericarditis, caused by compression of the trachea due to enlarged pericardial tissue. The natural process of blood circulation is also disrupted, resulting in swelling of the face, neck, chest and legs.
Persistent disturbances of vegetative-vascular functions, especially in an advanced stage, lead to loss of consciousness, attacks of weakness and regular panic attacks associated with the fear of death. Excitation of the phrenic nerve leads to gagging.
The intensity of pain depends on the amount of fluid in the pericardial area - exudate.
When to see a doctor
Heart pain that is difficult to relieve, recurs, intensifies, or feels unfamiliar is a serious reason to consult a doctor. It cannot be tolerated - urgent medical attention is required. The nature of the symptoms cannot be determined independently; they are similar to other heart pathologies.
We recommend that you additionally read the Algorithm for providing emergency care for pulmonary edema
With pericarditis, the volume of serous fluid can increase very quickly. Tamponade may develop. Therefore, qualified assistance must be urgent. Self-medication for pain in the heart area is unacceptable, because it can cost your life.
What is the threat?
The presence of exudate in the pericardium reduces the blood supply to the heart and leads to its compression. The clinical manifestation of compression is cardiac tamponade (stop).
The effusion involves adjacent organs and causes a permanent decrease in physical capabilities. The development of suppuration and the formation of cicatricial adhesions is possible when pericarditis passes into an adhesive form , requiring surgical treatment.
Pericarditis caused by tuberculosis is extremely dangerous: mortality from advanced disease approaches 85%. Death occurs due to cardiac arrest.
Immediate consequences
Without treatment:
- Heart failure;
- Ventricular fibrillation;
- Pericardial rupture;
- Compression of the mediastinal nerves;
- Weight loss (with severe compression of the esophagus).
With treatment:
- Injury to the pericardium and puncture of the heart during puncture;
- Infection;
- Sepsis.
Remote
During treatment:
- Ventricular hypertrophy;
- Arrhythmia;
- Sinus bradycardia.
Without treatment:
- Adhesive process;
- Development of scar tissue.
Is tachycardia dangerous during pregnancy? What can it mean and does it threaten the fetus? Find out all the details!
What is the risk of atrial fibrillation, what are its symptoms and what treatment is prescribed, read in this material.
Find out what atrial fibrillation looks like on an ECG and whether this condition is felt by the patient from the following publication.
Pregnancy and childbirth
During pregnancy, the disease is somewhat more severe than usual. An increase in the volume of fluid in a pregnant woman’s body leads to the development of hydropericardium, which does not cause complaints, but under the influence of unfavorable factors quickly turns into exudative inflammation.
The disease can lead to miscarriage and pregnancy complications due to circulatory problems, so the patient should be hospitalized regardless of the general condition.
If the amount of effusion is up to 500 ml, treatment is carried out conservatively, more than 500 ml - invasively (puncture reduces the risk of complications and promotes rapid recovery).
Childbirth is carried out naturally.
Possible complications
The following complications can be expected against the background of exudative pericarditis:
- acute cardiac tamponade (accumulation of a large volume of fluid in the cavity, which prevents adequate myocardial contraction);
- circulatory disorders;
- constrictive pericarditis;
- relapse;
- death.
Pericardiocentesis may pose a risk of developing some adverse consequences, namely:
- Specifics and mechanism of development of the disorder
protect the organ from sudden overstrain under any kind of load;- reduce friction between the heart and surrounding organs;
- prevent the movement of the organ and the bending of large vessels;
- serve as a protective barrier against various infections that can come from the pleural cavity and lungs.
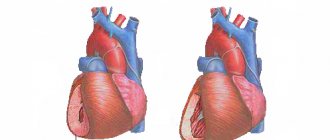
The human heart is located in a special two-layer closed “bag” called the pericardium (from the Greek peri - near and kardia - heart).
Purpose of the pericardial sac:
The pericardium itself is a fibrous layer on the outside (fibrous pericardium), and on the inside it is a serous layer. Large blood vessels arise from the outer fibrous layer of the pericardium. The structure of the internal serous layer of the pericardium is represented by two layers - parietal and visceral (epicardium).
A slit-like pericardial cavity is defined between them. It contains a certain amount of serous fluid, which is similar in composition to plasma. Its job is to wet the planes of the serous leaves and reduce their friction. In one minute, from 60 to 80 heart beats occur, during which the organ changes shape and volume, so the friction force is very large.
When diagnosing fluid in the heart, many patients do not understand what it is and where it comes from. This is the name for the serous fluid that fills the space of the pericardial region. Its amount in healthy people is insignificant.
Normally, the pericardial cavity should contain from 15 to 50 milliliters of fluid. In the process of pericarditis (inflammation of the pericardial sac), as a result of increased exudative processes, the amount of serous fluid in the pericardial cavity begins to increase significantly
The pericardial cavity fills, a large amount of exudate puts excess pressure on the organ. Contraction of the chambers and diastolic filling of the ventricles is difficult. The organ cannot function normally (critical decrease in the volume of ejection).
Such changes lead to the development of hemodynamic and microcirculation disorders, which, in turn, can provoke heart failure and, in some cases, complete cardiac arrest. If the development of such a syndrome occurs quickly, then the clinic develops rapidly. As a result, the outcome is unpredictable.
Disease in children
Effusive pericarditis in children occurs in 1% of cases, of which 60% have a viral etiology. Downstream, the acute form predominates. Pericarditis in children is characterized by rapid accumulation of effusion, prolonged fever up to 39 degrees, refusal to eat, redness of the face and neck. Children have more common symptoms (chills, insomnia, loss of appetite) than adults.
The treatment tactics are no different, but the doses of drugs are selected depending on weight. The indication for a puncture is a deterioration in the baby’s general condition.
Causes and types
Depending on the cause of the disease, pericarditis can be classified as follows:
- Pathologies caused by exposure to an infectious pathogen (bacterial, tuberculosis, streptococcal, viral, chlamydia, dysentery, typhoid, syphilitic, fungal, parasitic, etc.). They occur under the influence of toxins from pathogenic organisms, causing inflammation of the pericardial sac.
The diagnosis of pericarditis is made on the basis of the clinical picture, data from biochemical blood tests, data from electrocardiograms and echocardiograms, and x-ray examination. In more complex cases, a study is performed using computer or magnetic resonance imaging of the heart. The most reliable data is obtained using an echocardiogram both at the stage of diagnosis and to assess dynamics during treatment.
The blood picture is characteristic of the inflammatory process:
- increasing the reaction rate of red blood cells;
- leukocytosis;
- reactive protein and more.
Troponin screening is appropriate. The presence of troponin in the blood may indicate muscle destruction. If necessary, resort to puncture of the pericardial cavity. This procedure is carried out for diagnostic purposes. With its help, samples of the contents of the cavity are obtained, which makes it possible to detect the causative agent of the process. The procedure is also effective in routine treatment.
Diagnosis: techniques used to determine the presence of effusion
The patient’s treatment begins with studying the characteristic symptoms, if they coincide, you should immediately make an appointment with a cardiologist. A visual sign of pericardial effusion is bulging of the chest wall (anterior) and jugular veins . To confirm the diagnosis, the doctor sequentially prescribes a number of studies:
- ECG;
- EchoCG;
- chest x-ray;
- biopsy and puncture of the pericardium;
- tomography.
A physical examination of the heart can help determine the type of pericarditis based on heart murmurs. In the exudative form, dull noises without an element of friction can be traced.
How do the boundaries of the heart change? An x-ray shows an image of altered configurations of the heart: an increase in fluid accumulation bends the cardiac contour, making the heart more round, and the shadow of the bundle of blood vessels on the x-ray is shortened. There is a general increase in the boundaries of the heart.
In the acute stage, attacks of loss of consciousness occur, requiring an urgent call for an ambulance. The patient is transported in a semi-sitting or sitting position to facilitate breathing.
History, patient complaints
The patient's medical history indicates how long the disease has been, the connection with hypothermia, the presence of autoimmune diseases, the nature of the fever and the persistence of symptoms.
Typical complaints:
- Chest pain;
- Dyspnea;
- Cough;
- Frequent heartbeat and decreased blood pressure;
- Worsening when lying down;
- Insomnia.
If there is a large accumulation of fluid in the pericardial cavity, the patient takes a forced sitting position (or sleeps while lying on a high pillow).
Physical examination
- Examination : swelling of the neck veins, pallor, ascites;
- Palpation - displacement of the apical impulse down and to the left or its disappearance, dense swelling of the legs, enlargement of the liver;
- Percussion - an increase in the relative dullness of the heart while reducing the absolute dullness. With a significant accumulation of effusion, absolute dullness may not be detected, and in the supine position it may increase slightly. Relative dullness of the heart with effusion pericarditis is expanded to the right, left and down;
- Auscultation of the heart - dull tones. Pericardial murmur is heard regardless of the amount of fluid and intensifies at the height of inspiration. From the lungs - moist rales.
Instrumental examinations
What changes on the ECG are characteristic of exudative pericarditis? Electrocardiography can reveal:
- Reduced height of R and P waves;
- Decrease in the ST segment below the isoline;
- When the amount of effusion is 50-100 ml, there are often no changes on the ECG.
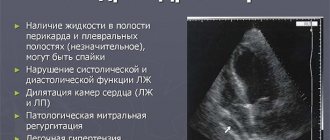
ECHO-KG allows:
- Detect effusion and determine its quantity;
- Diagnose fibrin deposits and the presence of adhesions;
- Identify cardiac tamponade.
X-ray is effective when fluid accumulation exceeds 200 ml. Detectable signs:
- Enlarged cardiac shadow with a predominance of transverse size;
- Disappearance of waist heart;
- Displacement of the esophagus;
- Poor visualization of the pulmonary roots;
- Thickening of the vascular bundle.
To determine the nature of the exudate, a pericardial puncture is performed.
Pericarditis and pericardial effusion
Pericarditis ( inflammation of the pericardium ) can occur with a variety of diseases, including viral or bacterial infection, metastatic tumors, connective tissue diseases, myocardial infarction, uremia, and heart surgery.
Rice. 11-1. Acute pericarditis with widespread ST segment elevation in leads I, II, aVF, V2-V6 with reciprocal ST segment depression in lead aVR.
Damage to the atrial myocardium is indicated by elevation of the PR segment in lead aVR with reciprocal depression of the PR segment in the left precordial leads and lead II. (From: Goldberger A.
L Myocardial infarction: Electrocardiographic Differential Diagnosis. – 4th ed. – St. Louis: Mosby, 1991.)
Differences between pericarditis and the acute stage of myocardial infarction
The electrocardiogram with pericarditis resembles the acute stage of myocardial infarction. In the early stages of acute pericarditis, ST segment elevation usually occurs (Fig. 11-1) as a consequence of inflammation of the superficial part of the heart, which is not uncommon in pericarditis.
The main difference between ST segment elevation in pericarditis and acute myocardial infarction is their location . ST segment elevation in acute myocardial infarction usually occurs in the anterior or inferior leads due to the limited area of myocardial infarction.
The pericardium covers the entire heart, so changes in the ST-T complex in pericarditis are usually more widespread (in the anterior and inferior leads): for example, ST segment elevation in leads I, II, aVL, aVF, V2-V6 in Fig. 11-1.
| In Fig. Figure 11-1 shows small but diagnostically important changes in repolarization in acute pericarditis. |
In acute pericarditis, not only ventricular repolarization (ST segment) is impaired, but also atrial repolarization. The latter corresponds to the PR segment (from the end of the P wave to the beginning of the QRS complex).
Inflammation of the pericardium often produces electrical flow through the atrium, typical of injury, as evidenced by elevation of the PR segment in lead aVR, as well as depression in the other limb leads and left precordial leads (V5 and V6).
Thus, in acute pericarditis, the PR and ST segments are usually deviated in opposite directions (the elevation of the PR segment is often no more than 1 mm in lead VR and slight depression of the ST segment in the same lead). In other leads, depression of the PR segment and elevation of the ST segment are possible.
After ST segment elevation in acute pericarditis, negative T waves are sometimes formed (Fig. 11-2).
Rice. 11-2. Subacute stage of pericarditis. Widespread T wave inversion in leads I, II, III, aVL, aVF, V2-V6.
The sequence of ST segment elevation and T wave inversion is the same as in myocardial infarction. Sometimes negative T waves caused by pericarditis completely disappear over time and the electrocardiogram returns to normal. Long-term persistence of T-wave inversion is also possible.
The ECG changes in acute pericarditis and acute myocardial infarction are very similar , as ST segment elevation with T wave inversion may occur in both cases. However, ST-T changes in pericarditis are usually more widespread compared with the limited changes in myocardial infarction.
Another important difference is the absence of pathological Q waves in pericarditis.
In myocardial infarction, pathological Q waves are the result of myocardial death and, accordingly, the disappearance of positive depolarization potentials (see section “Ischemia and myocardial infarction”).
Pericarditis usually involves only superficial inflammation and not myocardial necrosis. Thus, pathological Q waves never occur in isolated pericarditis .
Pericardial effusion
Pericardial effusion is the accumulation of fluid in the pericardial cavity. In most cases, this occurs with pericarditis.
However, sometimes pericardial effusion is possible in the absence of pericarditis , such as with myxedema ( hypothyroidism ) or cardiac rupture.
The main clinical significance of pericardial effusion is the risk of cardiac tamponade, when fluid “suffocates” the heart, which can lead to a decrease in blood pressure and even cardiac arrest.
The most common ECG finding of pericardial effusion (with or without tamponade) is low QRS voltage, which is likely due to disruption of the conduction of electrical impulses in the heart due to the fluid surrounding it.
The section “Enlargement of the atria and ventricles” describes the voltage criteria for myocardial hypertrophy. Low voltage is indicated when the amplitude of the QRS complexes in each of the six limb leads does not exceed 5 mm (0.5 mV).
With low voltage in the limb leads, low voltage in the chest leads is possible - the amplitude of the QRS complex is no more than 10 mm in each of the leads V1-V6.
For example, in obesity, low QRS voltage is possible due to fatty tissue lying between the heart and the chest wall. In patients with emphysema, the airiness of the lungs is increased, which contributes to the isolation of the heart.
The most common causes of low electrocardiogram voltage are obesity, anasarca (generalized edema) and pulmonary emphysema.
If low voltage QRS complexes are detected (especially against the background of sinus tachycardia), the presence of pericardial effusion should be suspected, as this can cause cardiac tamponade.
Electrical alternans is another important sign of pericardial effusion and cardiac tamponade (Fig. 11-3).
Rice. 11-3. Electrical alternans in cardiac tamponade. Alternation of the axis of the P-QRS-T complex during successive contractions of the heart, which is associated with its oscillatory movements in the pericardial fluid; relatively low voltage QRS complexes and sinus tachycardia.
In this case, a typical shift in the average electrical axis of the QRS complex from one heart contraction to another is associated with a change in the position of the heart in a large volume of fluid. Electrical alternans in combination with sinus tachycardia is one of the diagnostic signs of cardiac tamponade . However, this sign is not detected in every patient.
| So, in acute pericarditis, the electrocardiogram shows signs of widespread damage with ST segment elevation in the anterior and inferior leads, sometimes with T wave inversion in these leads. However, pathological Q waves do not occur in isolated pericarditis. Pericardial effusion is one of the causes of low wave voltage on the electrocardiogram. |
Source: https://cardiography.ru/izmeneniya_ekg_pri_zabolevaniyah/perikardit_i_perikardialnyiy_vyipot/
Treatment tactics
Treatment of the acute period is carried out in a hospital with bed rest.
After acute symptoms subside, patients are observed by a cardiologist until complete recovery. If there is a small amount of fluid in the pericardial cavity, a sick leave certificate is issued for 2-4 weeks, the total duration of therapy is 6 weeks. If the volume of effusion is significant, sick leave is extended to 6 weeks, therapy continues for up to 3 months.
In case of acute form, sick leave is issued until complete recovery (1-2 weeks), in case of subacute and chronic exudative pericarditis - until relief of the main clinic (from 2 to 4 weeks). The general treatment time for subacute and chronic forms increases to 3 months.
Conservative
Monitoring includes recording the dynamics of changes in heart rate, arterial and central venous pressure. The patient is on bed rest and taking a course of medications .
If the general condition is satisfactory and there is no threat of tamponade, diuretics are prescribed. They are most effective when fluid accumulation is less than 500 ml. The drugs of choice are loop diuretics, which increase urination (Lasix, torsemide). However, the effect of diuretics is hampered in the presence of diseases of the urinary system.
Physiotherapeutic procedures are not indicated for this disease due to the risk of increased proliferative processes.
In the presence of an infectious process, antibacterial therapy (cephalosporin antibiotics), including amoxilav or vancomycin, is prescribed. The ineffectiveness of treatment leads to a change in tactics - antibiotics of the aminoglycoside group are prescribed. Tuberculosis patients are prescribed streptomycin with the administration of medicinal substances through a catheter (in severe situations). Fungal infections require the use of flucytosine and amphotericin in the form of a dropper or intravenously.
After the inflammation is relieved, non-hormonal anti-inflammatory drugs are prescribed - ibuprofen and aspirin. Breathing problems will require enriching the body with oxygen by taking breathing mixtures (special mixtures of nitrogen and oxygen).
The dosage of all drugs is determined by the doctor based on the general condition and the amount of exudate.
Untreated effusion pericarditis becomes chronic (fluid accumulation lasts more than 6 months), which can only be corrected by surgical intervention. Surgery involves excision of part of the heart sac.
Dieting: what is the best way to eat?
Dietary nutrition is aimed at overall strengthening of the body and reducing intoxication. The diet consists of a high protein content, an optimal amount of fluid (up to 2 liters per day) and a reduced salt content. Calorie content – up to 2500 kcal.
Invasive treatment
Puncture (pericardiocentesis) is a puncture of the pericardium with a puncture needle to remove exudate. The puncture is performed slowly and after pain relief.
The resulting liquid is sent for laboratory tests. During puncture, medicinal solutions and antiseptics can be injected into the pericardial cavity.
Large accumulations of fluid - more than 200-300 ml - will require puncture and removal of effusion . Indications:
- Cardiac tamponade;
- Fainting;
- Tachycardia;
- Pressure drop;
- Thread-like or paradoxical pulse;
- Diffuse cyanosis.
How does recovery proceed after fluid is removed from the pericardium?
Removal of fluid is accompanied by symptoms associated with restoration of the position of the heart (cough, pain, pressure lability). Rehabilitation is carried out in bed and includes protein-rich nutrition, rest and good sleep. Most patients switch to ward mode within 3-5 days.
If the fluid is purulent, the pericardium must be sanitized - the cavity of the bag is washed with an antiseptic solution, and in recurrent cases it is possible to install a permanent catheter to remove the fluid.
Treatment of pericarditis
Before prescribing treatment, the patient is examined. Diagnosis of pericarditis begins with a history. They carry out inspection, listening, tapping.
A blood test is prescribed, the results of which determine the presence of inflammation.
An ECG and x-ray of the heart are performed. Irregularities in its operation are detected, as well as changes in shape, size and position.
The main method of research for pericarditis is echocardiography, which reveals fusion with the myocardium, the presence of fluid, and compaction of the pericardium. In severe cases, MRI and CT are used.
Treatment of a disease such as pericarditis depends on the cause that caused it. It is aimed at eliminating inflammation and treating the underlying disease. Medicines and, if necessary, surgery are used.
For infectious pericarditis, antibiotics are prescribed, the action of which is aimed at the microorganisms that caused the disease. Pain is relieved with analgesics. Treatment of acute pericarditis is aimed at eliminating symptoms.
Also used:
- Non-steroidal anti-inflammatory drugs with an analgesic effect (Diclofenac, Voltaren, Ibuprofen).
- Corticosteroid hormonal anti-inflammatory drugs (Dexamethasone, Prednisolone).
- Antiarrhythmic drugs (Amiocordin, Rotaritmil).
- Diuretics (Hypothiazide, Veroshperon, Lasix).
In most cases, the patient is given first aid, hospitalized, and treatment will continue in the hospital.
Adhesions in the membrane are successfully removed with a laser. The pericardial cavity is surgically opened to remove excess fluid (exudate). When treating severe cases of pericarditis, pericardiectomy is performed - excision of the membrane.
Treatment with folk remedies is used only as prescribed by a doctor after drug therapy. It is effective for dry infectious pericarditis. Anti-inflammatory, antiseptic, and sedative agents are used. Young pine needles, valerian root, hawthorn, birch catkins and others are used in recipes.
Prospects for therapeutic measures and the patient’s condition
Patients who have undergone surgery or treatment are advised to limit physical and mental stress, reduce salt intake, and receive a flu vaccination every year. Among the rehabilitation measures, resort and sanatorium treatment, frequent rest and dietary nutrition are equally distinguished.
Surgical intervention is dangerous: mortality during pericardiectomy is from 5 to 12%, depending on the presence of unrecognized myocardial fibrosis before the operation.
Exudative forms without complications demonstrate positive dynamics of treatment and the patient’s return to normal life. In 30% of cases, when inflammation spreads to the myocardium, arrhythmia and tachycardia are formed. The overall prognosis is moderately unfavorable , especially if therapeutic treatment is delayed.