A bit of terminology
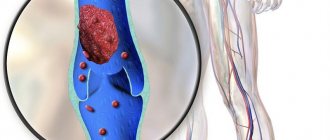
The ductus arteriosus is a small vessel that connects the aorta to the pulmonary artery. It is through it that blood circulation occurs in children who have not yet been born. After they are born and take their first breath, this vessel closes. In its place, a cord of connective tissue forms.
However, sometimes the duct does not close. Because of this, the heart and lungs of the crumbs work worse. If PDA is left untreated, the newborn may die. For this reason, all parents should be aware of the possibility of its development and be able to independently determine it based on the symptoms.
The stimulus for closing the ductus botallus is an increase in oxygen concentration in babies
Causes of patent ductus arteriosus in premature newborns
Risk factors for PDA based on meta-analyses and individual studies
Increase the risk of patent ductus arteriosus
- RDS
- Lower body weight and gestational age
- Hypotrophy
- Surfactant treatment
- “Liberal” fluid administration
- Antenatal administration of maternal indomethacin
- Mother's appointment MgSO4
- Infections
- Thrombocytopenia
- Phototherapy?
Reduce the risk of patent ductus arteriosus
- AGK
- Postnatal
- GKS
- Fluid restriction
- Caffeine citrate
- PTV
Pathogenesis/hemodynamics of patent ductus arteriosus
In utero, the duct is maintained open by high concentrations of circulating prostaglandins (especially prostaglandin E2) and nitric oxide.
Postnatal closure of the AP is facilitated by several mechanisms:
- increase in PaO2;
- decrease in blood pressure inside the duct;
- decreased concentration of prostaglandin E2 due to separation of the fetus from the placenta and increased excretion through the lungs;
- decrease in the number of prostaglandin E2 receptors in the duct wall.
In premature newborns, sensitivity to the vasoconstrictor effect of oxygen is reduced, and sensitivity to the vasodilators of prostaglandin E2 and nitric oxide, on the contrary, is increased; as a result, the AP is more likely to remain open, leading to shunting, which may contribute to important hemodynamic consequences. Depending on the ratio of pressure in the pulmonary artery and the aorta, a continuous shunt is recorded, most often a left-right one, since in most cases the pressure in the aorta is greater than in the pulmonary artery. Less commonly, right-left (sometimes PLH develops in premature newborns) and bidirectional shunting are observed.
A left-to-right shunt increases pulmonary blood flow, leads to an increase in pressure in the pulmonary capillaries, sweating of fluid and, ultimately, pulmonary edema, inactivation of surfactant, and sometimes the development of true pneumonia. An increase in venous return to the heart causes dilatation of its left sections, primarily in the left atrium. The degree of enlargement of the left atrium relative to the aortic root is one of the reliable indicators of the size of the shunt. Another important aspect of the clinical significance of PDA is the depletion of the systemic circulation, which leads to hypoperfusion of the kidneys, intestines and brain. These organs receive less blood flow due to a combination of low perfusion pressure and local vasoconstriction. With prolonged functioning of the patent ductus arteriosus, signs of circulatory failure may develop.
However, it is now believed that patent ductus arteriosus in preterm infants is a physiological condition in which a right-to-left shunt occurs in the first days after birth, when PVR is high, and a left-to-right shunt in cases of severe lung disease, when increased pulmonary blood flow would be beneficial ( increases pulmonary perfusion).
Timing of duct closure
This usually happens within two days after the baby is born. In the first few hours of life, in completely healthy full-term babies, blood shunting is possible, that is, movement around a certain section of the vessel:
- From left to right. It appears immediately after the baby is born and lasts about 1 hour.
- Two-way. Lasts for 180 minutes.
- From right to left. It is detected within 15-21 hours after the birth of the baby.
Complete closure of the vessel occurs within 2-3 weeks after the baby is born. Sometimes (when the baby is premature) this happens after 6-8 weeks. If after 3 months the duct remains open, then the newborn is diagnosed with PDA.
If there is a positive dynamics of vessel closure at 15 weeks, then this phenomenon is not considered a pathology
Types of disease and stages of its development
The following types of patent ductus arteriosus are distinguished:
- isolated;
- combined, that is, combined with narrowing of the pulmonary artery or other pathologies.
Stages of development of the ductus botallus:
| Stage | a brief description of |
| Primary adaptation | Lasts up to 3 years. Signs of cardiac PDA are clearly expressed. If there is no treatment for severe pathology, the baby may die. |
| Compensation | Lasts up to 20 years. The symptoms of the disease are mild, but functional overload is observed when the heart muscle is working. |
| Hardening of pulmonary vessels | During it, pulmonary hypertension develops. |
Stages and degrees
The process can be caused by various factors, and therefore the pathology is divided into 2 main types - functional closure and anatomical. The first stage is in most cases observed in full-term babies and occurs within 15 hours after birth. The second stage continues over the next 2-8 weeks.
The main stages of disease development:
| Stage | Flow characteristics/characteristics |
| Primary adaptation | The process is accompanied by pronounced symptoms. It is formed in the first 3 years of a child’s life. In this case, there is a violation of the sucking reflex, excessive pallor of the skin, shortness of breath occurs, and angina develops. With complications, the condition leads to death in half of the cases. |
| Compensation stage | Pathology develops from 3 to 20 years. Symptoms are mild. The condition is characterized by an increase in blood volume and, as a result, an increase in blood pressure. |
| Vascular sclerosis | The disease causes persistent hypertension. In the vast majority of cases, the pathology leads to death. If all recommendations are followed, the patient's life expectancy does not exceed 35 years. |
What causes the occurrence of pathology?
Why the ductus arteriosus does not close is not known exactly, but scientists have proposed possible reasons why this happens:
We recommend reading: Patent foramen ovale in a child
- premature birth;
- a woman has contracted rubella, influenza, herpes, enterovirus, mumps, Coxsackie virus or CMV during pregnancy;
- her use of medications that have a negative effect on the fetus;
- the presence of diabetes mellitus or hypothyroidism;
- consumption of alcoholic beverages and drugs by the expectant mother;
- radiation impact on it;
- low weight of the baby (less than 2 and a half kilograms);
- genetic predisposition;
- chromosomal abnormalities. For example, Edwards, Down or Shereshevsky-Turner syndrome;
- the presence of other congenital disorders;
- oxygen starvation.
It is assumed that PDA may occur if a woman had severe toxicosis and other complications during pregnancy
What symptoms can be used to identify illness in a baby?
Doctors sometimes call the Battalian duct a white heart defect. This is due to the fact that the skin of a newborn with this disease always has a pale tint. In addition to this, the presence of pathology in an infant is indicated by such signs as:
- increased sweating;
- too little weight gain;
- cardiopalmus;
- fast fatiguability;
- sleep disturbance;
- dyspnea;
- difficulties with feeding.
The occurrence of these symptoms is associated with heart failure, which appears due to congestion of the blood vessels of the lungs. This is caused by the fact that the blood does not rush to the organs, as it should normally happen, but returns to them.
The severity of the disease is influenced by the diameter of the ductus arteriosus. So, if it is small in size, then it will be asymptomatic. If the dimensions of the vessel correspond to the following values: in babies born on time - 9 mm, and in babies born ahead of schedule - 1.5 mm, then the following symptoms will be added to the above symptoms:
- hoarseness of voice;
- delay in both mental and physical development;
- cough;
- weight loss of the newborn;
- frequent occurrence of pneumonia and bronchitis.
Symptoms
In most full-term Botall babies, the duct does not manifest itself in any way. This is due to the fact that blood deprived of oxygen and enriched with carbon dioxide does not enter the left side of the heart and the aorta. Therefore, none of the body systems experiences oxygen starvation. With a PDA diameter of 4 mm or more, only a systolic murmur is usually heard. If this value is more than 9 mm (for premature babies - more than 1.5 mm), the following symptoms become noticeable:
- fast pulse (from 150 beats per minute);
- rapid breathing, lack of oxygen during active activities;
- coughing, hoarse voice;
- fatigue, sleep disturbances;
- difficulty breastfeeding;
- slow weight gain;
- frequent pneumonia and bronchitis, starting from an early age;
- developmental delay.
If the patent ductus arteriosus is wide enough, or it is present in a premature baby, the following signs are observed:
- significant increase in heart volume;
- increased and increased heart rate (this is tachycardia);
- increased blood pressure, noticeable by the pulsation of large vessels even with the naked eye;
- clearly audible heart murmurs;
- paleness of the skin caused by spastic contractions of arterioles;
- over time, the appearance of an elevation in the sternum.
Child developmental delay is a symptom of patent ductus arteriosus
Parents should remember that timely treatment of patent ductus arteriosus will be much easier than trying to fix everything if it is detected late. If a child is not gaining weight well, avoids active games, does not get enough sleep, often gets respiratory tract infections, or notices bluish skin on the legs after physical activity, it is necessary to be examined by a doctor.
Diagnostics
First of all, to confirm or refute the diagnosis, the doctor performs auscultation. He uses a special device (steothoscope) through the chest to listen to the newborn's heartbeat for the presence of murmurs. If they are, then he prescribes additional examinations.
| Procedure | PDA symptom |
| ECG | heavy load on the left ventricle |
| Ultrasound | an increase in the size of the atrium and left ventricle |
| chest x-ray | expansion of the vascular bundle and cardiac borders; changes in the lungs |
In addition, the following is carried out:
- Doppler echocardiography. During it, the direction and volume of blood that is discharged through the battalus duct is determined;
- cardiac probing. During it, the pressure in the left ventricle is measured.
The presence of noises in the first 48 hours of a baby’s life is the norm. During this time, the ductus arteriosus is just beginning to close. After 2 days, a band of connective tissue should already form in its place, and the heart murmurs will stop
Treatment methods
Depending on the patient’s age, severity of symptoms, size of the duct and the presence of other pathologies, the doctor may choose one of the following treatment methods:
- Medication. It is used to identify defects in infants who are not yet a year old. In children, in the absence of pronounced manifestations of pathology, anti-inflammatory drugs (for example, Indomethacin) are prescribed. They block substances that prevent the formation of a banner naturally. In addition to them, cardiac glycosides can be prescribed, as well as diuretics necessary to reduce the load on the baby’s heart; antibiotics and diuretics.
- Catheterization. The method consists of inserting a catheter into a large artery and bringing it to the Batallo duct. After that, a device is installed inside the PDA that interrupts the blood flow. This procedure is absolutely safe. It can be performed on both adults and children if they are already 1 year old.
- Ligation of the duct by clamping the vessel using a special clip or suturing the duct. Surgical intervention is allowed for children from 2 years of age.
The operation, as a rule, always gives a good result
Treatment
Medication
Treatment with medications is possible for minor manifestations of this disease, which proceeds without complications, if there are no other congenital heart defects. In most cases, such therapy is applicable to infants. The following drugs are prescribed:
- Nonsteroidal anti-inflammatory drugs. They reduce the synthesis of prostaglandins, which prevent the occlusion of the patent ductus arteriosus. The most commonly used are Indomethacin, Ibuprofen, and Nurofen.
- Diuretics. These medications have a pronounced diuretic effect, which leads to a slight decrease in the total volume of circulating blood. This takes some of the load off the heart muscle and eliminates swelling. Such drugs include Digoxin, Lasix, Furosemide, Hypothiazide.
- Cardiac glycosides. These medications distribute excess stress on the heart by increasing diastole time, giving the muscles additional rest. The most common of them are “Izolanid” and “Celanid”.
"Nurofen" is used as a treatment for ductus botanus in children
If a course of drug treatment does not help a child, doctors, if possible, prescribe it again. In the same case, when this does not produce any results, more “aggressive” methods are used. These include cardiac catheterization and surgery. The latter is indicated for large diameters of the Botallian duct.
Catheterization
This procedure has relatively low risks and good effectiveness. Moreover, it does not require large incisions of the skin, since the catheter is inserted into an artery or a fairly wide vein. Nowadays, this method is increasingly preferred. Catheterization is indicated for children over one year of age.
The success of the procedure largely depends on the professionalism of the doctor who performs it. Therefore, it would be frivolous to assume that catheterization always proceeds without complications. Thus, there are risks of bleeding, thrombosis, damage to the blood vessel used, the development of infectious pathologies, allergic reactions to the contrast agent and other serious consequences.
Operation
Surgery can be performed regardless of the child’s age. Of course, it is done in newborns only in cases of extreme necessity (usually in the presence of complications, other congenital heart defects or a large diameter of the Botallian duct). The effectiveness of the operation increases significantly if it is performed on a child under 3 years of age.
This procedure is rarely fatal and allows the duct to close completely. In very rare cases, PDA appears again after a few years. One of the disadvantages of surgical intervention is the need for subsequent rehabilitation (sometimes up to 2 months).
The consequences of the disease depend on the age of the patient. In young children, in most cases, all symptoms disappear immediately, which gives them the opportunity to lead a full life. But even if treatment for patent ductus arteriosus is successful, the child will need to undergo regular examinations with a doctor for another year.
Indications and contraindications for ligation of the duct
Surgery is recommended in cases where the PDA:
- accompanied by aortic stenosis;
- the baby often suffers from pneumonia or bronchitis;
- pressure increased in the pulmonary vessels.
- the baby has heart failure;
- drug therapy did not give the desired result;
- The baby was found to have signs of blood stagnation in his lungs.
The operation cannot be performed if:
- serious pathologies of the liver and kidneys;
- throwing blood into the aorta rather than out of it.
conclusions
There is currently no evidence that medical or surgical treatment of patent ductus arteriosus reduces mortality, incidence of BPD, necrotizing enterocolitis and other diseases. Prospective studies show that the majority of ALI detected immediately after birth close on their own, without treatment. It is likely that the presence of LI and the possibility of multidirectional shunting along it will in some cases be useful for premature newborns. However, treatment with indomethacin, ibuprofen or surgical ligation are themselves associated with significant side effects. Thus, the available evidence suggests that the best approach for the patient at this time is not aggressive early treatment of a hemodynamically significant PDA, but an individualized, largely conservative approach. Surgical ligation of the duct remains a treatment reserve for patients with a patent ductus arteriosus who develop congestive heart failure or continue to require mechanical ventilation not associated with other causes (for example, BPD).
Prognosis and possible complications
The ductus batallus should close completely in the first 3 months of a baby’s life. If this does not happen, then it will not happen without the use of certain medications. Some statistics!
- In 75-81% of cases, after several courses of drug injections, the pathology is eliminated.
- After surgery, the duct closes in everyone, but after some time it may open again.
- In the absence of therapy, pulmonary hypertension develops already at 2-3 years of age.
- Many people who do not have PDA treated live no more than 40 years.
Pulmonary hypertension is not treatable
Non-closure of Botall's anastomosis
During intrauterine development, fetal breathing using the lungs is impossible.
Viability is maintained by the placenta and the circulatory system. The fetus has an accessory vessel, the ductus botallus. It connects the aorta to the pulmonary artery. After birth it becomes overgrown. PDA is a congenital defect that is most often diagnosed in premature infants. In girls, this disease is detected 2 times more often.
Its share in the structure of all congenital defects reaches 10%. It is often combined with other developmental anomalies. In 5–10% of cases, aortic stenosis, coarctation and septal defects are simultaneously detected.
The length of this anastomosis between the pulmonary artery and the aorta is 12 mm with a width of 2–10 mm. When the flow rate is insignificant, compensation occurs. Such people can live up to 40 years. In more severe cases, emergency surgery is required.
PDA is characterized by increased pressure in the pulmonary artery system. Depending on its level, there are 4 degrees of severity of the defect.
In mild forms of this pathology, the pressure in the pulmonary artery does not exceed 40% of the systemic one.
At grade 2, this figure ranges from 40 to 75%. Severe pulmonary hypertension is observed if the pressure in the PA exceeds 75% of the systemic one.
At stage 4, a right-to-left shunt of blood is observed. This indicates that the pulmonary artery pressure is equal to or greater than the systemic pressure. There are also 3 stages of development of the defect:
- primary adaptation;
- relative compensation;
- sclerosis.
The first stage lasts 2–3 years. The second is up to 20 years old.
What are the dangers of white heart disease?
In the absence of proper treatment, the baby may experience the following complications:
- bacterial endocarditis;
- myocardial infarction;
- pulmonary edema;
- aortic rupture;
- pulmonary hypertension;
- heart failure;
- cerebral ischemia and hemorrhage.
PDA is being treated. The main thing is to detect it in time. Parents need to closely monitor the baby’s condition, and if he develops any symptoms indicating the development of pathology, consult a doctor.