Among the many modern medical devices, the defibrillator is especially commonly used. How it works and what it is is necessary for those people who are planning a surgical operation to implant the device to know.
A defibrillator is a medical device that was created for use in electrical impulse therapy. Often used for various rhythm disorders that are accompanied by too high heart rates. The first experiments with defibrillation were carried out in 1899 on dogs. Their main goal was to study the mechanism of death from electric current, since the very concept of defibrillation was not yet fully formed. This was done by Hooker's team in 1932. As a result of their experiments, the possibility of performing electroshock resuscitation was proven.
The first autonomous defibrillator was created in the Soviet Union in the mid-50s by Klimov and Eskin, but for various reasons it turned out to be impossible to widely popularize the experiments.
The first prototype cardioverter-defibrillator weighed about 27 kg. It was created by Baruch Berkowitz, while the main development of the device is carried out by Zolla Bernard Lown. Using such a device, a pulse with an energy of 100 J was created, which could be used on an open heart. In order for the shock to be used through a closed chest, an average pulse of 300 J was applied.
Video How does a defibrillator work? — Theories in 1 minute | BrainTime
What is this procedure and who performs it?
The technique of this procedure is a short-term effect of current on the electrical activity of the heart muscle.
The effect of direct current goes through the anterior chest wall to the myocardium. As a result of this, heart rhythm disturbances are corrected, and the heart begins to work in the correct mode - 60-80 beats per minute and at regular intervals.
Thus, a powerful discharge simply inhibits the activity of abnormal electrical impulses in the myocardium, and brings the rhythm of its contraction to normal - sinus.
An electrical discharge is applied externally using two defibrillator electrodes, generating a bipolar pulse. They are first moistened in a special solution and then applied directly to the patient’s chest.
There are two types of stimulation of cardiac activity using electric current:
- Defibrillation.
- Cardio version.
Defibrillation is done to normalize the ventricular rhythm, and cardioversion is performed to correct the atrial rhythm.
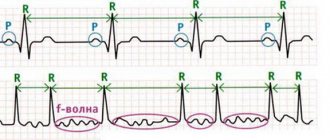
The difference between cardioversion and electrical defibrillation lies in the specifics of the discharges used: in the first case, they are synchronized by the electrocardiogram (ECG) with ventricular complexes, in the second, they are not synchronized.
In addition, cardioversion is carried out routinely, in a clinical setting, while electrical defibrillation is a resuscitation method performed to prevent possible cardiac arrest and save lives. You need to act very quickly, as the risk of biological death increases with every minute.
The procedure does not require special preparation, since the primary goal is to preserve the patient's life. It is performed using a defibrillator. All manipulations must be done by an emergency physician, resuscitator or cardiologist. The patient's behavior is characterized by loss of consciousness. First, a discharge of 200 joules (J) is applied, then the voltage can reach up to 360 J.
Key mistakes in defibrillation
- No resuscitation measures were carried out before the start of defibrillation, or a long break was taken after cardiac massage.
- The electrodes were pressed against the chest with insufficient force.
- The patient was diagnosed with small-wave fibrillation and the necessary measures were not taken to enhance the energy resources of the heart muscle.
- The discharge voltage was chosen incorrectly (too high or, conversely, too low).
Thus, only people knowledgeable in this matter can perform defibrillation. Using this method of eliminating fibrillation, it is possible to save patients in different conditions and under different circumstances.
4.67 Aug. rating ( 92 % score) – 9 votes – ratings
Types of defibrillation
There are three types of emergency defibrillation. Let's take a closer look at each of them.
Mechanical (precordial stroke)
This is a sharp blow with a fist to the victim’s sternum with the aim of shaking the chest and transmitting a mechanical impulse to the fibrillating heart. This method restores the normal functioning of the heart and serves as an external mechanical pacemaker. This method should be used only during the first two minutes of fibrillation, after first checking the presence or absence of a pulse in the victim’s neck.
If there is no pulse, it is recommended to raise the victim’s legs for a few seconds to allow blood to flow to the heart and apply a precordial blow. If the pulse has not recovered, then the procedure should be repeated, but no more than 2-3 times.
Electrical defibrillation
Electrical defibrillation is carried out using a special device - an automatic defibrillator, which can be portable or stationary. Currently, biphasic type devices are most in demand. Biphasic currents are more effective in treating ventricular fibrillation than monophasic ones, consume less energy and cause less harm to the patient.
Electrodes for external defibrillation are placed on the patient's chest in such a way that a short-term electrical pulse discharge passes from one electrode to another along a path corresponding to the electrical axis of the heart.
Medication
It is used when it is not possible to perform electrical cardiac stimulation. The chemical defibrillation method involves intracardiac injection of antiarrhythmic drugs. The drug effect can occur after the drug has been distributed into the muscle, usually after a few minutes.
After the injection is administered, chest compressions begin.
Click on photo to enlarge
If these measures are ineffective, the next step is intracardiac administration of cardiac stimulants.
Local anesthesia and venous access.
After the surgical site has been treated and the patient is covered with sterile surgical drapes, local anesthesia is administered. As a rule, surgeons use novocaine as an anesthetic, but it is possible to use lidocaine, naropin and other local anesthetics. After anesthesia, a skin incision is made. Its length is about 5 cm. The incision is localized, most often, in the left subclavian region. After the incision, the surgeon creates a “pocket” for the future cardioverter-defibrillator under the pectoralis major muscle, in its thickness, or above it. Next, you need to gain access to the subclavian vein. The surgeon punctures the subclavian vein as many times as electrodes are planned to be installed (one, two or three). The puncture is performed according to the Seldinger method: a vein is located with a needle, then a flexible metal conductor is inserted through the needle, and the needle is removed. Next, plastic tubes—introducers—are inserted along the guidewire.
Briefly about cardioversion
Cardioversion (electrical pulse therapy) is a procedure performed for patients with pathophysiological heart rhythm disorders. Its goal is to restore normal sinus rhythm.
There are two types of it:
- Pharmacological (drug) cardioversion is the intravenous administration of antiarrhythmic drugs (Cordarone, Amiodarone, etc.), which is carried out under strict monitoring of the patient’s condition.
- Electrical cardioversion (atrial defibrillation) is a method that leads to coordinated contraction of the heart muscle. This occurs due to the impact of a strong electrical impulse on it. The voltage is 50-200 J. When performing the procedure, synchronization with the electrocardiogram is performed, which reduces the risk of developing ventricular arrhythmia.
Cardioversion is planned, performed in a hospital setting and has special pre-hospital training. There are cases of emergency cardioversion, for example, in case of atrial fibrillation, aggravated by angina pectoris or heart attack.
The procedure requires special equipment - a cardioverter.
Defibrillator device
Defibrillators are divided into two types:
- External.
- Implantable.
The external defibrillator consists of storage and electrode blocks. In the first, the accumulation and transformation of electric current is carried out, and the second block represents electrodes. Defibrillators can be designed with one or two electrodes.
Devices can be divided into two more types:
- Professional or manual.
- Semi-automated and automated.
Professional devices are multifunctional. They perform defibrillation, heart rate monitoring, printing and more. The doctor has at his disposal a screen on which he can track the results of his work and a pinter. Also, professional equipment allows you to independently set the discharge values.
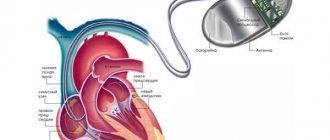
The implanted device is placed directly into the patient's heart muscle. The defibrillator independently reads a person's heart rhythm and, if necessary, sends a shock.
An automated defibrillator does this itself - it independently distinguishes between types of arrhythmia and sets the required shock value.
Reference! It takes about 20 seconds for an automatic defibrillator to detect the arrhythmia and the required shock.
In order for the semi-automatic device to give a shock, the doctor must press the “Start” button himself, while the automatic defibrillator does this itself.
Indications and contraindications
Emergency cardiac defibrillation is performed in the presence of the following symptoms:
- Pre-infarction condition of the patient.
- Heart failure.
- A sharp decrease in blood pressure (hypotension).
- Loss of consciousness by the victim.
- The patient's pulse cannot be felt.
- Severe ventricular arrhythmic disorders, which are characterized by frequent, asynchronous contractions of the heart muscle.
Severe ventricular disorders include:
- Ventricular fibrillation (flicker) is a pathology as a result of which the ventricles of the heart begin to contract at a huge frequency of 200-300 times per minute in a chaotic manner. The accelerated rhythm of contractions does not allow them to fill with blood, which causes a critical circulatory disorder that can lead to death. In this case, the patient may not have a pulse.
- Ventricular flutter is an arrhythmic disorder similar to fibrillation. Its distinctive feature is that the contractions occur in a rhythmic and orderly manner, rather than in a random order. In this case, fluttering can turn into fibrillation.
- Ventricular tachycardia is a disease in which the pulse is abnormal as a result of serious damage to the heart muscle. A violation can provoke an attack of rapid heartbeat, which will most likely develop into ventricular fibrillation. This can be fatal.
The main contraindication to this resuscitation procedure is complete cardiac arrest, since this fact makes the manipulation completely useless. If the heart suddenly stops, then it is urgent to perform indirect massage, artificial ventilation, and parenteral administration of drugs such as: Atropine, Epinephrine.
If the procedure is carried out as planned, then the contraindication will be that the patient took cardiac glycosides less than three days ago. With the accumulation of these substances, the risk of irreversible ventricular fibrillation increases significantly.
Diseases for which elective defibrillation (cardioversion) is contraindicated:
- permanent form of atrial fibrillation (more than 2 years);
- sinus tachycardia;
- arrhythmias arising due to dystrophic changes in the ventricles of the heart;
- the appearance of blood clots in the atria;
- polytopic atrial tachycardia.
Basic parameters and algorithms of AED
Many AEDs contain automatic and semi-automatic modes in their algorithm, the fundamental difference of which is that the automatic mode does not require operator intervention to deliver a shock; the semi-automatic mode of the defibrillator, in turn, provides notification of the need for defibrillation.
Compactness and light weight allow you to carry and conveniently place the defibrillator next to the patient. The AED takes into account tissue resistance, body weight, and height of the patient: the optimal power selection occurs automatically. Electrodes adhesive to the chest help free the rescuer's hands. The defibrillator itself sets the polarity of the electrodes.
Defibrillation using a biphasic (bipolar) pulse reduces the current strength compared to a monophasic (monopolar) pulse because the pulse passes through the heart muscle, then changes direction and passes through the myocardium again. A biphasic defibrillator, compared to a monophasic defibrillator, showed greater effectiveness in stopping life-threatening arrhythmias from the first shock: 94 versus 81%.
An important algorithm in the AED is to prohibit the delivery of a shock if the patient has a normal rhythm, which prevents inadequate shock delivery and the use of the device for other purposes.
An electrical discharge excites cardiomyocytes that are in a state of refractoriness during a life-threatening arrhythmia and are unable to cause full contractions of the heart muscle. The defibrillator discharge synchronizes cardiomyocytes, bringing them into a state of repolarization due to an electrical impulse similar to the impulse generated in the sinus node, but many times stronger.
If by the time of defibrillation the myocardium has not lost its energy reserves due to resuscitation measures, especially chest compressions, then in most cases sinus rhythm is restored, which promotes full contraction of the heart and adequate cardiac output.
The electrical impulse emanating from the defibrillator must exceed the defibrillation threshold in order to stop the arrhythmia. When a low-magnitude pulse is applied, fibrillation will not stop, and a high-power discharge can cause various types of arrhythmias: group extrasystoles, ventricular tachycardia, atrioventricular block, etc. - which will disrupt the functioning of the heart.
In this case, if a rare idioventricular rhythm or complete atrioventricular block occurs, implantation of a temporary endocardial lead and placement with a temporary artificial pacemaker may be required after defibrillation.
When using an AED, it is impossible to deliver a shock with insufficient or excessive power, since, after a quick analysis, the AED delivers the most effective and safe electrical impulse that helps restore cardiac activity. The quality of CPR performed can be determined based on the analysis of ECG signals, which are stored in the AED and can be assessed by specialists.
Features in children
In pediatric practice, the same algorithm of actions is used as for emergency care for adults.
When performing defibrillation on a child, it is important that the elements of the device cover the required area of the chest and do not come into contact with each other.
The age of the child plays a big role when choosing a defibrillator model. An automatic defibrillator should not be used for children under 8 years of age and weighing less than 25 kilograms, since these devices do not have the ability to regulate the voltage.
When carrying out defibrillation for infants weighing no more than 10 kilograms, special children's electrodes are used. For all other cases, the standard electrode size is used. For children aged 1 to 8 years, it is recommended to use a manual defibrillator.
In order to perform defibrillation correctly, it is necessary to know the exact weight of the child. For every kilogram of weight, it is allowed to give a shock with a force of 2 J; if there is no positive dynamics, the voltage is increased to 4 J.
When carrying out the procedure, small children need to ensure that the gel does not smear, because this may cause the electrodes to short-circuit and the effectiveness of defibrillation will decrease.
In children, the indications for the procedure will be the same as in adults - circulatory arrest (asystole) as a result of ventricular fibrillation or ventricular tachycardia in the absence of a pulse.
How to properly operate a defibrillator?
Before using these devices, you should carefully read the instructions supplied with them. The defibrillator should only be used when the person is as far as possible from conductive objects and on a flat surface.
When performing defibrillation, all safety regulations must be followed. During a critical situation, you must act calmly and quickly, without panicking. Before you begin to assist a fainting patient, you should make sure that he has a pulse and is breathing. Then you will have to call an ambulance, because without the help of professional doctors the chance of success in resuscitation is too low.
You can start defibrillation before the doctors arrive, so as not to waste precious time. To carry it out, you will need to remove the patient’s outer clothing and apply the device’s electrodes to the chest strictly according to the instructions. The person's skin should be dry. To reduce skin resistance, it is better to use electrically conductive paste. To prevent burns and reduce resistance, the electrodes must be pressed more tightly to the patient's body.
When performing a discharge, do not touch the metal electrode plates or the victim. It is for this reason that people nearby must move to a safe distance. There is no need to ventilate the lungs during defibrillation. The device discharges the device once, and a second pulse is performed with the same voltage or with an increase of several units.
Methodology
When carrying out resuscitation measures, ambulance teams use the method of electrical cardiac defibrillation. Diagnosis of circulatory arrest in a patient is made using a cardiogram, under the control of which the procedure is carried out.
Process on video:
It has the following sequence of actions:
- The patient is placed on a flat horizontal surface.
- Take off clothes and jewelry hanging on the chest.
- A special gel is applied to the electrodes, which promotes better current conduction. If it is not available, you can use gauze soaked in 7% sodium chloride solution.
- It is important to correctly position the electrodes on the chest: the first is installed on the left just above the apex of the heart, the second - under the right collarbone. If the patient has a pacemaker, the electrodes should be placed no closer than 8 centimeters from it.
- The electrodes should be pressed to the body with a force of 8-10 kg.
- Turn on the defibrillator and set the required power (the charge strength is calculated individually). There are defibrillators that detect this indicator automatically.
- While the electrodes are being charged, the patient can undergo indirect cardiac massage and artificial respiration.
- Before giving a shock to the patient’s body, it is necessary to make sure that at this moment no one from the medical personnel touches him or touches the surface where he is lying.
- After making sure it is safe, the doctor delivers a shock, then checks the pulse manually (on the carotid artery) or the patient is connected to an electrocardiography machine, where changes will be recorded.
- If there are no changes, then a second discharge of stronger power is applied. While charging the electrodes, perform cardiopulmonary resuscitation (indirect cardiac massage, CPR).
The procedure for providing assistance can be repeated up to four times, but if this does not give any therapeutic effect, then the patient’s death is declared.
Features of modern defibrillators
Today, defibrillators are often produced with an automatic operating mode. This allows them to be used even by non-professional health workers. Such models are widely used today on airplanes and trains; they are placed in first aid kits, which are then used in first aid stations of various locations.
It is worth noting that if assistance is provided with an automatic defibrillator during the first minutes from the onset of an attack, the effectiveness of its use reaches 98%.
The main differences between modern defibrillators:
- The discharge level is often selected automatically; for this, the device compares various indicators (gender and age of the patient, his height and weight, tissue resistance).
- The device selects the optimal polarization and placement of the electrode.
- If necessary, the user is notified by the device using prompts and signals.
- When cardiac activity normalizes, a button is automatically activated that blocks the discharge.
What types of defibrillators are there?
Before the advent of the first defibrillators, arrhythmias were treated exclusively with medications. Today, these various devices can be used by cardiologists and resuscitators, as well as ordinary people who do not have professional knowledge and skills.
In order to learn how to use the device, and in an emergency situation to be able to save someone’s life, just watch the video instructions, for example this one:
The widespread use of defibrillators is the reason for the emergence of several varieties of this medical equipment:
- Professional defibrillators are used in medicine, both in intensive care and hospital settings. They have the maximum number of possibilities. The electrodes with which the device is equipped are suitable for reusable use. All parameters are manually adjusted; to use the defibrillator, special knowledge and skills are required.
- Automatic defibrillators: have disposable electrodes, the device is relatively lightweight, so it can be transported. The device automatically detects rhythm disturbances and signals when an electrical shock should be administered. Modern defibrillators of this type are used by emergency services personnel, nurses, flight attendants, train conductors, and hotel staff.
- Combined defibrillators: can work both in stand-alone mode, and there is the possibility of manually setting the device. Thanks to this mechanism, they can be used both in hospitals and in crowded places.
- Implantable defibrillators: installed during surgery along with a pacemaker, or separately. They are designed to restore normal sinus rhythm and work on an open heart in contact with the myocardium. These devices are used for complex forms of heart rhythm disturbances.
Types of defibrillators
Devices that restore cardiac fibrillation come in different types:
- Automatic defibrillator - recognizes heart ailments, and then prompts the operator to deliver a shock. To perform defibrillation, you first need to turn on the device, stick electrodes on the patient’s chest and press the necessary button. Working with it does not require special skills, so the treatment procedure can be carried out not even by medical workers, but, for example, by sports team coaches, rescuers, flight attendants, teachers, and so on.
- An implantable defibrillator is a device that differs from other devices in its compact size. It is often used in conjunction with a pacemaker for patients with serious heart pathologies.
- A manually controlled professional defibrillator has the necessary set of programs. Such a device transmits an electrical discharge through electrodes in the form of irons. Before performing defibrillation, they are pressed more tightly to the patient's body.
Such medical devices also differ in the parameters of the pulses generated. Based on these characteristics, defibrillators can be biphasic or monophasic. Moreover, the latter are now impossible to find on the primary market, since bipolar devices are much more effective, so they are gradually replacing monopolar ones.
How often can you be saved?
The effectiveness of defibrillation and the chances of survival depend on the following factors:
- The amount of time that has passed since the onset of fibrillation: the procedure is highly effective only in the first three minutes, then its effectiveness decreases minutely by 10-15% and after just 10 minutes there is no longer any chance of saving the person.
- The correct technique for performing all accompanying actions during resuscitation - chest compressions, mechanical ventilation, injections.
- The correct technology for performing defibrillation itself.
- The quality of the equipment used.
Saving the life of a victim with a combination of all factors is about 85% of cases.
In real conditions, it is possible to save only 5-15% of people whose attack began in public places or at home, and 50-70% of patients who were already in hospital treatment.
Implantation of a defibrillator-cardioverter is considered the most effective; thanks to it, 99% of patients survive, since the attack is relieved instantly.
Implantation of a cardioverter defibrillator.
Implantable cardioverter defibrillator (ICD) is an operation in which an electronic device (implantable cardioverter defibrillator, or ICD) is placed into the human body to monitor and stop life-threatening arrhythmias.
ICD implantation
It is clear that such a device is implanted only in people at risk of life-threatening arrhythmias. These are, as a rule, people with severe heart failure, post-infarction patients, patients who experienced clinical death from arrhythmia and were successfully resuscitated, that is, survivors. The installation of an ICD into the human body takes place in an operating room equipped with fluoroscopic equipment, so that, under X-ray control, the surgeon installs the ICD and electrodes in the optimal position in the heart.
Complications and consequences
The powerful effect on the heart during defibrillation has its consequences in the form of the following complications:
- Extrasystole (extraordinary contractions of the heart muscle) is observed within several hours after defibrillation on electrocardiography. Mild forms of the disorder disappear after a couple of hours, severe forms - after a few days.
- Soft tissue injuries: burns, hematomas and bruises with bruising.
- Pulmonary embolism is a fatal condition in which the pulmonary artery or its branches are blocked by a piece of blood clot.
- Pulmonary edema.
- Breathing problems due to improper pain relief.
- Reduced blood pressure.
Early cardiac pacing saves the lives of many patients, eliminating even the most severe cardiac disorders. However, the prognosis for these patients will be poor.
Ventricular atrial fibrillation is not an independent and sole disease, but is a consequence of more complex and long-term pathologies: acute heart failure, myocardial infarction, combined heart defects.
As before, the patient continues to have a high risk of a second attack, from which a person who has experienced clinical death will no longer be able to get out again.
Author of the article: Yulia Dmitrieva (Sych) - In 2014, she graduated with honors from Saratov State Medical University named after V. I. Razumovsky. Currently working as a cardiologist at the 8th City Clinical Hospital in the 1st clinic.
Performing CPR and defibrillation
Defibrillation in case of sudden cardiac arrest must be timely, since its implementation some time after circulatory arrest leads to a decrease in the survival rate of patients.
One of the most important components in saving a patient’s life is proper CPR. Thus, in an experimental study involving animals, an increase in survival was shown in the case of CPR for VF.
Another study, in which emergency physicians performed CPR for 3 minutes before defibrillation during sudden cardiac arrest, demonstrated a higher success rate with CPR compared with no CPR. Two ambulance protocols were used. The first included CPR for 3 minutes before defibrillation, the second included defibrillation without previous CPR, while the time interval was no more than 5 minutes from the onset of clinical death.
The results of comparison and analysis of the two protocols did not differ significantly. When the time interval was more than 5 minutes from the development of clinical death, the analysis of the study results was in favor of the first protocol, the use of which led to increased survival in patients with sudden circulatory arrest.
According to the latest Congress on CPR and Emergency Care, in the event of sudden cardiac arrest, CPR should be started immediately, including chest compressions, mechanical ventilation and early defibrillation.
Defibrillation is carried out in the event of a sudden arrest of blood circulation when there are eyewitnesses at the scene and an AED is placed near it, which can be used in this situation. 5 minutes after loss of consciousness and cardiac arrest, it is necessary to perform CPR for 2 minutes, and then defibrillate.
In SCD, a single electrical impulse is given using a defibrillator, then, without wasting time in determining the heart rhythm, CPR is performed for 2 minutes, after which it is recommended to evaluate the heart rhythm. You should not spend a lot of time determining the heart rhythm, since stopping CPR at this stage leads to a decrease in perfusion pressure in the coronary arteries, as well as a decrease in patient survival.
The recommended electrical impulse value for defibrillation when using a biphasic defibrillator is 150-200 J. This is the shock value used in modern AEDs.
The shape of the discharge plays an important role in choosing the magnitude of the electrical pulse. So, if a rectangular form of a biphasic electrical pulse is used, then the value of the first discharge is 120 J. Subsequent discharges should be of a similar or greater magnitude.
This knowledge is necessary in cases where the value of the defibrillation discharge is set by the rescuer. In other cases, the AED independently recommends a shock of the required magnitude, taking into account the parameters of each patient.
If the rescuer decides to set the shock value independently, and the recommended initial shock value is not indicated on the AED and the rescuer does not know what form of biphasic shock is used in the AED, then the recommended value of the electrical impulse in such cases is 200 J.
When restoring heart rhythm, it is recommended to perform indirect cardiac massage for several minutes. This allows you to improve cerebral and coronary circulation, thereby strengthening the effectiveness of resuscitation measures.
Each of us can become a witness to SCD. In such a situation, the lives of our relatives, friends or people who need our help will depend on our preparedness and equipment.
If there is an AED near the rescuer, first of all it is necessary to free the chest from clothing, turn on the device, and apply the electrodes. An automatic external defibrillator will analyze your heart rhythm and, if indicated, make a recommendation to defibrillate by pressing a button. The device will re-analyze the heart rhythm and automatically issue an electrical impulse of the required magnitude.
If there is no positive effect, the device will advise you to proceed with CPR. At the same time, the correctness of the defibrillation algorithm is monitored: if the compression is insufficient, the device notifies about this and suggests either increasing the depth or increasing the frequency of compression.
The AED also makes recommendations on the need for artificial ventilation. The standard is two breaths for thirty compressions in one cycle. Five cycles are carried out for 2 minutes, then the heart rate is assessed. If the recovery of heart rate takes several minutes, it is recommended to perform indirect cardiac massage. If restoration of cardiac activity does not occur, a second shock is performed with the same or greater magnitude of the electrical impulse and CPR is continued.
One study of schoolchildren aged 11-12 years showed that children, just like adults, can perform CPR using an AED. The ability to achieve adequate depth of chest compression depends on the age and weight of the child. All other basic CPR activities, including AED operation, can be mastered by children over 11 years of age.
A modern AED helps the rescuer correctly perform all stages of CPR. In a situation where clear actions are required, even a trained rescuer may not immediately find his bearings. An automatic external defibrillator acts as a coordinator for a non-professional rescuer, and reminds a qualified specialist of the correct phasing of resuscitation measures.
Indications
- ventricular (ventricular) fibrillation;
- ventricular (ventricular) tachycardia without pulse.
Defibrillation is not indicated if the heart has stopped completely (with asystole and pulseless electrical activity), or when the patient is conscious or has a pulse.
Cardioverter defibrillator - prohibitions after surgery.
After implantation of a cardioverter-defibrillator, the patient must lie down for 6 hours after surgery. For 3 months after the operation, the patient is asked to maintain a certain motor regimen: raise the left arm (from the implantation side) above shoulder level, avoid sudden and sweeping movements, falls, sleep on the back or left side. Patients with a cardioverter-defibrillator should not work with high-voltage power lines or arc welding, and should not pass through metal detectors. Otherwise, people with ICD can lead normal lives.
Types and essence of the procedure
Defibrillation of the heart is the application of an electrical discharge through its chambers in order to restore the normal rhythm of the organ.
To perform the manipulations, a special device is used - a defibrillator. Therapy of this kind can be carried out plannedly or urgently, depending on the situation. Performing electrical pulse treatment is the responsibility of a cardiologist, ambulance doctor or resuscitator. These specialists must be skilled in the technique of performing the procedure. What is a defibrillator? The device for supplying electrical impulses can be portable or stationary. It is equipped with three blocks: in one of them electricity is accumulated and converted, the other is one or two electrodes, the third element is a defibrillator-monitor. There are monophasic and biphasic electrical stimulators. The first one starts current in one direction. The operating principle of the second device: it uses alternating current electricity moving from electrode to electrode and back.
There are automatic devices that, unlike manual ones, can detect various rhythm disturbances. They also select the required discharge power for each case. Sometimes care has to be provided far from the hospital walls. Ease of operation makes the device accessible even for use by people who have not been licensed, that is, without special medical training.
Many people have a natural question: is it possible to start the heart with a defibrillator? Electrical treatment is allowed only if at least some semblance of contractile activity is maintained. Thus, it makes no sense to use a defibrillator during cardiac arrest.
In case of asystole (lack of contractions), it is necessary to begin artificial respiration, alternating with chest compressions. When the most important organ shows signs of life, electrical pulse therapy can be performed. It exists in two varieties: defibrillation itself as an emergency measure, and cardioversion.
Why do you need an electric defibrillator in emergency situations? It is used to eliminate ventricular arrhythmia (the most severe disorder). This method of cardiac stimulation always requires urgent implementation, because in this case there is a real threat to life. The person is unconscious when the current is applied.
What is electrical cardiac defibrillation, called cardioversion? The term also implies the application of current discharges, but they must be synchronized with the ventricular complex (QRS). To do this, a parallel ECG is required during the procedure. The use of this type of treatment is relevant in the presence of atrial rhythm disturbance. Both planned and emergency procedures are possible. The first option is carried out with the patient’s informed consent and under anesthesia.
Electrical impulses are applied by two defibrillator electrodes, located in a special way on the patient’s chest. In this case, special treatment is carried out on the skin and the devices themselves.
There is another type of return to normal contractile activity of the heart. A device is implanted into the chest, which sets the desired rhythm. If necessary, a defibrillator-cardioverter recognizes and stops an attack of life-threatening atrial fibrillation.
Further tactics of assisting the patient after an attempt to restore rhythm
If defibrillation is successful, the patient requires observation and care. Often, applying an electrical discharge through the conduction system can cause the development of arrhythmia. Neurological disorders associated with temporary cerebral hypoxia are also possible.
Main goals of further actions:
- diagnosis and treatment of the causes of cardiac arrest;
- minimizing negative consequences on the nervous system.
To do this, the following conditions must be met:
- conducting an ECG in 12 leads;
- conducting encephalography in cases of impaired consciousness (coma) and in patients with epilepsy;
- emergency reperfusion (restoration of blood flow) if the cause of cardiac arrest is myocardial infarction;
- maintaining stable blood pressure and blood glucose levels;
- oxygen supply;
- control of body temperature (within 35-36 ˚C);
- consultation with a neurologist.
Resuscitation actions are stopped:
- if resuscitation measures carried out within 30 minutes are ineffective;
- when declaring death based on irreversible cessation of brain function.
Suturing the cardioverter-defibrillator bed.
The last stage of the operation is suturing. The tissues are always sutured in layers. First, the muscle is sutured with separate interrupted sutures using a non-absorbable thread. Then the subcutaneous fat is sutured with the same thread. Finally the skin is sutured. Most often, absorbable material is used on the skin and an intradermal cosmetic suture is applied. Absorbable suture material does not need to be removed; it will dissolve on its own in 1-1.5 months. Sometimes non-absorbable interrupted sutures are also placed in the skin. Such sutures are removed 10-14 days after surgery.
When is defibrillation performed?
Indications for the use of electrical emergency defibrillation – severe ventricular arrhythmias:
- Fibrillation (random accelerated rhythm).
- Fluttering (the rhythm is accelerated, but orderly).
- Tachycardia that is not treated conservatively.
In this case, the condition can be complicated by acute heart failure and severe hypotension.
- The heart beats frequently and chaotically. You need to check the heartbeat in the sternum area; the pulse most likely will not be palpable.
- The person is unconscious. Clinical death is registered.
The purpose of the procedure is to save a person’s life, restore adequate activity of the heart, and prevent it from completely stopping. The measures are related to resuscitation, the manipulation must be carried out as quickly as possible. With every minute of delay, the risk of biological death increases.
Indications for ICD implantation – who needs surgery?
The device in question is implanted in the following pathological conditions:
- The patient has a history of sudden cardiac arrest.
- Insufficient contraction of the heart muscle - ventricular fibrillation.
- Severe ventricular tachyarrhythmias. The introduction of an ICD will prevent sudden cardiac arrest.
- Heart rate is significantly lower than normal.
- A history of serious arrhythmias (1 or more).
- Myocardial infarction, in which the electrical conductivity of the heart was disrupted. This phenomenon may cause dangerous arrhythmias to appear in the future.
- Heart failure.
Types and degrees of heart block - symptoms and consequences of heart block