What is heart bypass surgery?
Coronary artery bypass surgery is an open-heart surgery in which a bypass path is created for cardiac blood flow, bypassing the affected arteries.
CABG surgery is performed using fragments of other vessels of the patient, which are most often taken from the lower extremities. Surgery is performed only in specialized clinics by highly qualified cardiac surgeons, with whom a transfusiologist works together to provide artificial blood circulation. It should be noted that the principle of this complex operation was developed by the Soviet doctor Vladimir Demikhov in the sixties of the last century.
What is cardiac bypass surgery (coronary artery bypass grafting), how long do they live after surgery?
From the article you will learn the features of heart bypass surgery, indications and contraindications, possible complications, rehabilitation, life prognosis.
From the article you will learn the features of heart bypass surgery, indications and contraindications, possible complications, rehabilitation, life prognosis.
Indications for bypass surgery
The indication for bypass surgery is narrowing of the coronary vessels due to atherosclerotic deposits or spasm, and the resulting disturbance of blood circulation in the myocardium.
Bypass surgery is done to reduce myocardial ischemia, eliminate attacks of angina, improve myocardial trophism - the supply of nutrients and oxygen saturation.
Shunt surgery is prescribed if:
- obstruction of the patency of the left trunk of the coronary artery;
- multiple narrowing of the coronary vessels in remote (distal) sections;
- disturbance of coronary blood flow in combination with a left ventricular aneurysm or disruption of the heart valves;
- failure of angioplasty, stenting.
Extensive lesions in the heart develop after a myocardial infarction, which makes coronary bypass surgery the best way to help solve the problem of restoring blood circulation after an attack, and it is advisable to do such an intervention as quickly as possible.
The patient is hospitalized 5-7 days before bypass surgery. During these days, he undergoes a full examination, masters the techniques of deep breathing and coughing, which are required during the recovery period.
How much does coronary heart bypass surgery cost in Moscow:
Complications
Complications after bypass surgery can occur during surgery and after discharge. As stated above, the risk of adverse effects is assessed before intervention and depends on the background condition of the body. The most common problems include:
- acute renal failure;
- thrombosis;
- cardiac arrest;
- rhythm disturbances;
- myocardial infarction;
- infection, including sepsis;
- pneumonia;
- bleeding;
- pericarditis and cardiac tamponade;
- pulmonary edema;
- cardiogenic shock;
- neurosis.
A long-term complication is stenosis of the shunts due to non-compliance with the doctor’s recommendations. In this case, the patency of the vessels becomes more difficult again, and a typical clinical picture of angina occurs. This situation requires repeated coronary artery bypass grafting.
- The stationary period is aimed at expanding the motor regime. The patient is allowed to sit down, then stand, walk around the ward, etc., increasing the load on the heart every day under the strict supervision of the staff.
- Long-term observation. After discharge from the cardiology center, recovery after cardiac bypass surgery continues at home. The patient is usually on sick leave to avoid overload and colds. You can return to work no earlier than six weeks after discharge (the period is determined individually). For a driver or builder, it is usually extended to another three months. The patient should visit the local doctor and cardiologist 3, 6 and 12 months after the intervention. During each visit, he undergoes an ECG, determines the biochemical spectrum of lipids, a general blood test, and, if necessary, a chest x-ray. The main principle of the rehabilitation process at this stage is lifestyle modification. The concept implies adequate sleep (at least 7 hours), frequent split meals with the obligatory inclusion of polyunsaturated fatty acids in the diet, quitting smoking and alcohol abuse, sufficient physical activity, maintaining normal body weight (waist circumference in women. How long do they live after surgery?
Types of heart bypass surgery
Blood can be shunted either from the general circulation to the pulmonary circulation (ie, a “left-to-right shunt”), or between the pulmonary circulation and the systemic circulation (ie, a “right-to-left shunt”). In rare cases, blood does not return through the shunt to the same chamber of the heart from which it came out without passing through the capillary bed. But this option is possible and it is called a “circular shunt”.
- Shunting from left to right
In a left-to-right shunt, oxygenated blood flows directly from the systemic circulation into the pulmonary circulation, resulting in decreased tissue oxygenation through decreased cardiac output. Reasons for performing this type of bypass:
Cardiac:
- Ventricular septal defect (VSD).
- Atrial septal defect (ASD).
- Atrioventricular septal defect (AVSD).
- Patent ductus arteriosus (PDA).
Vascular –
complete or partial abnormal return of venous blood.
- Shunting from right to left
In a right-to-left shunt, deoxygenated blood flows directly from the pulmonary circulation into the systemic circulation. As a result, oxygen saturation of tissues decreases due to a decrease in oxygen content in systemic arterial blood. Reasons for performing this type of AL:
Cardiac:
- Tetralogy of Fallot.
- Pulmonary atresia.
- Double exit from the right ventricle.
- Transposition of large arteries.
- Patent ductus arteriosus.
- Eisenmenger syndrome
Vascular:
- Pulmonary arteriovenous malformations.
- Hepatopulmonary syndrome.
- Parenchymal intrapulmonary shunts.
- Atelectasis.
- Pneumonia.
- Bronchoalveolar cancer.
- Circular shunt
Most cardiovascular shunts, performed from left to right or right to left, result in the shunted blood returning to the same chamber after passing through the capillary bed (pulmonary or peripheral). If this does not occur, then the term “circumferential shunt” may be used. Such shunts are usually present in complex congenital heart defects. [2]
- Bleeding
- Infectious disease
- Abnormal heart rhythms (arrhythmias)
- Lung and kidney problems
- Short-term memory problems – mostly temporary
Possible complications after vascular bypass surgery
Complications during cardiac bypass surgery are divided into specific and nonspecific.
Nonspecific risks are those associated with any operation.
Specific complications include:
- heart attack;
- inflammatory process of the outer layer of the pericardial sac;
- disruptions in myocardial function and tissue starvation as a result of insufficient blood supply;
- arrhythmias of various forms;
- infectious lesions of the pleura and trauma;
- stroke.
After discharge, the patient should perform therapeutic physical exercises to strengthen the cardiovascular system.
Preparation
Survey is the basis. Correct measures reduce the risk of dangerous complications after surgery.
What procedures are prescribed:
- ECHO. Ultrasound technique, the task is to assess the organic state of the heart and myocardium.
- ECG. Based on the results, a graph is drawn up, on the basis of which conclusions can be drawn about functional disorders of the muscular organ. Prescribed in conjunction with echocardiography.
- Coronary angiography. Mandatory technique. At its core, it is an X-ray with contrast enhancement. Allows you to examine the vessels of the heart in detail, examine areas of narrowing and other anomalies. Used as a matter of priority.
- FVD. Function of external respiration. It is carried out to assess the quality of lung function. Including under increased load. This is important to understand the state of the respiratory system.
- General blood test, biochemistry. To exclude inflammatory processes. Urine examination. For the same purpose.
- Special tests for infectious pathogens. Wasserman reaction, HIV tests and others.
- Consultation with an anesthesiologist. Since there will be a long-term anesthesia, you need to answer the specialist’s questions. Preferably in detail, without leaving out anything. Safety depends on this.
The day before surgery, the patient refuses to eat. Also, a few days before the start of treatment or even more, medications are discontinued. Anticoagulants, other dangerous ones. But strictly at the discretion of the specialist. This is necessary to minimize the risks of bleeding and arrhythmias.
What procedures are prescribed:
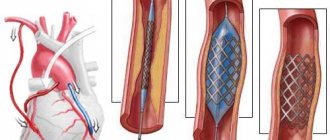
Coronary stenting of heart vessels
It is considered a gentle, minimally invasive, intravascular operation on the vessels of the heart, which consists of widening a narrowed artery by straightening the inserted stent. Stenting is usually carried out immediately after coronary angiography , which makes it possible to determine the extent of damage to the coronary artery and select the stent required in diameter and length.
- coagulogram;
- biochemical and general blood test;
- Ultrasound of the abdominal organs;
- lipid spectrum;
- chest x-ray;
- Ultrasound scanning of the lower extremities;
- ECG;
- EchoCG;
- Analysis of urine.
What to do before bypass surgery
It is important to understand that bypass surgery is a large abdominal operation where not everything depends on the capabilities of the surgeon. There are factors that can have an adverse effect on post-operative recovery.
-continued smoking. Studies have shown that patients who continue to smoke in the immediate preoperative period are significantly more likely to develop pulmonary complications, have poorer wound healing, and spend more time in the intensive care unit.
- obesity. Obesity is a risk factor for postoperative complications. If there is a temporary opportunity to reduce by 5-10 kg, you should take advantage of it, this will reduce the risks.
- insufficient compensation for diabetes mellitus. With long-term diabetes, one of the complications is slow or incomplete healing of the postoperative wound. Optimal treatment of diabetes mellitus over several weeks is desirable.
Return to work after coronary artery bypass surgery is strictly individual and depends on the dynamics of rehabilitation and the nature of the work. The decision to return to work is made by a special commission. Persons with sedentary and/or sedentary work can work as early as 1.5 months after surgery. In the case of heavy physical work, it may be necessary to change working conditions to easier ones. In some cases, the patient cannot return to work and is given a disability group. In all cases it is individual.
Coronary artery bypass grafting on a beating heart
Coronary artery bypass surgery without artificial circulation allows you to avoid complications caused by the use of a medical device. Surgery on a beating heart requires deep knowledge and skill from the surgeon. Coronary artery bypass surgery is performed under physiological conditions for the heart, which reduces the risk of postoperative complications and speeds up the patient’s recovery and discharge from the hospital.
Rehabilitation after heart bypass surgery contains a set of exercises and activities:
Varieties
Depending on which vessel is used for the bypass, there are two types of heart bypass:
- aortocoronary – CABG;
- mammarocoronary – MCS.
CABG, in turn, is divided into:
- autovenous, when the great saphenous vein of the leg is used;
- autoarterial - when using the radial artery (if the patient suffers from varicose veins).
For MCS, the internal mammary artery is used.
In addition, there is a division of bypass into:
- standard – using an artificial blood supply device (heart stopped);
- without the use of artificial blood supply to the heart (the heart does not stop), which requires the highest qualifications of the surgeon;
- hybrid, when different types of additional procedures are combined.
Story
The first coronary artery bypass surgery was performed in the United States on May 2, 1960, at the Johns College of Medicine. Albert Einstein. The operation was performed by a team led by Robert Goetz and thoracic surgeon Michael Rochman. To complete the SS, the technique of holding the vessels together using circular ligatures was used.
The internal mammary artery was used as a donor vessel and was anastomosed to the right coronary artery. The actual anastomosis with the Rosenbach ring was performed in fifteen seconds and did not require cardiopulmonary bypass.
Soviet cardiologist Vasily Kolesov performed the first successful artery-to-coronary anastomosis in 1964. He used a standard suturing technique and over the next five years, the doctor performed 33 stitched and mechanically fastened anastomoses in Leningrad, USSR.
Rene Favaloro, an Argentine surgeon, introduced a physiological approach to the surgical treatment of coronary artery disease at the Cleveland Clinic in May 1967. His new technique relied on saphenous vein autograft to replace a stenotic segment of the right coronary artery. He later successfully used the saphenous vein as a bypass, which became the typical bypass technique used today.
Soon, Dudley Johnson expanded the bypass, for which he included the left coronary artery in the system.
In 1968, doctors Charles Bailey, Teruo Hirose and George Green used the internal mammary artery instead of the saphenous vein for cardiac bypass surgery. [1]
Indications for surgery
Bypass surgery of the affected heart vessels is performed for arterial stenosis causing ischemia. The most common cause is atherosclerosis, when the lumen of the arteries is blocked by atherosclerotic plaques, or thrombosis. These pathologies are the main indications for surgical intervention. Additional examination is carried out when:
- retrosternal pain radiating to the left arm, shoulder, lower jaw, neck;
- hypertension;
- tachycardia; constant nausea, heartburn.
What is the essence of coronary artery bypass grafting?
With coronary heart disease, the main culprit of which is atherosclerosis of the coronary vessels, blockage of one or more arteries of the heart may occur. This process is accompanied by severe myocardial ischemia, the patient more often experiences angina attacks and myocardial infarction may develop. To restore blood circulation in the heart muscle, surgeons create bypass paths by performing an anastomosis from a vein excised from under the skin of the thigh, or an artery of the patient taken from the forearm or the inner surface of the chest. One end of this bypass vessel is attached to the aorta, and the other is sutured into the coronary artery below the site of atherosclerotic blockage or narrowing. If the internal mammary artery, which is already connected to the aorta, is used for the bypass, then one of its ends is sutured to the coronary vessel. This cardiac surgery is called coronary artery bypass grafting.
Previously, femoral veins were used to create an anastomosis, but now surgeons more often use arterial vessels, because they are more durable. According to statistics, a shunt from a venous femoral vessel is not subject to re-occlusion within 10 years in 65% of patients, and from an arterial vessel of the internal mammary artery it functions properly in 98% of those operated on. When using the radial artery, the anastomosis works flawlessly for 5 years in 83% of patients.
The main goal of coronary artery bypass grafting is aimed at improving blood flow in the area of myocardial ischemia. After the operation, the area of the heart muscle experiencing insufficient blood supply begins to receive an adequate amount of blood, angina attacks become less frequent or are eliminated, and the risk of developing a heart attack is significantly reduced. As a result, coronary artery bypass grafting can increase the patient's life expectancy and reduce the risk of sudden coronary death.
The main indications for coronary artery bypass surgery may be the following conditions:
- narrowing of the coronary arteries by more than 70%;
- narrowing of the left coronary artery by more than 50%;
- ineffective percutaneous angioplasty.
Contraindications
CABG surgery is not performed in the following cases:
- with renal failure;
- uncompensated diabetes mellitus;
- chronic nonspecific lung lesions;
- malignant neoplasms;
- post-stroke hypertension.
There are also relative contraindications for bypass surgery:
- heart failure;
- obesity;
- scarring of the heart, minimizing cardiac blood output below 30%;
- Menkenberg's arteriosclerosis - damage to all coronary arteries;
- elderly age.
AMI is considered as a contraindication at the discretion of the physician.
Coronary artery bypass grafting: indications, implementation, rehabilitation
Author: Averina Olesya Valerievna, candidate of medical sciences, pathologist, teacher of the department of pathology. anatomy and pathological physiology, for Operation.Info ©
Coronary arteries are vessels that extend from the aorta to the heart and supply the heart muscle. In case of plaque deposition on their inner wall and clinically significant blocking of their lumen, blood flow in the myocardium can be restored using stenting or coronary artery bypass grafting (CABG). In the latter case, a shunt (bypass) is inserted into the coronary arteries during the operation, bypassing the area of artery blockage, due to which the impaired blood flow is restored and the heart muscle receives a sufficient volume of blood. As a rule, the internal mammary or radial arteries, as well as the saphenous vein of the lower extremity, are used as a shunt between the coronary artery and the aorta. The internal mammary artery is considered the most physiological autoshunt, and its wear rate is extremely low, and its functioning as a bypass lasts for decades.
Carrying out such an operation has the following positive aspects : increasing life expectancy in patients with myocardial ischemia, reducing the risk of myocardial infarction, improving quality of life, increasing exercise tolerance, reducing the need to use nitroglycerin, which is often very poorly tolerated by patients. The lion's share of patients respond more than well to coronary bypass surgery, since they are practically not bothered by chest pain, even with significant stress; there is no need for the constant presence of nitroglycerin in the pocket; fears of heart attack and death disappear, as well as other psychological nuances characteristic of people with angina pectoris.
Author: Averina Olesya Valerievna, candidate of medical sciences, pathologist, teacher of the department of pathology. anatomy and pathological physiology, for Operation.Info ©
Preparing for the intervention
The basis of preparation for CABG surgery is coronary angiography, a procedure that thoroughly examines the relief of the coronary endothelium. To carry it out and subsequent detailed examination, the patient is hospitalized in a hospital. To perform coronary angiography, special catheters are inserted into the left and right coronary arteries, through which X-ray contrast is applied. X-rays then scan the endothelium. The procedure allows you to accurately determine the location and degree of narrowing of the vessel, while the patient receives a high dose of radiation. In addition, the manipulation cannot be performed if there is an allergy to iodine (x-ray contrast).
Therefore, in addition to coronary angiography, CT coronary angiography is used. It is more accurate, more expensive, but eliminates radiation exposure. True, contrast is still necessary, and a person weighing more than 120 kg cannot fit into the device.
If the examination reveals narrowing of the arteries by more than 75%, CABG is prescribed to minimize the risk of AMI or its recurrence. In addition to coronary angiography, the following are required: CBC, OAM, general biochemistry, coagulogram, lipidogram, ECG, EchoCG, ultrasound of the abdominal organs.
If the patient takes anticoagulants, their use is agreed with the doctor: usually a break is taken for two weeks before surgery. Other groups of pharmacological agents also require consultation with a doctor.
The day before coronary artery bypass surgery, the patient is examined by an anesthesiologist, correlating anesthesia with the height, weight, age of the person being operated on, and individual intolerance to drugs. On the eve of the intervention, the patient is sedated (taken sedatives). Necessarily:
- do not eat after 18:00;
- do not drink after midnight;
- prescribed medications are taken immediately after dinner;
- in the evening - shower.
Preparing for heart bypass surgery
About two weeks before surgery you will need:
- Consult with your doctor about taking prescribed medications—some may need to be delayed for a while
- It is advisable to prepare your home for your return after surgery. You can find someone to help you get from the hospital, and then for the first time you can participate in the recovery period and solve various everyday issues: shopping, cooking, cleaning, etc.
- Some important tests may be done - including an ECG, chest x-ray, blood tests, nasal swab and carotid Doppler (which is an ultrasound scan of the blood vessels in the neck that supply the brain).
On the day before the operation, the following necessary manipulations are performed:
- Colon cleansing - with a laxative or enema.
- A small bag of essentials, such as toiletries and glasses, is packed and will be taken to the intensive care ward, where patients are brought after surgery.
- The consumption of food and drink is limited - from approximately midnight until the planned operation.
On the day of surgery:
- It is important to remember not to eat or drink anything from midnight until your surgery.
- If necessary, the nurse will remove any hair from the chest, arms, legs, and groin to reduce the risk of infection.
- Shower with antibacterial soap.
- Hospital gowns are put on and any makeup, nail polish, jewelry, or dentures are removed if necessary.
Progress of the operation
To perform a heart bypass, the doctor needs to cut the sternum, which then heals for a long time, which determines the length of the rehabilitation period. Depending on the type of CABG, a heart-lung machine is used or not. The heart is not stopped unless additional manipulations are required: removal of an aneurysm, replacement of valves. Bypass surgery on a beating heart has the following advantages: no complications from the immune system or blood; intervention time is shorter; rehabilitation is faster.
The essence of the operation is to create a workaround. To do this: the surgeon opens access to the heart, takes a vessel for a shunt, if the heart stops, perform cardioplegia and turn on the artificial blood flow equipment. If the heart is beating, special devices are applied to the intervention area. The bypass itself involves stitching together blood vessels: one end of the bypass is connected to the aorta, the other to the coronary artery, which is located below the stenosis. After this, the heart is started again and the equipment is turned off. The sternum is secured with metal staples, and the skin on the chest is secured with regular sutures. The bypass lasts about four hours.
Essence and types of operation
To understand what coronary artery bypass surgery is, you need to understand the anatomy.
The heart, its muscle layer or myocardium requires a huge amount of resources. This is understandable, considering the load placed on the organ. Nutrition and cellular respiration are provided through two large branches extending from the aorta. These are called coronary arteries.
In turn, the right and left trunks are divided into even smaller structures, and these, in turn, into an additional network. This is how trophism of the whole heart occurs.
With some diseases, for example, atherosclerosis, the vessels can no longer do their job and transport blood to the right place. In the described case, the reason is that cholesterol plaques are deposited on the walls of the arteries. These are mechanical obstacles.
The greater the formation and layering of fats, the less nutrients and oxygen the organ will receive per unit of time.
The end result is coronary heart disease. Angina is also possible. The processes are different, but the essence is approximately the same: insufficient blood flow, impaired nutrition and breathing, the gradual death of the functional tissues of the muscle layer itself, which has contractility and pumps blood.
There are other possible causes of ischemia. For example, congenital malformations or blood clots. Provided that mechanical obstacles cannot be eliminated by other methods (stenting, ballooning, that is, expanding the area), they resort to heart bypass surgery.
The essence can be described in several points:
- Decide which path can be the main one to bypass. It is necessary to connect the coronary artery and a healthy vessel.
- Select a vein or other structure that, in terms of size, caliber and properties, could become a shunt.
- Find an area that is mechanically blocked or otherwise altered.
- Create a bypass path from the donor vessel to a place where blood no longer flows due to a mechanical obstruction. There are only two key options for which area can become a source (see below).
Thus, doctors create an artificial collateral. A bypass for normal blood flow.
There are 3 types of cardiac bypass surgery. Classification is carried out according to the vessel that becomes the donor. This quite strongly affects both the effectiveness in different cases and the technique of the operation itself.
There are three key approaches in total:
- Coronary artery bypass grafting (CABG). Classic technique. In this case, blood flow to the myocardium comes directly from the aorta. To create such a bypass, you need a fairly large fragment of the vessel. For example, a section of a leg vein.
- Mammarocoronary bypass surgery (MCBG). It is used less often. Basically, they resort to this method if the previous one turned out to be ineffective. Also, such an operation is possible when there are contraindications: thrombosis, vascular abnormalities.
The essence of the procedure is to connect the internal mammary arteries and the myocardium itself to provide a bypass. If both coronary structures are affected at once, a double bypass can be created.
- For small amounts of heart damage, doctors resort to microinvasive bypass surgery. This is not the best choice if there are atherosclerotic changes.
The operation can also be classified on another basis - the condition of the heart at the time of the procedure. Accordingly, there are two more types:
- Intervention on the beating heart. It is considered a much more difficult method of therapy, since during the procedure the organ beats and contracts. However, the risks of postoperative complications are reduced, and the rehabilitation period becomes much shorter.
- Intervention on a non-functioning heart. In this case, the patient must be connected to a heart-lung machine. In general, cardiac arrest is not normal and does not bode well for the patient.
After the procedure, the likelihood of complications is higher, including secondary ischemia and sudden cardiac arrest. Pulmonary edema and acute severe inflammatory processes that destroy the myocardium are also possible.
Thrombosis, including distant ones, localized in the vessels of the brain - another unpleasant surprise. There are many options and they are all dangerous.
Therefore, the patient remains in the hospital for a long time, and then under the supervision of a cardiologist.
Attention:
The recovery period is 1.5-2 times longer.
Coronary artery bypass grafting (CABG) is considered the gold standard of surgical treatment. To retreat from it or not, by how much, in which direction - depends on the case. The decision remains with the cardiac surgeon.
Complications
Often after surgery, the patient experiences a feeling of pain, heat, and discomfort in the chest. This is not a reason to panic; you need to inform your doctor about this, who will prescribe relief medications. The most common complications after cardiac bypass surgery are: pulmonary congestion, anemia, pericarditis and other inflammatory processes, phlebitis of veins adjacent to the shunt, immune disorders (during cardiac arrest), arrhythmias.
To prevent congestion in the lungs, it is recommended to inflate balloons up to 20 times a day. Anemia can be controlled with a special diet and, if necessary, with blood transfusions. Treatment of other complications is individual for each patient.
Performing coronary bypass surgery
Coronary artery bypass surgery is performed in a cardiac surgery hospital. The procedure algorithm has been worked out and is well known:
- The patient is given anesthesia.
- Next, you need to take a section of an undamaged vessel, which will be the necessary bypass (shunt). The thoracic, radial arteries or leg vein are suitable for these purposes. The doctor decides the issue before the event starts.
- The next step is opening the chest, mobilizing tissues and the heart. The shunt itself is created. If there are several areas of narrowing or other damage, then there is more than one artificial collateral. As a rule, the aorta or thoracic arteries are used as a new “donor”.
- The shunt is checked and the wound is sutured. The procedure can be considered completed.
The operation lasts 3-4 hours. Rarely more. Next, a difficult recovery period begins.
Rehabilitation
The recovery period is long. You cannot wash for two weeks after bypass surgery, as the wounds are extensive and there is a risk of secondary infection. Daily dressings, treatment with antiseptics. You will need to wear a chest bandage for six months to prevent the stitches on your sternum from coming apart.
Average rehabilitation is about three months. During this period, blood and blood flow will normalize, and the sternum will heal. An assessment test for the possibility of a full life is a stress test (for example, bicycle ergometry).
Which is better: a stent or a shunt?
If we compare two methods for correcting myocardial ischemia and hypoxia through the vessels supplying the muscle, the advantages and disadvantages of stenting and bypass surgery of the heart vessels become obvious:
| Evaluation criterion | Stenting | Bypass surgery |
| Scope of intervention | Minimal, intravascular | Technically complex intervention |
| Operation duration | From an hour to three | From three to nine or more |
| Heart failure | Need not | More than half of operations take place with the heart stopped |
| Incision | Deleted | The sternum is cut |
| Anesthesia | Local, less often - taking into account the individual threshold of pain sensitivity | Deep anesthesia |
| Rehabilitation | A few days | Up to six months |
| Acute cases | Relief of AMI is practiced | Not allowed due to the severity of the intervention |
| Capillaries | Correction of vessels with a diameter of 3 mm is possible | Cannot adjust small branches |
| Restoration of blood flow | For several years | Up to 10 years or more |
Forecast
A large amount of research has been conducted regarding cardiac bypass surgery, patient well-being, improved quality of life and increased life expectancy, among other things. Based on the results of these data, you can make a forecast about how long they live after surgery, what positive changes occur in the body, and draw a conclusion for yourself about the need for it.
- Life expectancy increases in all cases. No one will undertake to name exact numbers, since many factors must be taken into account here. But in any case, a person can live much longer.
- The likelihood of developing a myocardial infarction is reduced significantly.
- Quality of life increases compared to drug therapeutic treatment.
No matter how difficult the operation to bypass the heart vessels may be, no matter how much it costs, the result justifies all the efforts and expenses. If there are indications for such treatment, then you need to decide on surgical intervention.
Lifestyle recommendations after surgery
Coronary bypass surgery is a reliable way to prevent heart attacks and angina attacks, since it eliminates ischemia for decades. However, the shunt can narrow; in every fifth patient this happens after a year, and after 10 years - in 100%. To minimize this possibility, you should adhere to seven rules:
- complete cessation of alcohol and cigarettes;
- anti-atherogenic nutritional profile (DASH diet included);
- movement: exercise therapy, walking, sports (swimming);
- minimizing stress;
- a balanced drinking diet (30 ml of water per 1 kg of weight);
- eight hours sleep;
- annual medical examination.
Indications and contraindications for
IHD is usually based on atherosclerosis of the coronary arteries.
Cholesterol accumulates on their walls, and plaques form that impair the patency of blood vessels. The heart receives an insufficient amount of oxygen through the blood flow, and the person feels chest pain similar to angina pectoris. This condition is popularly known as angina pectoris. It manifests itself as pressing, squeezing, burning cardialgia of a paroxysmal nature, initially associated with physical activity or severe anxiety, and later occurring at rest. The indication for coronary bypass surgery of stenotic heart vessels is the need to restore blood flow in the myocardium in the following diseases:
- progressive, post-infarction and exertional angina;
- myocardial infarction.
Such conditions require coronary ventriculography (CVG) before choosing a course of action.
Coronary artery bypass grafting (CABG) is the method of choice if CABG reveals:
- hemodynamically significant stenosis of the coronary vessel of the heart (narrowing by more than 75%), including the trunk of the left coronary artery;
- simultaneous damage to several branches of the riverbed;
- defect of the proximal parts of the right interventricular branch;
- the preserved artery diameter is less than 1.5 mm.
Since heart bypass surgery requires the body to have good recovery capabilities, it has a number of contraindications. These include severe somatic diseases:
- liver (cirrhosis, chronic hepatitis, dystrophic changes) with severe hepatocellular failure;
- kidneys (late-stage renal failure);
- lungs (emphysema, severe pneumonia, atelectasis).
And:
- decompensated diabetes mellitus;
- uncontrolled arterial hypertension.
The age of patients in itself is not a contraindication to heart bypass surgery when there are no severe concomitant diseases.
The doctor considers the listed indications and contraindications comprehensively, determining the degree of operational risk and deciding how to proceed.