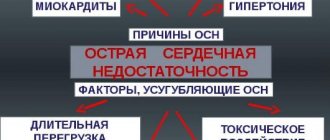
Cardiosclerosis is a pathological replacement of the working muscle tissue of the heart with rigid connective tissue that does not bear a functional load. An inelastic replacement is unable to contract and conduct impulses.
In cardiology, the disease is regarded as one of the manifestations of myocardial damage caused by a deficiency or cessation of blood supply, otherwise known as coronary heart disease (CHD). Cardiosclerosis is classified into four types:
- myocardial cardiosclerosis – a complication of inflammation of the muscular lining of the heart (myocarditis);
- post-infarction cardiosclerosis – consequences of necrosis (death) of a portion of the myocardium;
- primary cardiosclerosis is the result of congenital pathologies of the inner layer of the membrane of the myocardial walls and connective tissue;
- atherosclerotic cardiosclerosis.
According to ICD-10, the disease was assigned code I25.1.
Development mechanism
Atherosclerotic cardiosclerosis develops against the background of coronary atherosclerosis and is a chain of disorders associated with damage to the left and right coronary arteries. Coronary (also known as coronary) arteries are the only source that ensures an uninterrupted supply of arterial blood to the heart.
In atherosclerotic cardiosclerosis, impaired hemodynamics (blood movement) and oxygen starvation of the heart muscle are a consequence of narrowing of the lumen of the coronary arteries. In turn, the cause of stenosis (narrowing) of the vascular bed is pathological deposits of cholesterol on the inner wall of the arteries (intima, endothelium) - atherosclerosis.
Endogenous cholesterol, produced by hepatocytes (liver cells), and exogenous cholesterol, coming from food, are necessary for the body:
- as a basis for sex and steroid hormones;
- as active participants in interneuronal connections of the spinal cord;
- for proper lipid metabolism, absorption of vitamin D and bile acids.
When cholesterol combines with blood proteins, lipoproteins (transport lipids) are formed. The composition of low and very low density lipoproteins (LDL and VLDL) is dominated by fat. Their task is to deliver lipids from the liver to the body’s cells to ensure the above functions.
High-density lipoproteins (HDL) are mostly composed of protein. HDL is responsible for promptly clearing the arteries of excess LDL and VLDL and moving them to the liver for processing and excretion. The well-functioning process of lipid metabolism fails with hypercholesterolemia (an increase in the concentration of cholesterol in the blood due to an increase in the LDL fraction).
Excess low-density lipoproteins “get stuck” in microcracks in the endothelium. This intravascular deposit grows over time and transforms into a hard cholesterol plaque, which partially blocks arterial blood flow.
NC (circulatory failure) or ischemia causes organic and functional inferiority of the myocardium, replacement of functional tissue with connective fibers. Gradually, the replaced areas are deformed into scars, which further complicates the work of the myocardium. With occlusion (absolute obstruction of the vessel), cardiac activity stops. Lack of emergency resuscitation leads to the death of the patient.
Reference! Atherosclerotic plaques are a heterogeneous substance consisting of lipids (to a greater extent), connective fibers, calcium salts, and blood cells.
A type of ischemic heart disease - atherosclerotic cardiosclerosis - is diagnosed in men aged 45+, in women after 50-55 years. The gender difference is due to the cessation in the female body of the synthesis of sex hormones that protect the endothelium during the reproductive period.
Possible causes of the disease
Atherosclerotic cardiosclerosis is usually preceded by ischemic heart disease. The real cause of this disease is high cholesterol. It causes the formation of cholesterol plaques that clog blood vessels.
Also factors in the development of this disease are:
- heredity (if close relatives have this disease);
- gender (men suffer from this disease more often than the fair sex);
- age (the older a person is, the greater his risk of developing cholesterol plaques);
- bad habits (alcohol, smoking, drugs);
- sedentary lifestyle and excess weight;
- unhealthy diet (fast food, excess of sweets and carbohydrates, fatty foods in the diet);
- concomitant diseases (diabetes mellitus, hypertension, kidney disease, etc.).
Even age and heredity cannot affect the development of cardiosclerosis if a person monitors his health, eats right, exercises, follows a routine and avoids bad habits.
Causes of hypercholesterolemia and atherosclerosis
Atherosclerosis develops under the influence of correlation factors: hypercholesterolemia and the presence of microdamage to the endothelium. The normal level of total cholesterol in the blood for adults is 3.2-5.2 mmol/l. Analysis results > 7.7 mmol/l are considered pathologically overestimated.
An increase in LDL and VLDL in the blood is caused by:
- unhealthy eating habits (excessive fatty and sweet foods in the diet);
- low physical activity (hypodynamia);
- long-term psycho-emotional instability (stressful state);
- chronic diseases of the gallbladder and liver;
- malabsorption is a violation of the resorption (absorption) of nutrients in the intestine.
Hypercholesterolemia accompanies diabetes mellitus and other metabolic disorders. Microcracks in the endothelium appear as a result of the aggressive influence of nicotine, alcohol, and certain medications. Intimal damage is caused by:
- diseases associated with blood disorders (including metastatic cancer and diabetes mellitus);
- high pressure on the walls of blood vessels - arterial hypertension.
Fragility of arteries and cracks can be a consequence of hypovitaminosis.
The inner layer of the coronary and all other arteries is protected by flat blood cells - platelets. They are also responsible for blood clotting. When a microcrack appears in the intima, platelets (in large quantities) try to “seal” the damage.
Due to the identical charge of LDL molecules and platelets, excess fats are attracted to the crack, which is the beginning of the formation of cholesterol deposits. At first, a spot forms, then it increases in volume and area, turning into a plaque - an obstacle to blood flow. Then the plaque calcifies and transforms into a hard growth - the cause of NK and atherosclerotic coronary artery sclerosis.
Drug therapy
There is not a single drug that can treat cardiosclerosis.
Therapy is aimed at treating heart failure (relieving its symptoms), maintaining the myocardium and treating concomitant diseases:
- The group of statins is the drug Rosuvastatin and the drug Atorvastatin. Statins lower blood cholesterol;
- A group of antiplatelet agents - to thin the blood. The drug Aspirin;
- Beta blockers to lower the blood pressure index and treat tachycardia - the drug Bisoprolol and Nebivolol;
- Cardiac glycosides drug Digoxin;
- ACE inhibitors - the drug Ramipril;
- Diuretics - Furosemide and the drug Torasemide. Prescribed for heart failure;
- To improve metabolism in the myocardium, the drug Preductal and Trimetazidine.
Lifestyle with cardiosclerosis
Forms of the disease
Atherosclerotic cardiosclerosis is classified according to the degree and extent of myocardial damage. There are two forms of the disease:
- Focal. Difficult to diagnose. Based on the area of damage to individual myocardial areas, it is divided into small-focal (sclerotic zone less than 2 mm) and large-focal (sclerotic zone more than 2 mm). It is practically asymptomatic until the scar lesions grow to large sizes.
- Diffuse. It is characterized by a generalized distribution of connective tissue in the myocardium. The heart muscle acquires a mixed (diffuse) structure. Scars and necrosis form in the altered areas. Extensive lesions are accompanied by severe symptoms characteristic of ischemic heart disease.
In the case when atherosclerosis develops simultaneously in the coronary arteries and the central vessel (aorta), the risk of diffuse cardiosclerosis increases. In addition, when the walls of the aorta (aneurysm) expand and stretch, due to an increase in the volume of cholesterol plaques, there is a danger of rupture of the vessel and instant death.
Classification of cardiosclerosis
Cardiosclerosis is a heart disease in which normal myocardial tissue cells are replaced by scarred ones.
Depending on the area of damage and the extent of scarring, the following forms of cardiosclerosis are distinguished:
- diffuse;
- affecting the valve apparatus.
- focal;
Diffuse form
With this form, they speak of a general degeneration of muscle cells of myocarditis, affecting the entire organ, the entire heart. At the same time, on an ultrasound, the doctor notices changes in all areas of the tissue.
The entire tissue that forms the organ is greatly deformed, and it is impossible to find an area that is not affected by changes. The main danger with this form of cardiosclerosis is the high risk of heart failure.
Focal form
Indicates disease damage to individual parts of the heart.
This type of disease is divided into:
- small-focal - tissue scarring is small and insignificant;
- macrofocal - cover most of the myocarditis.
Previous heart attacks contribute to the development of this form of the disease. If the infarction was extensive, then large foci of sclerotic changes develop. As a result of this process, one of the heart walls can completely atrophy and a wound (aneurysm) forms in its place.
As small lesions develop, small scars form. The development of this form is provoked by hypoxia of the heart, after which it contracts and the ability of tissues to stretch is lost.
Cardiosclerosis with damage to the valve apparatus
A rather rare form of cardiac sclerosis. The valves are mainly affected by other common rheumatological problems.
Defeat can be expressed:
- valve stenosis – characterized by a decrease in the opening inside the valve due to tissue deformation. At the same time, the cardiac load (pressure) increases and serious tissue deformations occur. Subsequently, myocardial hypertrophy develops.
- valve insufficiency - with such deviations, the valve flaps are not completely closed. The development of cardiosclerosis leads to deformation of the valve walls, which aggravates the situation.
Complications
Atherosclerotic cardiosclerosis leads to disruption of the rhythm of heart contractions. Due to the fact that the conducted impulse “stumbles” over a healed area of the myocardium, the heart rate is lost. Types of failures:
- bradycardia – slowing of the rhythm. HR (heart rate) less than 60 beats/min.;
- tachycardia – heart rate more than 140 beats/min. without physical activity;
- extrasystole - uneven contraction of the heart (the most characteristic pathology for cardiosclerosis);
- atrial fibrillation is a chaotic contraction (in the atria the rhythm slows down, while the ventricles contract up to 140-150 times/min.).
Reference! The normal heart rate at rest for an adult ranges from 60 to 90 beats/min.
Unstable myocardial function leads to the development of:
- CHF (chronic heart failure);
- acute necrosis of a portion of the myocardium (infarction);
- congestion in the lungs and pulmonary edema;
- cardiomyopathy;
- sudden cardiac arrest (coronary death).
The main clinical syndrome of pathological changes in cardiosclerosis is angina pectoris (an imbalance in the myocardial oxygen demand and the supply of blood to the heart muscle).
Etiological forms of cardiosclerosis
The identification of forms of cardiosclerosis is associated with the root causes of scarring of myocardial muscle tissue:
- post-infarction;
- myocardial;
- atherosclerotic.
Atherosclerotic cardiosclerosis
This form has a diffuse manifestation and a long course. As the disease progresses, it causes hypertrophy of the left ventricle of the heart, and later its dilatation (increase in the volume of the heart chambers). At the same time, the symptoms of heart failure increase.
Characteristic manifestations for this form of cardiac sclerosis are:
- contractile dysfunction;
- increase in coronary insufficiency;
- broken rhythm.
With atherosclerotic changes in the tissues of the heart, pathologies such as:
- decreased overall body tone;
- swelling;
- dyspnea;
- extrasystole;
- intraventricular blockade;
- atrial fibrillation.
At first, these phenomena are isolated in nature, later they become more frequent and can be observed in patients constantly.
Myocardial
With this form, cardiosclerosis develops according to a different scenario. The sclerotic process affects the heart muscle itself (myocarditis) and cardiomyocytes. Severe inflammation occurs, causing the death of the muscle cell membrane. After the acute phase, an increase in connective tissue is observed, which is not able to enable the muscle to fully cope with its functions.
The causes of myocarditis include:
- intoxication of the body (drugs, alcohol);
- bacteria (streptococci, meningococci);
- viruses (Coxsackie, rubella, influenza).
It can develop in people of different ages.
Post-infarction
This form is also called postnecrotic. It is diagnosed 2-4 months after the heart attack, when the scarring process is completed. Myocardial muscle tissue is partially affected by necrosis. This occurs due to the proliferation of sclerotic replacement tissue cells.
Scars can vary in size and location, which determines the nature and severity of the abnormality in the functioning of the organ.
The overgrown sclerotic tissue cannot fully perform the contractile function, which leads to further development of arrhythmia.
After a heart attack, dilatation and an increase in myocarditis and the development of failure are possible. Also, sclerotic transformations in the post-infarction state can develop in the heart valves.
Other causes of the disease
Other mechanisms that provoke sclerotic changes in heart tissue include:
- sarcoidosis of the heart - the organ is affected by an inflammatory process. With treatment, inflammation disappears, but is replaced by connective tissue, which contributes to the development of cardiosclerosis.
- hemochromatosis – a disease in which excessive accumulation of iron occurs in the thickness of the heart tissue. This leads to intoxication and inflammation of the heart muscle;
- exposure to radiation - the received dose of radiation can change the molecular structure of cells, which leads to the spread of unhealthy tissue in the organ;
- scleroderma - there is an increase in the organ due to thickening of the walls. There is no tissue inflammation, but connective tissue begins to grow from the capillaries;
- idiopathic cardiosclerosis - the nature of its occurrence is not clear. Most doctors agree that this is due to family predisposition.
Symptoms
Atherosclerotic cardiosclerosis progresses slowly. Primary symptoms are not specific. Changes in the myocardium are manifested by slight shortness of breath, chronic drowsiness and fatigue, accelerated fatigue, tingling in the subclavian region (left).
Patients note increased heart rate, pale skin, and short-term numbness in the fingers of the left hand. As the sclerotic areas increase, sharp chest pain occurs (angina pectoris syndrome). Periodically, the heart “stabs”, and pain is felt not only in the heart area, but also on the left side of the body (under the shoulder blade, under the collarbone, in the arm).
Developing:
- dyspnea (shortness of breath);
- heart rate disturbance (tachycardia, bradycardia);
- painful sensations in the epigastric region, accompanied by nausea;
- dry chest cough;
- insomnia (insomnia).
At a later stage, the symptoms of coronary heart disease are added to the listed signs. Swelling of the face and lower limbs. Dizziness, periodic clouding of consciousness, fear of death, manic anxiety, and fainting occur. Angina attacks last up to 15 minutes.
One of the signs of hypercholesterolemia is fatty growths under the skin of the eyelids - xanthomas.
Types of development of sclerosis of the heart organ
Cardiosclerosis is divided into types depending on the degree of damage to the muscular part of the heart organ:
- Diffuse sclerosis;
- Small focal cardiosclerosis, which occupies a large area of the cardiac myocardium.
Pathogenesis of diffuse type of cardiosclerosis
If the process of scarring and replacement of cardiomyocytes with fibrous tissue covers a large area of the cardiac myocardium, or does not have pronounced boundaries of the lesion, then this is called a diffuse type of cardiosclerosis.
In the first periods of pathology development, a mesh of scars is formed, and between the mesh there are healthy cardiomyocytes. The muscle tissue that is located in these cells of the scar network performs a contractile function.
As diffuse cardiosclerosis progresses, an increasing part of the myocardium is replaced by fibrous tissue and the contractility of the heart is significantly reduced.
It is impossible to allow complete replacement of myocardial cells with scar tissue, because this instantly leads to death.
It is impossible to allow complete replacement of myocardial cells with scar tissue
Pathogenesis of focal type of cardiosclerosis
If the pathology is limited only to a small area of fibrous tissue on the myocardium, and has fairly clear boundaries, then a focal type of cardiosclerosis develops. In a simple explanation, it is like a scar on the cardiac myocardium.
The scar consists only of connective fibrous tissue, and cardiomyocyte cells are not present in it, which becomes the reason for the ability of this part of the heart muscle cells to contract.
If the scar does not affect the main functional parts of the heart and the impulse conduction system, then this pathology does not cause any symptoms of improper functioning of the cardiac myocardium, but if the scar affects the main tissues in the left ventricle, or the IVS, then the heart rhythm is disturbed and the person feels signs of a malfunction hearts.
Diagnostics
The diagnosis of “atherosclerotic cardiosclerosis” is based on the results of laboratory and instrumental studies. The patient receives an appointment for tests and diagnostic procedures upon presentation of symptomatic complaints. Characteristic changes in the biochemical blood test indicate myocardial damage.
An increase in enzyme concentration is determined:
- aspartate aminotransferase (ALT);
- creatine phosphokinase (CPK);
- lactate dehydrogenase (LLH).
The lipidogram (the patient's lipid profile, which determines the quality of fat metabolism) shows a significant excess of the norm for total cholesterol, triglycerides, low and very low density lipoproteins. A general clinical blood test determines the hanging platelet count, the discrepancy between thrombocrit and platelet indices from normal values.
A number of pathological changes are recorded during a coagulogram (blood clotting test). Primary examination of the heart - ECG (electrocardiogram) reveals areas of the myocardium that have lost the ability to conduct impulses.
Depending on the nature and intensity of the violations, the following may be prescribed:
- transthoracic or transesophageal echocardiography - ultrasound of the heart with an external probe or a tubular probe through the esophagus;
- echocardiography with Doppler – examination of the aorta and coronary arteries;
- stress echocardiography – ultrasound of the heart in a calm state and after a dynamic load (physical exercise or administration of medications);
- coronography - x-ray of the coronary arteries of the heart with the introduction of a radiopaque substance.
If possible, magnetic resonance imaging or computed tomography of the cardiovascular system is performed.
Types of illness
The disease manifests itself actively both among older people and among young people and even occurs in childhood. Cardiosclerosis is classified according to the prevalence of the pathological process and has two corresponding forms:
- Focal cardiosclerosis;
- Diffuse cardiosclerosis.
The focal form of the disease manifests itself in the form of scar formation in the myocardium, occupying various areas. Focal manifestations of the disease are often provoked as a result of successfully survived myocardial infarction or myocarditis. Thus, there are small-focal and large-focal types of manifestation of this form.
Large-focal is caused by the formation of extensive myocardial infarctions based on previous myocardial infarctions. This form is characterized primarily by the subsequent growth of massive fields of connective tissue. As a result of complete overgrowth of the walls, a scar is formed, which contributes to the manifestation of a cardiac aneurysm.
The small-focal appearance is characterized by minor lesions of the connective tissues and appears in the form of white layers that are located in the thickness of the myocardium. The small-focal form occurs when there is insufficient oxygen in the chambers of the heart muscle. Thus, this leads to the reduction and subsequent death of cardiac muscle cells.
Diffuse cardiosclerosis is formed based on the uniform distribution of connective tissue throughout the myocardium. Often the diffuse form occurs when a person has a chronic form of coronary artery disease.
All heart diseases are dangerous manifestations, since the human “engine” is a rather fragile creation that requires care and attention. Almost all manifestations of cardiosclerosis have fatal consequences, especially if appropriate treatment measures are not taken.
Classification by etiology
Post-infarction cardiosclerosis
Based on the reasons that caused certain factors of illness of the cardiovascular system, in medicine the following classification is distinguished according to etiological criteria:
- Post-infarction cardiosclerosis , formed as a result of an experienced attack of myocardial infarction. It is also called myocardial.
- Atherosclerotic cardiosclerosis is formed on the basis of atherosclerosis of the coronary vessels.
- Postmyocardial cardiosclerosis is formed due to the development of inflammatory processes in the myocardium.
These are three main classes of disease, which have characteristic signs of etiology development. So, let's look at each type in more detail.
Post-infarction cardiosclerosis is directly related to the complication of myocardial infarction. Very often, after a heart attack, after some time, doctors diagnose post-infarction cardiosclerosis.
When the heart is damaged in the form of a blood clot in the artery, muscle cells die and do not grow back. If the person was saved by dissolving the blood clot, then the oxygen supply is resumed, but the dead heart cells do not have the opportunity to recover. In their place, connective tissue begins to actively grow, which ultimately forms rough scars. After active tissue growth and scar formation, myocardial hypertrophy begins. This means that scars bind the surface of the heart muscle and the latter has to increase in volume to fulfill its purpose. This phenomenon is a matter of time, so if post-infarction cardiosclerosis is not treated, then eventually the heart will simply fail.
The development of an aneurysm is also caused by the predominance of the post-infarction type of the disease. An aneurysm is a disease that manifests itself in the form of a protrusion of the walls of the left cardiac ventricle, where the growth of connective tissue actually occurs. An aneurysm often contributes to a decrease and disruption of blood flow in the body and leads to the development of heart disease.
Atherosclerotic cardiosclerosis is based solely on the presence of coronary heart disease in a person. It is characterized by the duration of the formation of abnormalities in the heart and the appearance of the first signs. The main reason for the long-term formation of signs of the disease is poor blood supply to the myocardium, resulting from damage to the coronary vessels. Long-term formation of this form of cardiosclerosis leads to atrophy of the cells of the muscle tissue of the heart, which, in turn, causes the development of acquired heart defects. Atherosclerotic cardiosclerosis is predominantly diffuse in nature, that is, it is caused by the proliferation of connective tissue over the entire surface of the heart muscle.
Postmyocardial cardiosclerosis occurs mainly in the population aged 20 to 40 years. The reason for its development is the predominance of infectious diseases, allergic reactions and other inflammatory or chronic processes in the body. Postmyocardial cardiosclerosis, like atherosclerotic one, is predominantly diffuse in nature.
It is also worth highlighting another important type of disease, which is called congenital cardiosclerosis. It manifests itself in very rare cases, and the cause of its formation is congenital abnormalities in the cardiovascular system.
Treatment
Conservative treatment of atherosclerotic cardiosclerosis is aimed at eliminating the symptoms of ischemia, correcting blood composition, improving blood circulation, increasing the density and elasticity of arterial vessels.
In advanced stages of the disease, drug therapy is inappropriate. To restore hemodynamics, the patient undergoes surgery to correct the arteries. Regardless of the chosen treatment tactics, the medical diet “Table No. 10” is prescribed, intended to eliminate hypercholesterolemia.
Groups of medications
Prescribed drugs are divided into several pharmacological groups:
How to lower blood cholesterol levels?
- Statins. Slow down the production of endogenous cholesterol. As a result, the level of LDL decreases and the content of HDL in the blood compensatory increases.
- Fibrates (fibric acid derivatives). Normalize lipid metabolism and the balance of lipoproteins of different densities.
- Calcium channel blockers and angioprotectors. They tone the walls of the arteries, strengthen the endothelium, and enhance the contractility of blood vessels.
- Anticoagulants and antiplatelet agents. Reduce high blood clotting rates characteristic of coronary artery disease and its manifestations.
- Bile acid sequitrants. Stimulate hepatocytes to use excess low-density lipoproteins for bile synthesis.
- Cardiac glycosides are plant stabilizers of rhythmic myocardial contractions.
- Vitamin PP (nicotinic acid) is an active participant in lipid metabolism.
- Nitroglycerin preparations for the relief of angina attacks.
At the same time, hypertension, metabolic disorders and other chronic diseases are treated.
Diet therapy
Diagnosed atherosclerosis, as a trigger for cardiovascular pathologies, is poor eating behavior, nicotine addiction, and addiction to alcoholic beverages. First of all, cardiologist patients are advised to review their diet, quit smoking, and give up alcohol.
The diet for atherosclerotic cardiosclerosis excludes the consumption of foods rich in animal fats, baked goods, smoked products, sausages, fast food, and pickles. It is prohibited to eat foods prepared by frying (including over charcoal).
Dietary nutrition is organized on the basis of slow carbohydrates (dishes from legumes, grains and cereals), fiber and vitamins (vegetables, herbs, berries, fruits), foods rich in Omega acids (linseed oil, fish, seafood, nuts). The rules of the diet indicate adherence to the eating regimen (every 3-4 hours in small portions).
A short list of products for atherosclerotic disease
Beverage classification
| Refuse | Introduce into your diet on a regular basis |
| coffee | freshly squeezed fruit and vegetable juices |
| alcohol (any strength) | berry compotes and jelly |
| energy | decoctions of rosehip, linden |
| sweet cocktails and juices |
When compiling a daily menu, special attention should be paid to compliance with the daily calorie intake and the ratio of nutrients.
Surgical intervention
With intense negative dynamics of the disease, surgical methods are used in treatment. Depending on the progressive changes, one of the following types of surgery may be prescribed:
- coronary bypass surgery - creation of an artificial channel for blood flow bypassing the atherosclerotic section of the coronary artery;
- aneurysm resection – excision of the damaged area of the aorta of the heart followed by prosthetics;
- RFA (radiofrequency ablation) – endoscopic cauterization of a section of the myocardium that blocks cardiac impulses;
- angioplasty of coronary vessels with stenting - dilation of arteries by installing a wall.
In difficult cases, an electrical pacemaker (ECS) is implanted.
Symptoms of cardiosclerosis
To maintain the normal strength of heart contractions, a certain number of muscle fibers are required. The more of them are replaced by connective tissue, the lower the cardiac output. This explains the asymptomatic course of cardiosclerosis with a small lesion.
If the pathological process has affected a significant part of the myocardium, then the patient develops symptoms of heart failure. They may appear as follows:
| Symptom of heart failure | Characteristics of the symptom | Why does it happen? |
| Dyspnea | More often, it is more difficult for the patient to inhale; in some cases, the entire breathing process is difficult. The time at which shortness of breath occurs depends on the degree of heart failure. At the initial stage of the disease, the symptom occurs only after severe exercise (running, lifting heavy objects, etc.). With severe myocardial dystrophy, the patient finds it difficult to breathe even at rest. | If the heart cannot “pump” blood with the required force, it begins to stagnate in the vessels of the lungs. Because of this, they expand and the liquid part of the blood is “pushed” through the vascular wall into the alveoli - the part of the lungs where gas exchange occurs. Air cannot enter the blood in sufficient quantities and the patient experiences difficulty breathing, which increases with exercise. |
| Edema | Heart failure is characterized by swelling in the legs. Often, this is the first symptom of an onset of illness. However, with an advanced process, swelling can appear on the face, hands and even in internal organs. | Edema and shortness of breath have a similar mechanism of development. In the first case, insufficient cardiac output leads to stagnation of blood in the vessels of the entire body. And since the pressure is greatest in the veins of the legs (due to gravity), swelling first of all appears there. |
| Low blood pressure | Develops only in the later stages of the disease. The presence of this symptom is an extremely unfavorable sign. | Normal blood pressure is 120-139/70-89 mmHg. It is maintained due to cardiac output and vascular tone. If the heart cannot contract with sufficient force, blood output decreases and blood pressure drops. |
| Pain in the right hypochondrium | The symptom often develops in patients with severe edematous syndrome. The pain is dull or aching in nature and is not relieved by NSAIDs (Ketorol, Analgin, Nise, etc.). It intensifies with pressure on the hypochondrium and does not radiate anywhere. | The cause of these pains is an enlarged liver due to stagnation of blood in the portal vein. |
| Acrocyanosis | Acrocyanosis is a cold and bluish discoloration of the distal parts of the extremities (hands, feet, lower third of the legs and forearms). As a rule, this symptom persists constantly and may intensify with physical activity. | With significant damage to the myocardium, cardiac output is insufficient to “drive” blood to all parts of the body. Therefore, the most distant parts (ends of the arms/legs) experience insufficient blood supply. |
| Dizziness and fainting | This symptom appears only with prolonged progression of the disease. Dizziness persists constantly and can significantly reduce the patient’s quality of life. Fainting is usually rare. Their appearance is provoked by physical/emotional stress. | In the development of these symptoms, two points are important: a sharp decrease in blood pressure and heart rhythm disturbances. Often, they accompany each other, but can cause dizziness separately. |
| Appearance changes |
| All these signs arise due to impaired microcirculation of blood through various tissues. |
In addition to the general symptoms of cardiosclerosis listed above, patients may present additional complaints related to the cause of the development of the pathology.
Complaints with ischemic heart disease
The main symptom that worries patients with coronary artery disease and cardiosclerosis is pain. It is always located behind the sternum and has an aching or pulling character. Irradiation is possible to the left shoulder blade, arm, right shoulder. A characteristic feature that allows one to reliably confirm the presence of coronary artery disease is the rapid (within 5 minutes) disappearance of pain after taking Nitroglycerin.
The time of occurrence of painful attacks depends on the form of coronary artery disease:
- Angina pectoris - only after physical exertion. The pain goes away within 3-5 minutes after rest;
- Prinzmetal's angina is a spontaneous onset of pain, mainly at night. Patients may wake up from a pressing feeling in the chest, which goes away only after using Nitroglycerin;
- Unstable angina – pain occurs both during exercise and at rest. They gradually progress, occurring more frequently and becoming more intense. This type of angina is an absolute indication for hospitalization in a cardiology hospital.
As a rule, symptoms of IHD prevail over signs of cardiosclerosis. With adequate treatment of the initial stages, it is possible to completely eliminate patients’ complaints and return them to their previous quality of life.
Symptoms of myocarditis
It is difficult to make this diagnosis, since there are no absolute symptoms of myocarditis. Most often, in addition to the symptoms of cardiosclerosis, patients may present the following complaints:
- Fever up to 40°C, weakness, headache, decreased/loss of appetite;
- Attacks of palpitations, a feeling of “interruptions” in the work of the heart, abnormal rhythm;
- Acute cutting pains that are located to the left of the sternum.
Cardiosclerosis can appear both against the background of myocarditis and after it. It is possible to reduce the likelihood of its development by promptly seeking medical help.
Signs of systemic diseases
Regardless of the type of systemic disease (scleroderma, lupus erythematosus), there are characteristic signs that allow them to be suspected in the early stages. The most common symptoms include:
- Skin damage:
- the appearance of a rash in the form of pinpoint hemorrhages;
- increased sensitivity to sunlight;
- hair loss on the head and torso;
- causeless constant dry skin.
- "lupus butterfly" An almost absolute symptom of lupus erythematosus is the appearance of a characteristic butterfly-shaped rash on the face. Its middle part is located in the nose area, and the “wings” extend to the cheeks, lower eyelids and nasolabial triangle.
- Changes in mucous membranes - characterized by the appearance of pinpoint hemorrhages and severe dryness;
- Raynaud's phenomenon - spontaneously occurring numbness and cyanotic coloration of the fingers;
- Joint damage – all patients develop arthritis due to systemic diseases. Patients complain of pain and stiffness in large joints, which increase in the morning. Swelling and redness of the skin over them, as a rule, are absent.
This is far from a complete clinic of systemic diseases, however, it is the above symptoms that often make it possible to detect the possible cause of cardiosclerosis.
Results
Atherosclerotic cardiosclerosis is one of the types of coronary heart disease. During the disease process, living, functional myocardial tissue is replaced by non-functional connective tissue.
Scars are formed, the free movement of blood, the saturation of the heart with oxygen, the conductivity of impulses, and the contractility of the myocardium are disrupted. Pathological changes develop against the background of progressive atherosclerosis of the aorta and coronary arteries. The consequences of unstable cardiac activity can be myocardial infarction, CHF, and coronary death.
Causes and consequences of the development of cardiosclerosis
| development mechanism | reasons that depend on the mechanism | common types of pathology |
| myocardial dystrophy due to malnutrition | · IHD in the chronic stage; | diffuse type of pathology of cardiosclerosis |
| · atherosclerosis of the coronary arteries; | ||
| · pathology cardiomyopathy; | ||
| Cardiodystrophy. | ||
| necrotic destruction of cells of myocardial tissue fibers | myocardial infarction; | focal type of development of cardiosclerosis |
| heart surgery; | ||
| myocardial injury. | ||
| inflammatory process of the heart organ | · pathology myocarditis of viral and infectious etiology; | cardiosclerosis of both types of disease development |
| · rheumatism of the heart. |
Symptoms
The clinical picture depends on the phase of development and the severity of the narrowing of the diameter of the lumen of blood vessels. At an early stage, there are no manifestations at all or they are so minimal that they do not attract attention.
As long as the body is able to compensate for the disorder, there will be no signs. Then, as it becomes impossible to correct the deviation, problems begin.
A complete list of those for cardiosclerosis of atherosclerotic origin is presented by the following points:
- Chest pain. Varying degrees of intensity. The character is burning or pressing, bursting. They go to the stomach, arm, neck, face. Mostly of medium or minimal strength.
- Dyspnea. As a result of increased physical activity. But gradually the threshold decreases, and the intensity of the mechanical load necessary for the development of the symptom decreases. As a result, it comes to the point that a person is not even able to move, perform basic actions around the house, in everyday life. Not to mention anything more. In the decompensation phase of heart failure, the symptom may develop at complete rest.
- Arrhythmia. According to the type of supraventricular tachycardia (sinus). The heart rate rises to 120 beats or more. It occurs in attacks, and then becomes chronic and exists constantly; the patient just gets used to it and stops paying attention to the disorder.
- Severe weakness, drowsiness. Asthenic phenomena. The reason is a decrease in myocardial contractility and insufficient nutrition of cerebral structures and the brain.
- Peripheral edema. The ankles suffer, only then do central disorders develop, affecting the face. This is the result of increasing heart failure. Read more about the symptom here.
- Headache. Neurological sign. They develop as the pumping function of the myocardium decreases and, accordingly, there is a small release of blood into the systemic circle, from where it must flow to all organs and tissues, including the brain.
- Cough without sputum. An alarming sign. Indicates increasing symptoms of cardiac asthma. Hemoptysis is gradually added for the same reasons.
- Mental disorders of the neurotic spectrum, depressive type. Usually we are talking about emotional instability, insomnia, and apathy.
As soon as the disease reaches a certain peak, tachycardia is replaced by the reverse process. The heart rate drops, which indicates a failure of the cardiac structures.
Emergency conditions become a logical outcome of long-term cardiosclerosis.
Attention:
The disease itself never regresses, this is an axiom. Move only forward. The rate varies, but it usually takes several years to become critically ill.
Kinds
There are two forms of atherosclerotic cardiosclerosis:
- Diffuse small focal;
- Diffuse macrofocal.
The disease is divided into 3 types:
- Ischemic – occurs as a consequence of prolonged fasting due to lack of blood flow;
- Post-infarction - occurs at the site of tissue affected by necrosis;
- Mixed - this type is characterized by the two previous characteristics.
Treatment and observation by a doctor
Atherosclerotic cardiosclerosis is a slowly progressive disease, the lack of treatment of which leads to failure of the heart muscle (areas of dead muscle cells are replaced by connective tissue).
Taking into account the characteristics of this condition, I highlight the main directions of treatment for the disease:
- whenever possible, compensation for the underlying disease;
- symptomatic correction (elimination of edema syndrome, restoration of rhythm, support of myocardial contractile function);
- lipid-lowering therapy;
- lifestyle modification;
- prevention of complications.
The treatment plan for atherosclerotic cardiosclerosis should include:
- A set of physical activity, quitting smoking and alcohol.
- Special diet: limiting the intake of sodium, water, unsaturated fats, gas-forming products, coffee, strong tea. Fractional 5-6 meals a day. Regular weighing.
- Lipid-lowering drugs (Atoris, Rosuvastatin).
- Diuretics (“Furosemide”, “Trifas”, “Veroshpiron”).
- ACE inhibitors (Enap, Lisinopril).
- Beta-blockers (“Bisoprolol”).
- Antiplatelet agents (Cardiomagnyl, Clopidogrel).
- If necessary: ytrates (“Nitroglycerin”);
- cardiac glycosides (Digoxin).
How to make a diagnosis
The diagnosis of “atherosclerotic cardiosclerosis” can only be established on the basis of a detailed examination of the patient for myocardial damage, blockage of coronary vessels and dyslipidemic changes in the blood serum.
The examination plan for a patient with suspected atherosclerotic coronary artery sclerosis includes:
- Laboratory blood test:
- cholesterol level, lipoprotein fractions;
- blood sugar, glycosylated hemoglobin (HBA1c);
- glucose tolerance test;
- biochemical study - creatinine, urea, ALT, AST;
- coagulogram, international normalized ratio (INR);
- hemoglobin, hematocrit;
- natriuretic peptide.
- Electrocardiography:
- standard at rest (12 leads);
- with dosed physical activity (bicycle ergometry, treadmill test);
- 24-hour Holter monitoring.
- EchoCG (ultrasound examination will accurately show the degree of myocardial hypertrophy, ejection fraction, size of the heart chambers, condition of the valve system). Recently, stress echocardiography has been introduced into practice - the study is performed in combination with physical activity on a treadmill or bicycle ergometer.
- Myocardial scintigraphy (OFCET, PET). The essence of the method is the intravenous administration of a radionulide marker (technetium99). The quality of the blood supply to the heart muscle is examined (the better it is, the more the radiopharmaceutical accumulates in the tissue; well-nourished areas have a bright glow). This scan in combination with stress tests has the greatest diagnostic information value.
- CT scan:
- CT visualization of the coronary arteries without the introduction of contrast - calcification index (cholesterol plaques, during their growth, go through the stage of calcium deposition in them, which can be seen on the scan);
- CT coronary angiography is a study of the coronary arteries using intravenous contrast.
- Invasive coronary angiography. The most accessible method for visualizing atherosclerotic lesions of the heart vessels. During the procedure, a conductor with a contrast agent is inserted through the femoral artery into the coronary artery and the location of the narrowing is determined using x-rays.
All cardiac imaging methods will help make a differential diagnosis between different types of cardiosclerosis (post-infarction, atherosclerotic, myocardial).
Diagnostic measures and treatment
Diagnosis of the disease includes the collection and analysis of patient complaints, medical history and lifestyle. After this, a physical examination is performed aimed at:
- Detection of swelling;
- Determination of the condition and color of the skin;
- Blood pressure level measurement;
- Detection of abnormal heart sounds.
To identify concomitant chronic diseases, the doctor prescribes a general blood test. Biochemistry is performed to determine the level of cholesterol, LDL, VLDL and HDL. Next, the patient is sent for a number of additional studies.
An ECG is done to establish heart rhythm disturbances, detect scars and diffuse myocardial changes. Echocardiography is prescribed to identify an area of the heart that is no longer able to maintain contractile function and consists of replaced tissue. Holter ECG monitoring is performed to detect arrhythmia. To identify the focus of cardiosclerosis, the patient is sent to an MRI, and scintigraphy is performed to determine the size of the pathological lesions and determine the possible cause of the disease.
Danger and complications
Cardiosclerosis is a rather dangerous disease that can cause complications such as acute or chronic heart failure . Acute failure can occur as a result of blockage of the heart vessels by an embolus or thrombus. Such phenomena often lead to rupture of the artery and death of the patient.
Chronic insufficiency is formed against the background of gradual narrowing of the arteries due to atherosclerotic processes . Such cardiosclerosis can lead to cardiac hypoxia, ischemic heart disease, atrophy or dystrophy of cardiac tissue.
Other complications of this disease are cardiac arrhythmias, cardiac aneurysms, chronic fatigue syndrome, thromboembolism, and acquired defects.
Complex treatment of cardiosclerosis
You need to understand that cardiosclerosis is not a fatal disease or a depressing illness, it is a way of life, coexistence with such a feature of the heart. You can live an absolutely fulfilling life by following a diet, physical activity and taking medications. You can enjoy life by taking control of the disease.
Photo: https://pixabay.com/photos/doctor-doctor-s-office-stethoscope-3464761/
Therefore, an integrated approach in the treatment of cardiosclerosis is important, teamwork between the doctor and the patient working towards a single result - human health.
So how do you need to change your lifestyle?
Control body weight
The first stage of lifestyle changes is to monitor the efficiency of the heart and the effect of drug therapy by controlling hidden edema. If your body weight has increased by 2 kg in 5 days or by 3 kg in 7 days, you should contact a cardiologist or adjust the therapy yourself according to the algorithms given by the doctor.
Follow a diet
Excess body weight or obesity worsens the prognosis and course of the disease, therefore, with a body mass index of more than 25 cm/kg2, you should adhere to a diet that limits caloric intake depending on age and somatic norms. At the same time, the diet should contain a sufficient amount of protein - mainly fish, lean poultry, legumes, contain a lot of polyunsaturated fatty acids, vegetables and fruits (up to 500 g per day).
It is necessary to exclude or minimize the intake of processed meat, simple carbohydrates, salty, fatty, fried foods, and canned food from the diet. The amount of table salt supplied with food should not exceed 6 g/day, which corresponds to moderate salting of food during cooking or “do not add salt to food,” since a large amount of essential sodium and chlorine enters the body with foods that do not contain salt.
Liquids should be limited only if the patient’s condition is severe with severe edema; in other cases, it is recommended to drink about 1.5 l/day.
Do physical exercise
You can and should do physical exercise! Even if the patient’s condition is serious, it is necessary to practice breathing exercises even while sitting in bed, starting from a few minutes a day, increasing the pace, since it has been proven that increasing the body’s fitness improves the patient’s prognosis and his quality of life.
Starting with breathing exercises with a gradual increase in intensity and improvement, over time the patient can move on to aerobic exercises such as walking, then running, cycling, swimming and water exercises, Nordic walking. The level of tolerable and suitable load is taken into account taking into account the six-minute walk test (how many meters the patient can walk in 6 minutes). The motor regimen should be prescribed and discussed with the patient by the attending physician.
Follow recommendations for a healthy lifestyle
Smoking is contraindicated for all categories of patients. Alcohol should also be excluded, but the recommendations of the Russian Cardiological Society are a little softer - no more than 250 ml of beer or 125 ml of wine per day. It is also recommended that patients be vaccinated against influenza and pneumococcal infections annually according to the vaccination plan.
Photo: https://pixabay.com/photos/a-change-in-lifestyle-banana-diet-1430599/
Psychological support for patients
It has been scientifically proven that prevention of depression, work with a psychoanalyst in groups and schools of heart failure improves the prognosis of patients and has a positive effect on the dynamics of the disease.
Prevention
Even in the early stages, cardiosclerosis is incurable; irreversible changes can only be stopped. The most effective way to prevent cardiosclerosis is to prevent the development of coronary atherosclerosis. You can achieve your goal by adhering to the following rules:
- no smoking;
- do not abuse alcohol;
- play sports, move more;
- Healthy food;
- control blood pressure.
An important component of prevention is cholesterol control. Biochemical changes precede clinical symptoms by several years. Early detection of hypercholesterolemia allows one to take measures to prevent the development of atherosclerosis. It is recommended that healthy adults have their sterol levels checked every 4 to 6 years.
Prevention of cardiosclerosis
The first stage of prevention is constant monitoring by a cardiologist or therapist, treatment of the underlying cardiac pathology.
It is also important to undergo an annual examination: do an ECG, ultrasound of the heart, take blood tests for cholesterol and sugar.
It is worth observing the work and rest schedule, not performing heavy physical activity, engaging in physical education, and monitoring blood pressure levels.
Follow the Mediterranean diet rules in your diet, consume healthy and tasty food, drink at least 1.5 liters of water per day.