Hypertension (HD) is rightfully considered a disease of civilization. The rhythm of life and habits dictated by modern society provoke the development of many pathologies. Obesity, atherosclerosis, angina pectoris, gastrointestinal diseases, and hypertension are based on non-compliance with the rules of a healthy lifestyle. Knowing the etiological factors and pathogenesis of hypertension, you can avoid its occurrence or reduce the severity of symptoms. It is important to know what the pathophysiology of the disease is.
Hypertension – persistent increase in blood pressure
What is arterial hypertension
Hypertension (hypertension, hypertension) is persistently increased blood pressure, as a result of which the structure is damaged and the functioning of the heart and arteries is disrupted.
According to the WHO classification (1999), normal blood pressure numbers are as follows:
- A blood pressure of up to 120/80 millimeters of mercury is considered optimal;
- Blood pressure less than 130/85 is considered normal;
- to normal elevated - 130-139/85-89.
In case of an increase in pressure numbers above those indicated earlier, the condition is called arterial hypertension and is divided into degrees:
- degree one (mild hypertension) - from 140/90 to 159/99;
- degree two (moderate hypertension) - from 160/100 to 179/109;
- degree three (severe) - more than 180/110;
- borderline hypertension - in the case of an episodic increase in blood pressure to 140-149/90 and its subsequent spontaneous normalization;
- Isolated systolic hypertension - cases when arterial systolic pressure is stably elevated, while diastolic pressure remains normal or reduced (140/90).
Causes of hypertension
In most cases of arterial hypertension, the etiology (pathogenesis will be discussed below) of the disease remains unclear. In such cases we speak of primary (essential) hypertension. This form of pathology is usually diagnosed in elderly patients.
In 10% of cases, hypertension is a symptom of other pathologies or a side effect when taking certain medications. This type of hypertension is called secondary. The most common causes are: taking antipyretic and steroid drugs, cortisone, pathologies of the endocrine organs and kidneys.
In addition, there are factors that provoke the development of a persistent increase in blood pressure:
- pathological changes in cholesterol metabolism;
- excessive body weight;
- burdened heredity;
- smoking;
- large amounts of table salt in food;
- alcohol abuse;
- deficiency of potassium in food.
Primary arterial hypertension: pathogenesis
The development of this pathology requires an increase in cardiac output, as well as an increase in peripheral total resistance, or a combination of these factors.
The pathogenesis of arterial hypertension does not imply the simultaneous participation of various mechanisms of blood pressure regulation. At the beginning of the disease, the increase in pressure is neutralized by mechanisms that normalize it. It is the influence of these mechanisms on each other that determines the occurrence of pathology.
The triggering factor in the pathogenesis of arterial hypertension is prolonged nervous overstrain, which leads to a decrease in the inhibitory effect of the cortex on the subcortical centers of the brain and, as a consequence, the emergence of stagnant foci of excitation in the hypothalamic-pituitary system. This process disrupts the functioning of the autonomic subcortical centers, as well as protein-fat metabolism. Which in turn triggers the following mechanism of the pathogenesis of arterial hypertension - persistent overexcitation in pressor centers, leading to spasm of arterioles and an increase in blood pressure.
All this excites the baroreceptors of the aortic arch and carotid sinus, which leads to stimulation of the vasomotor centers in the medulla oblongata and the pressure decreases. However, this process “works” only in the initial stages of the pathology.
In case of further persistence of nervous overstrain, the load on the sinocarotid zone (its baroreceptors) increases. And disturbances in the central regulation of vascular contractions are accompanied by an increase in the amount of catecholamines due to activation of the sympathetic-adrenal system, which also contributes to an increase in blood pressure.
Spasms of the renal arterioles (which also occurs in primary arterial hypertension, the etiology of which is discussed in this article), combined with the influence of the sympathetic system, triggers the so-called renal factor, and blood pressure increases even more.
Renal hypertension
The pathogenesis of renal arterial hypertension is associated with:
- retention of water and sodium ions;
- activation of the renal factor (aldosterone-angiotensin-renin system);
- inhibition of renal depressor systems (renal prostaglandins and kallikreinin system).
The trigger mechanism in the development of renal hypertension is a decrease in blood flow in the kidneys and filtration in the glomeruli, which develops both as a result of vascular lesions and changes in the parenchyma. Due to a decrease in renal blood flow, the absorption of sodium and water increases, and their retention in turn leads to hypervolemia and, as a result, the amount of sodium in the vascular wall increases, which causes swelling of the wall and an increase in its sensitivity to aldosterone and angiotensin.
Activation of the angiotensin-aldosterone-renin system is one of the main points determining the pathogenesis of secondary arterial hypertension (renal etiology). Renin, secreted by the kidneys, is a proteolytic enzyme that combines with serum alpha-2-globulin to become angiotensin 2, which increases blood pressure and stimulates the production of aldosterone by the adrenal glands, which in turn increases sodium absorption by the kidneys. In parallel with the processes described, the compensatory capabilities of the kidneys are depleted, which also leads to an increase in blood pressure.
Where does hypertension come from?
To date, the main cause of the development of hypertension has not been established, therefore this pathology is called primary or essential. In each individual case, it is caused by a combination of disturbances in regulatory processes.
The causative factors for the manifestation of hypertension are a lot of features:
- burdened heredity;
- excessive addiction to table salt;
- gender identity;
- age;
- stress;
- increased weight;
- alcoholic drinks;
- smoking;
- physical inactivity.
Hypertension can be caused by metabolic syndrome, kidney disease or thyroid disease.
The role of heredity in the pathophysiology of essential hypertension has been known for a long time. Many scientists believe that this is the main etiological factor in the development of hypertension. The dependence of the functioning of the renin-angiotensin-aldesterone system (RAAS) on the mutation of genes encoding this process has been established. It is also important that impaired insulin sensitivity and the functioning of the endothelium (the inner lining of the artery) are also mediated by heredity.
The connection between excessive salt intake and the development of arterial hypertension has been proven by numerous multicenter studies.
It is believed that the use of more than 6 g of salt daily with a family history is a reliable trigger for the development of hypertension. This connection is also proven by the high effect of a salt-free diet in patients with hypertension.
Stress, negative emotions, and increased anxiety are of particular importance in the development of pathology. Due to constant overexcitation of the sympathetic nervous, hypothalamic-pituitary and adrenal systems, there is a load on the cardiovascular system. This explains the fact that hypertension is not uncommon among people in “stressful” professions.
To avoid the development of hypertension, you need to eat right and move more.
The negative impact of alcohol on all body systems is undeniable. It has a toxic effect on the walls of blood vessels and the nervous system. In this case, the mechanism of blood pressure regulation is disrupted. When drinking alcoholic beverages, the heart rate accelerates and cardiac output increases.
When smoking, a reflex spasm of arterioles occurs, which leads to hypoxia (lack of oxygen). As a result, total peripheral vascular resistance increases and blood pressure rises. Systematic repetition of the pathological process ends in the development of hypertension.
Symptomatic hypertension
The causes of symptomatic or secondary hypertension are different:
- renal pathologies (nephrogenic arterial hypertension etiology, pathogenesis, clinical picture, treatment are described in other sections of this article);
- endocrine diseases (thyrotoxicosis, pheochromocytoma, Conn and Itsenko-Cushing syndrome);
- hemodynamic disorders (presence of various heart/vascular defects);
- taking certain medications;
- pathologies of the nervous system.
The mechanisms of development of such hypertension are different. That is, symptomatic arterial hypertension, the pathogenesis of which is different, depends on the cause and characteristics of the underlying disease.
- For example, in renal pathologies, the main factor is renal ischemia, and the main mechanism determining the increase in blood pressure is a decrease in depressor agents and an increase in pressor agents.
- In the case of endocrine pathologies, increased release of certain hormones leads to increased blood pressure (catecholamines, corticosteroids, ACTH, aldosterone, growth hormone).
- In the presence of organic damage to the nervous system, ischemia occurs in the centers that control blood pressure.
- In the case of hemodynamic secondary hypertension, which develops as a result of lesions of blood vessels or the heart, the mechanisms of increase in blood pressure are different and depend on the nature of the lesion. The main mechanisms are:
- dysfunction of the sinocarotid zone and decreased elasticity of the aorta (for example, with atherosclerosis of the latter);
- excess blood in the vessels that are located above the aortic narrowing (for example, with coarctation of the aorta), leading to the development of a renopressor ischemic mechanism in the kidneys;
- vascular constriction as a consequence of a decrease in cardiac output and an increase in blood volume, as well as an increase in blood viscosity caused by secondary hyperaldosteronism (occurs in congestive heart failure);
- acceleration and increase in systolic blood output (in the case of aortic valve insufficiency) with prolongation of diastole (in the presence of complete AV block) or with an increase in blood flow to the heart (with arteriovenous fistulas).
Etiology of hypertension
Risk factors
Heredity, stressful situations, excessive consumption of table salt, insufficient intake of magnesium and calcium from food and water, smoking, alcohol, obesity, low physical activity - all these factors contribute to increased blood pressure and the development of hypertension (HD) or arterial hypertension (AH) . The risk of developing hypertension has been noted to be higher among people with lower socioeconomic status.
This is explained by the fact that people with low incomes pay less attention to a balanced diet, proper active recreation due to lack of material resources, and also smoke and drink alcohol more. It is worth highlighting a separate form of hypertension - “white coat” hypertension, which occurs in people only when visiting a doctor due to anxiety and psycho-emotional stress, at home, in a familiar environment, the blood pressure of such individuals is within normal limits.
If the cause of hypertension cannot be clearly established, there is a connection with heredity, it is more common in men and the incidence increases with age, we are talking about primary (essential) hypertension. It accounts for about 80% of all hypertension. The etiology of arterial hypertension of secondary origin (the incidence of the secondary form is about 20% of all identified cases of high blood pressure) is directly related to the disease that caused it.
Renal hypertension
The following types of secondary (essential) hypertension are distinguished:
- Renal hypertension. The cause of such hypertension is diseases of the kidneys and renal vessels: congenital malformations, infections, anomalies and disorders of the kidney vessels, diseases of the kidney tissue (glomerulonephritis, pyelonephritis, amyloidosis);
- Endocrine hypertension. The reason for the increase in blood pressure lies in disorders of the endocrine organs: pathology of the adrenal glands, excessive thyroid function, acromegaly, hormonal imbalances during menopause;
- Hemodynamic hypertension. When large vessels and the heart are damaged, symptomatic hypertension may occur: coarctation of the aorta, ischemia, circulatory congestion, valvular insufficiency, arrhythmias and other disorders;
- Neurogenic hypertension. Hypertension caused by pathological activity of the nervous system and brain diseases: brain tumors, inflammation (meningitis, encephalitis), trauma, vascular disorders.
In addition to the main causes of symptomatic hypertension, there are also special causes of pathologically high blood pressure:
- Salt or food hypertension: develops as a result of excess salt intake in food, or excessive consumption of foods that contain tyramine - cheese, red wine;
- Drug-induced secondary hypertension - develops when taking certain medications that can cause hypertension.
Variants of Arterial Hypertension
In accordance with the etiology and pathogenesis of arterial hypertension, several varieties of this pathology are distinguished:
- Transient hypertension. Accompanied by periodic increases in blood pressure lasting up to a couple of days. After the specified time, the pressure numbers return to the initial (normal) values spontaneously (that is, without the use of any drugs). Most often, this variant of the course is regarded as the initial stage of hypertension (hypertension).
- Hypertension is labile. Accompanied by periodic episodes of increased blood pressure due to the influence of various provoking factors (for example, heavy physical activity, stress). In these cases, medications help lower blood pressure.
- Hypertension is stable. It is characterized by a persistent increase in blood pressure, which decreases only with the use of medications followed by maintenance therapy.
- Hypertension is malignant. This form of pathology is accompanied by an increase in blood pressure to extremely high values. In this case, the disease quickly progresses and leads to the development of serious complications, often leading to death.
- Crisis option. It is accompanied by periodically occurring hypertensive crises, which are sudden surges in pressure with slightly increased or normal pressure.
Stages of the disease
Hypertensive syndrome or hypertension is a disease that progresses and, as it develops, passes from one phase to another. There are the following stages of the pathological process:
- first (easiest);
- second;
- third (with the risk of death).
The first stage of the disease is the easiest. A person’s blood pressure level does not constantly rise; this condition does not cause any particular harm to internal organs. Treatment of this form of the disease is carried out without the use of drug therapy, but under the supervision of a specialist.
In the absence of any actions aimed at treating high vascular tone, the disease can progress to a more severe form - the second stage. In this case, damage to internal organs that are sensitive to sudden changes in pressure is already possible. These include the organs of vision, kidneys, brain and, of course, the heart. A person develops the following pathologies:
- pathologies of the carotid arteries (intimal thickening, development of atherosclerotic plaques);
- microalbuminuria;
- narrowing of the retinal arteries;
- pathology of the left ventricle of the heart.
In case of a third degree disease, all internal organs receive serious damage, complications including death are possible. The following conditions develop against the background of arterial hypertension:
- aortic dissection;
- proteinuria;
- retinal hemorrhages;
- vascular dementia;
- acute hypertensive encephalopathy;
- transient ischemic attack;
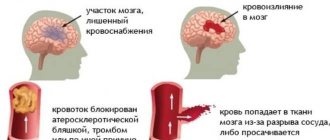
- stroke;
- heart failure grade 2–3;
- myocardial infarction.
If diagnosis is not made in a timely manner or test data is not interpreted correctly, the chance of a successful outcome for the patient is reduced.
Arterial hypertension in children
The pathogenesis, as well as the causes of this pathology in childhood, are different. There are several forms of diseases that lead to increased blood pressure in children:
- hypertonic disease;
- VSD (hypertensive variant);
- symptomatic secondary hypertension (diseases of the kidneys, central nervous system, endocrine organs, heart defects).
The pathogenesis of the development of this pathology in children is the same as in adult patients, however, the blood pressure numbers regarded as hypertension may differ from those in adults.
Arterial hypertension in pregnant women: pathogenesis, classification, treatment approaches
Arterial hypertension in pregnant women and associated pathological changes are one of the main causes of maternal, fetal and neonatal mortality, and these rates do not differ significantly in developed countries and third world countries. According to some data, preeclampsia and hypertension in pregnancy are serious risk factors for the development of coronary heart disease (CHD) and arterial hypertension (AH) after childbirth. A survey of 600 thousand women in Norway revealed an 8-fold increase in the risk of coronary artery disease and hypertension over 13 years in the group of patients who had preeclampsia with premature birth. During a physiological pregnancy, blood pressure decreases in the second trimester by an average of 15 mmHg. Art. In the third trimester, blood pressure returns to its original level or increases further. Such blood pressure fluctuations are typical for both normotensive and initially hypertensive women and patients with gestational hypertension. There is no consensus regarding the blood pressure levels at which hypertension can be diagnosed during pregnancy. It is customary to focus on an increase in blood pressure in the second trimester compared to the level of the first trimester or pre-pregnancy levels. However, assessment of absolute blood pressure values (SBP > 140 mm Hg or DBP > 90 mm Hg) is considered more reliable when diagnosing hypertension during pregnancy.
Pathogenesis
Against the background of hormonal changes accompanying pregnancy, vascular smooth muscles relax, the subsequent formation of placental blood flow and fetal blood circulation occurs, and the volume of circulating blood increases. Pregnancy is characterized by sodium and water retention, with sodium retention being about 900 mmol and water retention being 6-8 liters. Approximately 2/3 of the retained water and sodium are distributed throughout the mother's body. There is also usually dilatation of the afferent and efferent arterioles of the glomerulus with a 50% increase in renal plasma flow and glomerular filtration. Another physiological phenomenon is the change in the regulation of antidiuretic hormone (ADH) during pregnancy. There is a shift in the “trigger point” for ADH release. The consequence of this is disproportionate water retention in the body, moderate dilution hyponatremia and a decrease in serum osmolality. In addition, in the third trimester, under the influence of placental vasopressinase, the metabolic breakdown of ADH increases, and therefore symptoms of diabetes insipidus may occur.
Among the mechanisms leading to an increase in blood pressure during pregnancy, fluctuations in the levels of hormones of the pressor and depressor systems, such as natriuretic peptide and endothelial factors, are considered. In addition, during pregnancy there is an increase in the circulating blood of renin, angiotensin, corticoids, especially aldosterone, deoxycorticosterone and progesterone. There is also evidence of changes in the secretion of vasodilating prostanoids, NO synthase (NOS) and nitric oxide, which are responsible for the decrease in peripheral resistance during normal pregnancy.
The development of hypertension during pregnancy often precedes preeclampsia (PE), understanding the pathogenesis of which is extremely important, given the severity and prognosis of this pathology. The etiology and pathophysiology of PE are completely unclear. Among the mechanisms of PE, various disorders are considered.
Placental disorders. Perhaps the basis is remodeling of the spiral arteries, leading to uteroplacental hypoxia, which can be aggravated by substances that damage the maternal vascular endothelium. It has been established that in PE the expression of cytotrophoblasts is disrupted and adhesion molecules trigger the process of vascular remodeling. Other authors note that in women with the T235 gene variant of angiotensinogen, the activity of the local RAAS in the vessels of the placenta may change, which is fraught with inadequate angiogenesis with possible thrombus formation in small-diameter vessels. Importance is given to factors leading to apoptosis, human leukocyte antigen G (which may be important in disrupting maternal tolerance to the placenta), and an increase in trophoblast growth factors and other placental proteins.
Impaired vascular reactivity . Increased maternal vascular reactivity due to the effects of endogenous pressor substances can lead to blood pressure lability and is the cause of peripheral vasoconstriction observed in PE. Theories of the development of PE are based on the assumption of an imbalance of vasodilating prostanoids and other pressor systems, such as endothelin and angiotensin II, and the presence of receptor disorders with the appearance of autoantibodies - AT1 receptor agonists. In addition, there is damage to NOS production, NO-dependent and -independent vasodilation. Maternal endothelial dysfunction may also be caused by increased cytokine levels, vitamin and mineral deficiencies, or oxidative stress. It has been established that the state of pregnancy leads to an imbalance in the activity of circulating antioxidants and oxidants in favor of the latter. The production of free radicals may increase.
Insulin resistance and sympathetic hyperactivity . In the pathophysiology of hypertension, the role of insulin resistance (IR) has been proven. Insulin resistance is characteristic of normal pregnancy. Some researchers have noted a higher IR in women with PE and in women with a history of preeclamptic pregnancy. The increased tone of the SAS described in PE may be due to hyperinsulinemia and may lead to vasoconstriction.
Activity of the RAAS system. Unlike healthy pregnant women, women with PE have lower levels of circulating components of this system. At the same time, there is activation of cellular and tissue components of the RAAS, which cause remodeling of placental vessels. With PE, the sensitivity of receptors to A2 in different tissues increases. Polymorphism of the angiotensinogen gene increases the incidence of PE.
Immunological changes . Fetoplacental antigen plays an important role in the etiology of PE. The higher incidence of PE in first pregnancies also supports the immune theory. The risk for PE usually decreases with repeated pregnancies, but if the father is different, the risk returns to the original. This concept contradicts the common belief that long intervals between pregnancies with the same partner are often associated with PE.
Genetic factors . The presence of a gene or genes that predict the development of PE indicates the familial nature of PE. The hereditary risk of PE has been shown and several specific alleles associated with PE have been described (this was first described by Chesley in the 60s). Gene variations associated with hypertension, thrombophilia, endothelial dysfunction, and vasoactive hormones have been studied in various combinations. The results are mixed.
Classification of hypertension
A pregnant woman is diagnosed with arterial hypertension in the following situations:
- SBP > 140 mm Hg. Art., and DBP > 90 mm Hg. Art.;
- increase in SBP by > 25 mm Hg. Art. or DBP > 15 mm Hg. Art. compared with blood pressure before pregnancy or in the first trimester.
Chronic (pre-existing) hypertension occurs in 1–5% of pregnant women and is characterized by blood pressure > 140/90 mm Hg. Art. Hypertension was present before pregnancy or appeared before the 20th week of pregnancy and was recorded more than 42 days from the moment of detection. Such hypertension may be associated with protenuria.
Gestational hypertension is induced by pregnancy and is not characterized by protenuria. Gestational hypertension associated with significant proteinuria (more than 300 mg/l or more than 500 mg at 24 hours) is regarded as preeclampsia. This hypertension develops after 20 weeks. pregnancy. In most cases, it progresses within 42 days from registration. Gestational hypertension is characterized by impaired organ perfusion.
Pre-existing hypertension + layered gestational hypertension with proteinuria. Pre-existing hypertension associated with a progressive increase in blood pressure and protein excretion > 3 g/day after the 20th week of pregnancy; in the old classification it was positioned as “chronic hypertension with risk of preeclampsia.”
Unclassified hypertension is hypertension with or without systemic manifestations when hypertension is first reported after the 20th week of pregnancy. Repeated blood pressure monitoring is necessary on the 42nd day or later. If arterial hypertension progressed during this time, then the situation should be classified as gestational hypertension with or without proteinuria. If hypertension has not progressed, the case should be classified as pre-existing hypertension (chronic hypertension).
Edema occurs in 60% of women during normal pregnancy and is not a reason for diagnosing preeclampsia.
Increased blood pressure during pregnancy, especially gestational hypertension, with and without proteinuria, can lead to hematological, renal and hepatic changes that worsen the prognosis for the mother and fetus. For pregnant women with arterial hypertension, a set of general clinical laboratory tests is recommended (Table 1).
Antihypertensive therapy
Most women with pre-existing hypertension have mild to moderate hypertension during pregnancy (140–179/90–109 mm Hg) and a low risk of cardiovascular complications throughout pregnancy. Hypertension with normal renal function indicates a good prognosis for the mother and fetus; such women are candidates for non-drug therapy, since at present it has not been proven that the results of pharmacotherapy are absolutely safe for the fetus.
Non-pharmacological treatment of hypertension is prescribed to pregnant women with SBP 140–149 mm Hg. Art. and/or DBP 90–99 mm Hg. Art. Management tactics depend on the level of blood pressure, the age of the pregnant woman, the presence of risk factors for the mother and fetus and include dynamic observation, limitation of physical activity, rest in bed in a position on the left side. A normal diet without salt restriction is recommended. Preventive actions aimed at reducing the risk of developing gestational hypertension and, especially, preventing eclampsia, including the prescription of calcium supplements (2 g per day), fish oil supplements and low doses of aspirin, are unjustified, particularly in relation to the fetus. However, low-dose aspirin is used in women with early (less than 28 weeks' gestation) preeclampsia. Weight loss helps reduce DBP in non-pregnant women, but is not recommended for obese women during pregnancy, as it can lead to fetal malnutrition.
The volume and duration of drug therapy in women with chronic hypertension remain under discussion. The need for drug therapy in pregnant women with severe hypertension is beyond doubt.
Therapeutic interventions for hypertension during pregnancy should reduce the risk to the mother and fetus. When SBP > 170 mm Hg. Art. and/or DBP > 110 mm Hg. Art. urgent hospitalization is indicated.
The US FDA (Food and Drug Administration) regularly publishes data on the safety of various medications during pregnancy. According to the presented classification, only very few drugs can be classified as category A, while the majority of drugs used to treat arterial hypertension in pregnant women belong to category C (Table 2).
Central α2-agonists
Methyldopa (dopegyt, aldomet, dopanol) is a first-line drug for the treatment of hypertension in pregnant women. The effectiveness of this drug has been proven.
In the 70s A randomized placebo-controlled trial showed a reduction in perinatal mortality with methyldopa. Another study looked at long-term effects in children whose mothers took this drug during pregnancy and found no negative effects over 7 years. The drug does not interfere with uteroplacental blood flow and fetal hemodynamics. Thus, methyldopa is safe for both mother and fetus. Hypertensionists often criticize obstetricians for using this drug, believing that methyldopa is less effective and less well tolerated than new drugs. However, all comparative studies of methyldopa and other antihypertensive drugs have not proven advantages in the effectiveness and safety of the latter. Another α2-agonist, clonidine (clonidine, Hemitone), can be prescribed to pregnant women, although experience with its use is less extensive. Thus, in one study, the effectiveness and safety of these drugs were equivalent. Another study in hospitalized women found that clonidine alone or in combination with placebo or hydralazine reduced the incidence of preterm birth. Clonidine should be avoided in early pregnancy due to the risk of embryopathies. In one small neonatal prospective study, an increased incidence of dyssomnia was reported in the clonidine group. In addition, this drug has been used relatively rarely in recent years due to other side effects (dry mouth, depression, withdrawal symptoms).
Vasodilators
Parenteral hydralazine is not a therapeutic option for the treatment of sudden increases in blood pressure in pregnancy, as its use is associated with a higher perinatal risk compared with other drugs. However, there is also an opposite point of view. For the treatment of chronic hypertension, it is used as a second-line agent in combination with methyldopa or beta-blockers. Side effects include headache, dizziness, and tachycardia. There are limited studies on the successful use of hydralazine as monotherapy.
Despite the abundance of literature on this issue, the safety of β2-blockers (BABs) in pregnant women and the indications for their use are still unclear, due to conflicting research results. In many studies, treatment with these drugs was prescribed late, which makes it difficult to assess the reliability of negative effects, especially fetal growth retardation. The greater number of complications when using beta blockers concerns the fetus. These drugs can impair the resistance of the fetal cardiovascular system to hypoxia, causing bradycardia, respiratory depression, hypoglycemia and developmental delay. Many of the reported effects are derived from animal studies and descriptive reports. And only delayed fetal development has been documented. Most large human studies have not found conclusive evidence of other side effects in the fetus. The use of atenolol is associated with an increased incidence of fetal growth restriction and decreased placental weight due to its ability to increase resistance in the fetal vessels (umbilical artery and aorta). However, in a control study conducted a year later, this effect was not confirmed. Most likely, only long-term use of atenolol is accompanied by these side effects, while its short-term use in later stages is relatively safe. When treatment was started in late pregnancy, atenolol, metoprolol, pindolol and oxprenolol did not cause undesirable effects.
These drugs are indicated for long-term treatment of hypertension in pregnant women if methyldopa and hydralazine (and even labetolol) do not control blood pressure or cannot be prescribed for some other reason.
α-blockers
Data on the use of these drugs in pregnancy are sparse, descriptive, and non-evidence-based. The only indication for their use is rare cases of pheochromocytoma in pregnant women.
α-, β-blockers
Labetolol is the most studied drug in this group, used in pregnant women with hypertension. Parenteral forms are used to treat severe arterial hypertension. Some researchers believe that drugs in this group are more effective and safe (including the frequency of side effects such as headache, arrhythmias, hot flashes) than parenteral administration of hydralazine. Other researchers find no differences. Data on the use of labetolol for chronic hypertension in pregnant women are presented by several randomized studies, which failed to identify any advantages of labetolol over methyldopa. Reports of fetal growth retardation associated with labetolol are contradictory, and long-term outcomes in children are unknown. Possible hepatotoxic effect. Labetolol can therefore be used as a second-line agent.
Calcium antagonists
These drugs are used to treat acute and chronic hypertension in pregnant women. Most studies are descriptive and concern the use of calcium antagonists (CAs) in severe hypertension. Oral short-acting drugs can provoke a sharp uncontrolled drop in blood pressure (decreased placental blood flow and decreased maternal cerebral perfusion). This is especially true when combining calcium antagonists with intravenous administration of magnesium sulfate (severe cases of hypotension and inhibition of myocardial contractility have been described). Thus, it is better to avoid prescribing calcium antagonists for rapidly progressing hypertension in pregnant women. Data regarding the use of these drugs in chronic hypertension in pregnant women are also contradictory. In a multicenter randomized trial, neither benefit nor harm from the use of nifedipine was recorded for the mother and fetus. A multicenter, prospective, cohort study examining the use of nifedipine in the first trimester of pregnancy did not find an increase in the incidence of major malformations. The calcium antagonist nimodipine is used by neurologists to treat impaired cerebral perfusion in women with eclampsia. Thus, nifedipine is indicated for pregnant women with chronic hypertension in cases where hypertension is refractory to treatment with methyldopa or β-blockers or there are contraindications to their use.
Diuretics
Data on the use of diuretics are conflicting. When using them, inhibition of the physiological increase in plasma volume in pregnant women was noted. Suboptimal expansion of plasma volume may be associated with oligohydramnios and fetal growth disturbances, but these data are inconclusive. Another problem is hyperuricemia while taking diuretics, which can cause errors in the diagnosis of preeclampsia. At the same time, there is no doubt about the advantages of diuretics in the treatment of the salt-sensitive hypertensive population, especially in cases of rapidly developing refractoriness to vasodilators. Many researchers recommend continuing diuretic therapy for hypertension prescribed before and during pregnancy. Thiazide diuretics appear to be safe and effective drugs for the treatment of hypertension in pregnant women, especially in combination therapy, due to their ability to potentiate the effect of other antihypertensive drugs. They are contraindicated during pregnancy in cases where the uteroplacental circulation is already reduced (preeclampsia and/or intrauterine growth retardation). A meta-analysis of 9 randomized trials, which included more than 7 thousand women receiving diuretics, revealed a decrease in the development of edema and/or arterial hypertension and did not confirm an increase in the incidence of adverse outcomes for the fetus.
ACE inhibitors and AT1 receptor antagonists
ACE inhibitors are contraindicated during pregnancy as their use is associated with intrauterine growth retardation, oligohydramnios (as a result of fetal oliguria), impaired fetal renal function and neonatal mortality. Data on the development of bone dysplasia (impaired ossification of the cranial vault and shortening of the limbs) have been published. Despite the lack of information on the use of AT1 antagonists in pregnant women, experimental data (fetal and neonatal mortality from renal failure) allow us to recognize that these drugs are absolutely contraindicated during pregnancy.
Breast-feeding
There are rather sparse data on this subject, which, unfortunately, indicate that most antihypertensive drugs are excreted in breast milk, sometimes in concentrations that can cause hypotension in newborns. Relevant information is presented in the monograph by Briggs et al., the recommendations of the Committee on Drugs of the American Academy of Pediatrics, reviews by White, Dillon, and others. It is believed that if the mother is receiving antihypertensive therapy, breastfeeding is not contraindicated, with the exception of treatment with propranolol and nifedipine, the concentrations of which are in breast milk are the same as in maternal plasma. In other cases, the concentrations of antihypertensive drugs in milk are quite low and can be regarded as safe.
Arterial hypertension, which is the most common complication of pregnancy and the main cause of maternal and perinatal mortality in pregnant women, remains a poorly understood disease. Due to little progress in understanding its pathogenesis and a lack of evidence to support the introduction of new therapeutic agents, its treatment has not changed significantly in recent decades. Today we can say that hypertension in pregnant women can be radically cured only by childbirth.
There is an urgent need for an in-depth study of this pathology. Appropriate clinical trials, although at first glance appear extremely complex and low-cost, could ultimately provide valuable information that could significantly reduce the risk of maternal and perinatal morbidity and mortality.
For questions regarding literature, please contact the editor.
T. V. Adasheva , Candidate of Medical Sciences, Associate Professor O. Yu. Demicheva MGMSU, State Clinical Hospital, Moscow
Clinic
When blood pressure rises, patients complain of:
- noises in the ears, head;
- headache (pulsating or pressing), which is localized in the temples and back of the head;
- decreased performance;
- dizziness and heaviness in the head;
- mood changes;
- poor sleep;
- stars/flies, veil/mesh before the eyes;
- heartbeat;
- dyspnea;
- swelling;
- decreased vision;
- general weakness;
- interruptions in cardiac activity;
- double vision;
- squeezing/aching pain in the heart.
Upon examination, attention is drawn to pallor of the skin, occasionally redness of the face, and in the long-term - acrocyanosis, swelling (pastyness) of the legs (first the feet, and then the legs).
Studies of the heart and blood vessels confirm elevated blood pressure numbers, as well as left ventricular hypertrophy or dilatation.
A local examination reveals increased pulsation at the cardiac apex, abdominal aorta, temporal and carotid arteries. On palpation: an increase in the area of the apical impulse and its displacement downward and outward.
The pulse with this pathology is frequent, hard and tense. Upon percussion, the left border is shifted outward, and subsequently there is an expansion of the boundaries of the vascular bundle.
On auscultation: increased 1st tone at the apex. In the case of severe disease, there is a gallop rhythm and systolic murmurs at the apex.
Diagnostics
If episodes of high blood pressure occur, a visit to the doctor cannot be postponed, since perhaps irreversible changes are already developing in the body, which require serious therapy.
Diagnosis of hypertension includes collection of anamnesis, complaints, examination and laboratory and instrumental studies.
At the initial stage, blood pressure is measured, but to confirm the diagnosis, elevated pressure numbers must be recorded in at least 3 independent measurements.
Laboratory and instrumental studies include:
- blood test (general);
- ECG;
- detailed clinical blood test with determination of lipid levels;
- urine test (general);
- Ultrasound of the heart and other organs;
- consultation with an ophthalmologist with examination of the blood vessels of the eyes.
In addition, if the presence of secondary hypertension is suspected, the doctor prescribes additional studies of other systems and organs whose diseases can lead to arterial hypertension. Moreover, the list of necessary studies is individual for each patient.
Diseases accompanying high blood pressure
In addition to hypertension, there are a number of diseases accompanied by increased blood pressure: kidney pathologies (chronic pyelo-/glomerulonephritis), renovascular hypertension (caused by narrowing of the renal artery), adrenal tumor - pheochromocytoma, coarctation of the aorta (congenital vascular defect), endocrine disorders (syndrome Conn, Itsenko-Cushing's disease). To exclude the presence of these pathologies, the doctor prescribes a comprehensive examination. Additional examination is aimed at detecting pathologies of target organs. It allows you to clarify the stage of hypertension and prescribe appropriate treatment.
Diagnostic measures include:
- ECG: there may be signs of left ventricular enlargement (hypertrophy), ischemic changes, signs of acute myocardial infarction.
- X-ray of the chest organs: changes in the contour of the heart can be detected (manifestation of left ventricular hypertrophy);
- echocardiography (ultrasound of the heart): hypertrophy of the left ventricle, dilation of the cavities of the heart, and a decrease in its work may be detected;
- fundus examination: narrowed retinal arteries, dilated veins are determined, in later stages - hemorrhages, exudates, edema;
- blood test: the amount of cholesterol, kidney function indicators (creatinine, urea) are determined;
- Urinalysis: detects renal dysfunction, microalbuminuria, etc.
Therapy
Treatment of arterial hypertension comes down to maximally reducing the risks of heart and vascular diseases, as well as reducing blood pressure to normal values, that is, less than 140/90.
To achieve these goals, it is recommended to constantly take maintenance doses of antihypertensive drugs, a special diet with limited salt and cholesterol, quit smoking/alcohol, reduce body weight, and increase physical activity.
In addition, ACE inhibitors, diuretics, beta blockers and calcium antagonists are used as drug treatment.
In the case of secondary hypertension, the underlying disease is treated.
Treatment and prevention
For hypertension, patients will definitely need to undergo a course of treatment, which includes both medications and physiotherapeutic procedures. Most often, patients are prescribed medications that reduce fluid levels in the body, which will help lower blood pressure. The attending physician also prescribes sartans, that is, drugs that block angiotensin II receptors. Their effect is that they reduce blood pressure and allow it to remain at this level for a day.
If the patient has detected disturbances in the functioning of the heart, then in this case calcium antagonists will be needed. If necessary, vasodilators and drugs are prescribed to normalize the heart rhythm. Particular attention is paid to the nutrition of patients suffering from hypertension. It is necessary to significantly reduce consumption or completely avoid foods that increase blood cholesterol levels. Therefore, the diet should not contain fatty, fried and smoked foods, and it is also important to reduce the amount of salt consumed.
As for preventive measures, it is important to normalize the functioning of the entire body, and not just the cardiovascular system. Normal sleep has a positive effect on the body, it should be at least 8 hours, you should go to bed at the same time. If you have night jobs, you need to give them up.
Proper nutrition is included not only in the course of treatment, but is also considered an excellent preventative norm; add more vegetables and fruits to your diet. Give up bad habits and normalize physical activity; if there is a lot of it, reduce it; if you have constant sedentary work, you need to increase its quantity. One of the most important factors is psychological health. It is the stress experienced that most often provokes the development of this disease. Meditation and auto-training can be used as prevention. If the first symptoms occur, you should consult a doctor. Do not start self-treatment of the disease; this approach will not only not eliminate the problem, but may also worsen the existing condition.