Hypertensive encephalopathy is an acute (less often chronic) severe malnutrition of the brain against the background of a simultaneous jump in blood pressure. This disorder is a complication of hypertension.
How quickly it occurs in a particular patient is a controversial issue and depends on many factors. Encephalopathy is accompanied by a difficult general situation. It is considered a pre-stroke condition, therefore, if the development of such a serious complication is suspected, urgent hospitalization in a hospital is required.
The effectiveness of primary measures and further therapy depends on many factors. Therefore, the prospects for recovery are vague.
There are no uniform statistics, but the mortality rate of hypertensive encephalopathy, or rather what it entails - stroke, is extremely high.
Development mechanism
It is based on a group of violations. The patient may have a single factor or a system of them. In this case, the risks of a negative outcome, as well as the overall severity of the condition, are many times higher.
In all cases, the direct culprit of the pathological process is a stable increase in blood pressure, and the retention of equally high numbers for a long time. Risks begin to increase from the range of 150/90 mmHg and above.
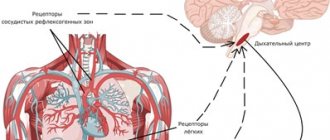
Instability of blood pressure leads to a reflexive further narrowing of the arteries that supply cerebral tissue. Dysfunction itself causes precisely the same reason.
The vessels lose their normal tone as a result of a biochemical reaction and the release of large amounts of angiotensin-2, renin, aldosterone, and cortisol. It is also possible that there is a violation of the regulation of arterial tone on the part of the nervous system.
The pressure continues to rise. The brain does not receive enough nutrients and oxygen. In particularly difficult cases, the risks of vessel rupture and hemorrhage are high.
But hypertension itself does not exist in isolation. It has a lot of reasons, fundamental mechanisms of the pathological process.
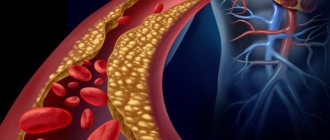
For example, narrowing of the lumen of the arteries as a result of the deposition of cholesterol plaques on their walls. This is the so-called atherosclerosis.
Or constant narrowing, decreasing diameter as a result of chronic spasm. As happens with experienced smokers and alcohol drinkers. This is just the tip of the iceberg.
Further, the process accelerates development.
Acute hypertensive encephalopathy begins suddenly and proceeds aggressively. From the moment of the first symptoms to a critical condition (stroke) it can take only a few hours or even less.
The diameter of the vessels continues to decrease, and the blood has to overcome greater resistance. The body seeks to compensate for insufficient trophism (nutrition) by increasing blood pressure. It's a vicious circle. If it is not broken, the death of cerebral structures cannot be avoided.
Knowing the patterns of development of hypertensive encephalopathy, it is possible to urgently plan treatment and increase the patient’s chances of survival.
There is also a chronic type of the disease. It is provoked by the same mechanisms, but is formed sluggishly. For several months, or even years.
This is a definite plus, because there is time for high-quality diagnostics and full-fledged treatment.
Forecast
With DEP 1, the prognosis is favorable. The progression of the disease is unlikely to be stopped, but it is possible to reduce the severity of symptoms and lead a full life. To do this, it is important to maintain a healthy lifestyle and adhere to medical recommendations.
When the disease moves to the second stage, recovery can only be said if the cause that caused it can be eliminated surgically. Otherwise, the disease progresses. Gradually the patient's condition will worsen and lead to disability. Timely comprehensive treatment of DEP 2 allows you to delay the appearance of signs of the third stage for up to 10 years.
Discirculatory encephalopathy is a complex disease that destroys the emotional, cognitive and motor spheres of human life. The prognosis can be favorable with early detection of pathology, its treatment and prevention. Pronounced symptoms indicate an organic lesion and are difficult to treat.
Symptoms depending on stage
Practitioners and medical theorists distinguish three main phases of the pathological process.
First stage
Refers to the compensated form. Hemodynamic (blood flow) disturbances already exist; they are registered based on the results of Dopplerography of blood vessels, and an increase in blood pressure also makes itself known.
But so far the violation is not so critical. There is every chance of a full correction. In addition, the symptoms are barely noticeable.
Among the possible manifestations:
- Headache. Not strong, but monotonous and very annoying. Accompanies a person for a significant part of the day and occurs in attacks. It intensifies against the background of jumps in the tonometer reading. Therefore, it depends on vascular tone and is of arterial origin. By nature - aching or pulling, shooting. It is well relieved with analgesics.
- Dizziness and spatial disorientation. The patient feels that the world is spinning, but can still keep himself normal. Walk and even perform professional duties with almost no restrictions.
- Nausea, rarely vomiting.
- Weakness, drowsiness, asthenic phenomena. The pathological process is accompanied by a decrease in the quality of brain trophism. Nervous tissues are extremely “gluttonous” and require a lot of energy. The only way out is to minimize the required amount by transferring the cerebral structures to “standby mode.” Therefore, problems with intelligence and concentration develop. Lethargy.
- Behavioral disorders. So far the patient is at the level of irritability, tearfulness and increased aggressiveness.
In some cases, there are no symptoms at all at the first stage or they are extremely scarce. They intensify as encephalopathy transforms.
Second stage
Decompensation of the process. The body is still able to maintain cerebral blood flow, but not to its full extent. Neurological deficits become apparent.
Possible manifestations of the violation include:
- Severe headache. Excruciating. Usually short-term. Lasts about an hour or a little more. Variations are possible.
- Nausea, vomiting.
- Loss of consciousness.
- Syncope.
- Weakness, the same asthenic phenomena.
- Irritability.
- Decline in thinking abilities. Cognitive impairment is particularly common. First, as a type of decrease in productivity, and then they lead practically to dementia.
- There may be a decrease in motor activity. A person has less control over his own muscles. Faces, limbs. Although formally there are no paresis or paralysis.
The second stage of hypertensive encephalopathy is characterized by almost identical symptoms, but much more severe than in the first stage.
Quality treatment is still possible, although full recovery is not expected. Structural changes in the brain have already begun from a lack of nutrients and oxygen. They cannot be reversed.
There are, however, chances to bring the disease under control, eliminate symptoms and prevent further progression.
Third stage
Accompanied by decompensation. The patient's body can no longer correct problems with blood circulation. There is total dysfunction of the central nervous system. Efficiency drops to zero, the person becomes disabled.
Identical manifestations are detected, but in a critical form. The same neurological deficit puts an end to the ability not only to work, but even to social interaction. Including with loved ones.
Recovery is basically impossible. There are chances to partially eliminate the symptoms, but not the cause itself. The next natural outcome is a stroke and then death.
Regardless of the stage. There is always an objective disorder—high blood pressure. The numbers depend on the provocateurs, as well as the individual characteristics of the cardiovascular system of a particular patient.
Symptoms of hypertensive encephalopathy in the acute phase resemble those of a stroke. However, they are not very selective.
All parts of the brain are affected at once, the list of manifestations is as wide as possible:
- Strong headache. Covers the skull, accompanied by pulsation in time with the heartbeat. Does not go away throughout the entire period of the condition. Doesn't respond well to medications. Even powerful analgesics.
- Weakness, drowsiness. Asthenic manifestations. The opposite option also occurs. The patient rushes about, cannot find a place for himself. Restless, does not make contact. This is a so-called panic attack. It is accompanied by increased motor activity and a strong fear of death.
- Dizziness. Inability to navigate in space. The person is in a forced lying position. Any movement only makes it worse.
- Nausea and vomiting.
- Feeling of ringing and buzzing in the head and ears. A typical sign of a jump in blood pressure. Although, if the patient also has a serious illness, the manifestation may not be so noticeable.
- Darkening in the eyes, flickering of flies and bright flashing dots, spots in the field of vision. Visual manifestations are caused by irritation of the occipital lobe of the brain.
- Auditory hallucinations. Also, loss of the ability to perceive noise stimuli from one or both sides at once. Sign of damage to the temporal areas. At the same time, memory problems are possible for an identical reason.
- Cramps. Epileptic seizures.
Paresis and paralysis are not typical. This is more likely a manifestation of a full-fledged stroke.
Therefore, with the development of more serious signs, a revision of the possible diagnosis and urgent differentiation of various similar conditions is required.
Signs of a pre-stroke condition are described in detail in this article.
Forms of the disease
Taking into account the nature of the course, symptoms, and anatomical damage, experts have identified the following forms of hypertensive encephalopathy:
- Subcortical arteriosclerotic.
- Multi-infarction.
Subcortical arteriosclerotic encephalopathy tends to manifest itself between the ages of 55 and 70, when the atherosclerotic process reaches high activity. The patient is concerned about the following signs:
- slowing down the pace of movements;
- memory loss;
- speech problems;
- inability to walk independently;
- orientation disorder;
- loss of appetite, vomiting;
- dysfunction of the pelvic organs;
- inability to concentrate;
- apathy, lack of emotions.
But most often doctors hear complaints about:
- hand tremors;
- headache;
- insomnia;
- swallowing disorder.
Lack of therapy is dangerous due to the development of mental retardation (dementia) after 5–10 years. Phases of improvement and stabilization of the condition are periodically observed. Various areas of the white matter of the brain are affected. Lacunar infarctions are observed in the optic thalamus, cerebellum, and pons. There is also swelling of the brain tissue.
The course of multi-infarct encephalopathy is more favorable. Patients do not experience complete dementia. Patients with this form of pathology complain of:
- difficulty speaking;
- swallowing disorder (variable);
- visual impairment, hearing impairment;
- muscle cramps;
- inability to perform movements with the hands;
- numbness of different parts of the body;
- weakness of the muscles of the arms and legs;
- headaches, dizziness.
The difference from subcortical encephalopathy is the presence of multiple areas of infarction at different depths of the intracerebral arteries. After such lesions, cavities and multiple cysts with a diameter of 0.1 - 1.5 cm are formed. At the same time, doctors record the most predisposing conditions for hemorrhagic stroke.
Please note: Hypertension is considered the most common disease of the cardiovascular system (it affects about 20 - 30% of adults. With age, the percentage of patients increases, approaching 50 - 65%).
Causes
Encephalopathy of the hypertensive type develops as a result of a regular or constant increase in blood pressure. This has already been said.
But what causes the change in blood pressure itself in the long term?
- In women, gestosis is a common option. Late complication of pregnancy. Pre- and eclampsia. These are emergency conditions.
- Discontinuation of antihypertensive medications. Also a sharp transition to other means. May cause the opposite effect or withdrawal syndrome. It is accompanied by a multiple increase in the intensity of the symptoms of the disease that is intended to be kept in check.
- Kidney pathologies. So-called secondary arterial hypertension occurs.
- The primary form (essential) is caused by the actual problems of the heart and blood vessels. Without correction, even a level of 150/90 mmHg increases the likelihood of hypertensive encephalopathy by almost 35%.
- Endocrine disorders. In particular, adrenal dysfunction, such as hypercortisolism. Or the formation of a hormonally active tumor in the structure - pheochromocytoma.
- Alcohol abuse and constant smoking also have an impact. Consumers of tobacco products with a decent amount of experience risk many times more. Caffeine does not contribute to cardiovascular health. Atherosclerosis is another significant factor in the development of hypertensive encephalopathy.
Correcting the root cause will allow you to cope with the problem much faster and with better effect than dealing with symptoms.
Diagnosis of hypertensive encephalopathy
Diagnosis of this disease is carried out on the basis of the disease history, patient complaints, and general symptoms. The results of analyzes and studies are also taken into account. The difficulty of diagnosis may lie in the fact that the signs of encephalopathy are quite similar to the clinical picture of many other pathologies: strokes, brain tumors and some other diseases.
examinations need to be carried out :
- MRI/CT helps determine cerebral edema;
- urine and blood tests (general and advanced);
- lumbar puncture;
- echocardiography (to determine the condition of the left ventricle);
- electroencephalography (to determine epileptic brain activity).
For diagnosis, the help of other doctors may be necessary: therapist, cardiologist, endocrinologist, nephrologist. They will be able to point out pathologies in other organs as a result of hypertension.
Diagnostics
The examination is carried out under the supervision of a cardiologist. You may also need the help of a neurologist and a vascular surgeon. The process under consideration is interdisciplinary.
An approximate list of methods:
- Oral interview with medical history. It is not always possible. If a person is in serious condition, you need to act quickly. Only after first aid has been provided can an in-depth examination of the patient be carried out.
- Blood pressure measurement. Indicators are usually extremely high or significantly higher than normal. What can be considered additional evidence in favor of hypertensive encephalopathy.
- Daily monitoring. Allows you to evaluate the dynamics of blood pressure and heart rate within 24 hours.
- Electroencephalography. It is carried out with the aim of studying brain rhythms and the activity of different parts of cerebral structures.
- ECG, ECHO. Methods for assessing the heart. Organic and functional disorders are identified.
- MRI if necessary. Used to identify changes in cerebral structures.
- Blood tests: hormones, general, sugar, biochemistry and others. Full laboratory evaluation.
Usually this is enough. If the need arises, other methods are prescribed.
Treatment
Therapy is carried out in a hospital setting. As soon as hypertensive encephalopathy is detected, a group of pharmaceuticals is prescribed.
The basis of treatment is the use of drugs:
- Cerebrovascular. In order to restore cerebral blood flow. Piracetam, Actovegin. Duration of use may be indefinite. Because often the cause of the disease is chronic and cannot be completely corrected.
- Nootropics. They accelerate metabolic processes, which reduces the need for oxygen and improves brain function. Phenibut, Glycine and analogues.
- Antihypertensive. Means for normalizing blood pressure. For urgent help, use Kapoten and other similar ones. But they have a pronounced effect, so the dosage must be selected carefully so as not to provoke a sharp drop in blood pressure.
A too rapid decrease will lead to a critical lack of oxygen supply to nerve tissues. Possible stroke.
The safe rate of normalization is no more than 15-20% within an hour of the initial value.
For long-term use, beta blockers (Anaprilin), calcium antagonists (Verapamil, Diltiazem) are indicated.
- Diuretics. Diuretics. Furosemide, Torasemide, others if necessary.
- Antispasmodics. They relieve vasoconstriction. Papaverine or Dibazol. Both medications are powerful. They are used by ambulance teams or doctors in hospital settings. Independent use strictly with the prescription of specialists.
- Sedatives. Not always. Only when necessary. Tranquilizers are addictive and depress the nervous system too much, which can be dangerous.
- Anticonvulsants. If there is such a need.
After recovery from the acute condition and compensation, you need to undergo a rehabilitation course.
It is mandatory for the patient to give up smoking, alcohol, and the unauthorized use of any medications, and limit the consumption of salt (up to 7 grams) and sugar. Eliminate fatty and fried foods from the diet in principle.
It would also be a good idea to optimize your physical activity. Walking or exercise therapy are suitable. Each stage of recovery must be coordinated with a doctor.
Regular examinations by specialists are also indicated in the future. At least a neurologist and cardiologist. Every 3-6 months.
Prevention
To treat DEP, prevent its occurrence and transition to more severe stages, it is recommended to lead a healthy lifestyle. The patient is advised to give up alcohol and smoking. It is necessary to exclude semi-finished products and fried foods from the diet, replace fatty meat with lean meat, eat more vegetables, fruits, and lean sea fish. It is recommended to control your weight, walk, play sports, taking into account your general condition and age.
It is important to provide yourself with normal rest, sleep at least eight hours a day. Take vitamins as needed.