Hypercapnia
(Greek hyper- + kapnos smoke) - increased carbon dioxide tension in arterial blood and body tissues.
The normal carbon dioxide tension in arterial blood in humans, referred to as “normocapnia,” is 35–45 mm Hg. Art.
The condition of Hypercapnia can be caused by exogenous and endogenous causes. Hypercapnia of exogenous origin occurs when inhaling air containing an increased amount of carbon dioxide (see). This may be due to staying in small isolated rooms, in mines, wells, in submarines, spaceship cabins and autonomous diving and space suits in the event of a malfunction of the atmosphere regeneration system, as well as during certain medical interventions, for example, in the event of a malfunction of the anesthesia breathing apparatus or when inhaling carbogen. Hypercapnia can occur under conditions of artificial circulation with insufficient removal of carbon dioxide, etc.
Hypercapnia of endogenous origin is observed in various pathological conditions accompanied by insufficiency of external respiration, impaired gas exchange (see), and is always combined with hypoxia (see).
Reasons for the development of hypercapnia
Excess carbon dioxide in the blood can be caused by external and internal factors. The first group includes:
- inhalation of air with a high content of carbon dioxide (closed isolated rooms, stay in mines, autonomous diving suits);
- violation of the regime during artificial ventilation;
- industries with high air temperatures - bakers, steelworkers;
- deep sea diving;
- being on fire.
Deep dive
Internal causes of hypercapnia are most often associated with lung diseases:
- penetration of a foreign body into the trachea, bronchial branches;
- spasm of the larynx;
- attack of bronchial asthma;
- increased secretion of sputum during bronchitis;
- pneumonia;
- chest injury;
- extensive lung surgery;
- tuberculosis;
- compaction of lung tissue due to occupational diseases (dust bronchitis, pneumoconiosis), pneumosclerosis.
Pneumonia
Extrapulmonary internal causes include respiratory depression under the influence of drugs and general anesthesia. Hypercapnia occurs with traumatic brain injury, stroke, intracerebral tumor. Respiratory failure can also provoke paralysis of the respiratory muscles during botulism, myasthenia gravis, tetanus and polio, and massive administration of muscle relaxants during surgical operations.
Secondary respiratory disorders occur with massive bleeding, a drop in blood pressure, shock, pulmonary embolism, and impaired systemic and pulmonary circulation.
We recommend reading the article on hypoxemia and hypoxia. From it you will learn about the causes of hypoxemia, classification of pathology, symptoms, diagnosis and treatment of this disease. Read more about the treatment of pulmonary hypertension here.
Causes and risk factors
The following conditions lead to the development of hypercapnia:
- pulmonary hypoventilation, accompanied by impaired gas exchange in the alveoli (the final vesicular structures of the lungs) and developing due to respiratory diseases (obstruction, inflammation, trauma, foreign objects, operations);
- impaired respiratory function due to depression of the respiratory center due to brain injuries, neoplasms, cerebral edema, poisoning with certain medications - morphine derivatives, barbiturates, anesthetics and others;
- inability of the chest to carry out full respiratory movements.
Hyperventilation as a “provoker” of hypercapnia
Separately, we should highlight hyperventilation of the lungs, which is the opposite of hypoventilation and develops with intense breathing, during which the body is oversaturated with oxygen. Often this condition subsequently leads to an increase in the amount of carbon dioxide in the tissues and blood. This happens, for example, during diving (deep diving), when a person in front of him actively and quickly breathes, trying to saturate his lungs with oxygen, but does it incorrectly.
During neurological hyperventilation (for example, during panic attacks), which provokes frequent but shallow breathing in the patient, poisoning can also occur - first with excess oxygen, then with carbon dioxide. The fact is that during superficial inhalations and exhalations, carbon dioxide is not completely removed from the lungs, accumulating in them. For this reason, experienced runners, hunters, and special forces soldiers maintain a breathing rhythm in which the exhalation is 2 or 3 times longer than the inhalation. In this case, the person completely frees the lungs of carbon dioxide, but does not provoke hyperventilation.
Endogenous factors
The causative factors causing the occurrence of endogenous hypercapnia include the following diseases and pathological conditions:
- respiratory diseases: pneumonia, asthma, emphysema, pneumosclerosis, airway obstruction;
- chest injuries, including rib fractures, arthritis of the rib joints;
- spinal deformity (scoliosis, kyphosis);
- tuberculous spondylitis, previous rickets;
- extreme obesity (Pickwickian syndrome);
- congenital defects of the osteochondral apparatus;
- limited mobility of the chest due to muscular dystrophy and pain due to intercostal neuralgia;
- damage and damage to the structures of the brain and spinal cord - strokes, encephalitis, trauma, tumor, poliomyelitis;
- myasthenia gravis (neuromuscular genetic disease);
- acidosis, metabolic alkalosis;
- atherosclerosis;
- epileptic seizures;
- apnea (sudden uncontrolled stop of breathing).
Exogenous factors
External (exogenous) causes of hypercapnia are:
- professional activities associated with frequent inhalation of carbon monoxide or prolonged breath holding (divers, firefighters, bakers, miners, foundry workers);
- heavy physical activity in conditions of carbon dioxide accumulation;
- prolonged stay in stuffy rooms, smoking, including passive smoking;
- long stay in closed and sealed spaces (wells, mines, submarines, space suits, closed garages), where carbon dioxide accumulates;
- improper operation of furnaces and boilers;
- damage by phosgene, ammonia, hydrochloric, sulfuric acid;
- poisoning with anticholinesterase drugs;
- technical problems in breathing equipment during surgical interventions when the patient is under anesthesia.
Diving work in a sealed diving suit is a warning against professional hypercapnia
Effect on the body
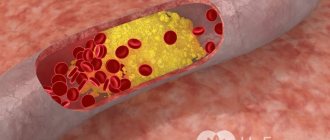
The main consequence of excess carbon dioxide is acidosis of the blood. At the cellular level, the movement of ions in membranes is disrupted - chlorine passes into red blood cells, and potassium leaves them into the blood plasma. The ability of hemoglobin to attach oxygen decreases, and therefore its content in the blood decreases (hypoxemia).
The consequences of hypercapnia include:
- activation of breathing (after an increase to 70 mm Hg - depression);
- disruption of the penetration of oxygen through the alveoli even with an increased concentration in the air;
- an increase in tissue oxygen consumption and then a decrease;
- expansion of systemic and peripheral vessels;
- increased pressure in the pulmonary artery system;
- increase in intracranial pressure;
- decrease in body temperature;
- increased venous blood flow to the heart;
- an increase in cerebral and coronary circulation with subsequent inhibition of blood flow during severe hypercapnia.
Increase in intracranial pressure
Carbon dioxide has a predominantly inhibitory effect on the nervous system - the excitability and conductivity of nerve impulses decrease after a period of brief activation.
At a high concentration of carbon dioxide, a convulsive syndrome appears, and later a narcotic effect occurs.
Forecast
Mild Hypercapnia (up to 50 mm Hg) does not have a significant effect on the vital functions of the body even with prolonged exposure: from 1-2 months for people working in hermetically sealed rooms, to many years for patients suffering from chronic. respiratory failure. The tolerability and outcome of gastrointestinal tract at higher pCO2 is determined by training, the composition of the inhaled gas mixture (air or oxygen), or the presence of a disease of the cardiovascular system.
When breathing air, pCO2 increases to 70-90 mmHg. Art. causes severe hypoxia, which, with further progression of G., can cause death. Against the background of oxygen breathing, pCO2 reaches 90-120 mm Hg. Art. causes a coma requiring emergency treatment measures.
The exact period after which it is still possible to bring a person out of a comatose state is unknown; this period is shorter, the more severe the patient’s general condition. However, with timely emergency treatment it is possible to prevent death, even if the person is in a comatose state for several hours or even days.
There are known cases of a successful outcome of G. that occurred during anesthesia, with an increase in pCO2 to 160-200 mm Hg. Art.
Symptoms of pathology
Depending on the concentration of carbon dioxide in the air, a person experiences the following changes in the body:
- admixture from 1 to 3% (normally 0.04%) - after a few days the kidneys retain bicarbonate, the formation of red blood cells increases. Without loss of performance, a person can work at 1% for a month or more, at 2-3% for several days;
- after 6% the condition worsens, over 10% consciousness is impaired after 5 minutes.
Clinical signs of hypercapnia are not specific or consistent. Each person has an individual reaction to an increase in blood carbon dioxide.
Chronic forms with minor deviations from the norm are asymptomatic, since the body easily adapts to metabolic disorders. In acute poisoning, symptoms include:
- nausea, vomiting;
- headache, dizziness;
- shortness of breath even at rest;
- sweating;
- blue skin;
- visual impairment;
- depression;
- drowsiness, decreased ability to concentrate;
- stunned;
- general weakness.
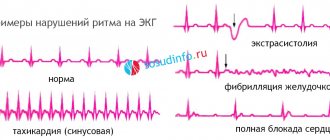
As hypercapnia increases, rapid breathing is replaced by rare breathing, and then it can completely stop. High blood pressure decreases and cardiac output decreases. Arrhythmias often occur in the form of single or paired extrasystoles. Renal blood flow does not change with a moderate increase in carbon dioxide in the blood; as poisoning progresses, the amount of urine excreted decreases (oliguria).
Clinical manifestations of hypocapnia
Symptoms of low levels of carbon dioxide in the blood are varied and nonspecific; according to some authors, one patient can demonstrate up to 80 symptoms, which can mislead not only the average person, but also the doctor. For ease of perception, the manifestations of hypocapnia can be divided into complexes of manifestations from organs and systems:
- From the respiratory side: a feeling of compression of the chest outside or inside, rapid breathing (tachypnea), frequent deep and quick sighs, yawning, coughing.
- From the cardiovascular system: tachycardia, palpitations, a feeling of the heart “jumping out”, various types of thoracolgia (chest pain).
- From the central nervous system and blood vessels: collapse (fainting), dizziness, instability in an upright position, a feeling of loss of control over oneself, the unreality of what is happening, disorientation, absent-mindedness.
- From the peripheral nervous system and blood vessels: paresthesia, tingling sensations, numbness, “coldness” in the face, ears, limbs, fingers.
- Digestive organs: swallowing air, belching, feeling of a full stomach, flatulence, xerostomia (“dry mouth”), pain in the upper abdomen.
- Musculoskeletal system: pain in muscles and joints, trembling of hands, twitching of small and large muscles, spasms of the hands (obstetrician's hand) and feet (feet turned inward), local and even general cramps.
- Excretory system: polyuria with a shift in urine reaction towards alkalization, dehydration.
- Neuropsychic state: anxiety, restlessness, fear, overexcitation, drowsiness and apathy are less common.
- General manifestations: nervousness, fatigue, sleep disturbances, low-grade fever, decreased performance.
In severe cases of hypocapnia, which can occur with improper mechanical ventilation or hyperbaric oxygen therapy, coma may occur due to metabolic dysfunction of the respiratory center.
Stages
An increase in carbon dioxide concentration and an increase in acidosis is characterized by a staged course.
| Stages of hypercapnia | Symptoms |
| First stage | Difficulty breathing occurs periodically, pressure increases simultaneously with an increase in hypercapnia, sweat production increases, urination is disrupted, apathy or aggressiveness, agitation are noted, and insomnia appears. At this stage, complete recovery is possible if the cause of the pathology is eliminated. |
| Second stage | Breathing becomes rare and shallow, mucus secretion in the bronchi increases, there is intense sweating, arterial hypertension, right ventricular failure, attacks of aggression or delirium are possible, and coma gradually develops. Oxygen therapy partially eliminates cyanosis. Urgent resuscitation is usually successful |
| Hypercapnic coma (third stage) | There are no reflexes, rare breathing, respiratory acidosis, oxygen starvation of tissues (hypoxia). With rapid development, blood circulation is disrupted, since the combination of hypercapnia and hypoxia is toxic for the myocardium |
| Terminal stage | Stoppage of blood circulation, respiratory movements, dilation of the pupil, without intensive care - fatal. Effective resuscitation at this stage is not always possible. |
Possible consequences
Hypercapnia can either lead to the development of serious complications or go unnoticed by the victim. It all depends on the severity of the disease and treatment. Consequences may include respiratory failure in newborns or unborn children if the pregnant woman suffered from respiratory acidosis. High levels of CO2 negatively affect the baby’s not fully developed central nervous system, especially the cerebral cortex, which can provoke:
- delayed mental and psychomotor development;
- cerebral palsy;
- epilepsy and other complications.
Types of hypercapnia
Depending on the mechanism of development and duration of action of the damaging factor, several types of hypercapnia have been identified.
Alveolar
The most common form of hypercapnia. It occurs when ventilation in the alveoli of the lungs decreases. Occurs with injuries, obstruction of the airways, decreased functioning of the lung tissue due to inflammation, emphysema, pneumosclerosis, edema or congestion in the lungs. It is also caused by respiratory depression due to anesthesia or drug, drug intoxication, or brain damage.
Permissive
Such hypercapnia is created deliberately during artificial pulmonary ventilation (ALV) in order to prevent excessive stretching of the lungs and limit the range of movement of the affected areas. With it, the level of carbon dioxide (35-45 mm Hg is normal) is increased to 50-120 units.
Tolerable (permissive) hypercapnia is used in resuscitation practice for adults and newborns, since a controlled increase in carbon dioxide causes the following reactions in the body:
- stimulates the expansion of the bronchi;
- leads to the opening of supplemented ventilation pathways;
- promotes the formation of a surfactant - pulmonary surfactant, which prevents the alveoli from collapsing (not developed in premature babies);
- improves the penetration of oxygen into the blood.
Permissive hypercapnia
Permissive hypercapnia is contraindicated in cases of decompensated acidosis, high intracranial pressure, severe arterial hypertension and hypotension, acute renal failure and sepsis.
Features of hypercapnia in children
In children, hypercapnia develops much faster and is more severe than in adults. This is explained by the anatomical and physiological characteristics of the child’s body, such as:
- narrowness of the respiratory passages - accumulations of mucus and swelling of the mucous membrane against the background of even minor inflammation can lead to a violation of their free patency;
- underdevelopment and weakness of the respiratory muscles;
- the ribs extend from the sternum almost at a right angle, which limits the excursion (mobility) of the chest in the act of breathing.
Acute and chronic
Acute development of hypercapnia is observed when breathing suddenly stops. It can be caused by suffocation, drowning, compression of the chest due to compression injury, electric shock, malfunction of ventilation systems in closed mines, on submarines, or malfunction of a ventilator. In such cases, symptoms increase over the course of minutes and, in the absence of emergency assistance, the patient falls into a coma with a fatal outcome.
In case of chronic disorder, excess carbon dioxide can be compensated by the body by increasing respiration and retaining bicarbonates by the kidneys. Such forms can be latent, but with continued exposure to a damaging factor they can become acute with pronounced clinical symptoms.
What is the difference between hypercapnia and hypocapnia?
Low carbon dioxide levels in the blood are called hypocapnia. Such conditions lead in mild cases to dizziness, and in more severe cases to loss of consciousness. Occurs with panic, hysterical reactions, which are accompanied by frequent and deep breathing. Forced inhalations occur when diving or inflating swimming mattresses. Low physical activity and age-related changes can also cause hypocapnia.
Chronic increased ventilation of the lungs (hyperventilation syndrome) accompanies mental disorders and brain damage. Manifested by headache and heart pain, tachycardia, indigestion and abdominal pain. Brain fog or fainting may occur.
Diagnosis of the condition
Hypercapnia can be suspected based on the patient's complaints, as well as on the basis of the circumstances of their occurrence. The most reliable criterion is the determination of blood gas composition and acid-base balance. In this case, respiratory (respiratory) acidosis is detected in a decompensated form. In the future, its compensation occurs due to metabolic alkalization of the blood with the participation of the hemoglobin buffer, the work of the kidneys and lungs.
To determine the causes of the development and course of pathology, patients are prescribed:
- general blood test, electrolyte composition;
- spirography;
- X-ray examination of the chest organs;
- capnography using an exhaled air carbon dioxide analyzer.
Operating principle of the exhaled air carbon dioxide analyzer
Treatment of hypercapnia
First of all, the patient needs to provide an influx of fresh air, remove it from an atmosphere with a high carbon dioxide content, and remove obstacles to breathing. In case of coma, an artificial lung ventilation device is urgently connected. Oxygen therapy is mainly used for external factors causing hypercapnia.
Internal causes require treatment of the disease that caused the disturbance in the blood gas composition. Oxygen is used with great caution, especially in case of respiratory depression due to drug poisoning, or during exacerbation of respiratory failure due to lung diseases. Oxygen therapy in such patients worsens the condition, as it further suppresses the activity of the respiratory center.
Features of hypercapnia in pregnant women
In pregnant women, especially in the third trimester, any breathing disorders can cause rapidly developing hypercapnia, which is associated with the following features:
- oxygen consumption during pregnancy increases by 20-23%;
- the type of breathing changes to the chest, the abdominal muscles cease to play the role of auxiliary respiratory muscles;
- there is a high standing of the diaphragm caused by the growing uterus, which prevents deepening of inspiration when the need arises.
In late pregnancy, hypercapnia can develop rapidly
Prevention
It is possible to prevent external hypercapnia by following safety rules when working in sealed rooms, scuba diving, ensuring sufficient absorption of carbon dioxide by filters, and also monitoring the serviceability of anesthesia and mechanical ventilation devices.
To prevent chronic forms of pathology, it is recommended:
- frequent exposure to fresh air;
- ventilation of industrial and residential premises;
- treatment of respiratory diseases;
- daily therapeutic and breathing exercises;
- increasing the body's fitness through swimming, running, walking.
We recommend reading the article on pulse oximetry. From it you will learn about the principle of the non-invasive method, what the sensor is, what determines the accuracy of the measurement, as well as about normal and abnormal indicators. And here is more information about the polarizing mixture.
Hypercapnia occurs due to lung diseases, respiratory depression, or increased concentrations of carbon dioxide in the inhaled air. The chronic form may be asymptomatic, but in acute and severe poisoning it manifests itself as a coma. Permissive hypercapnia is used for therapeutic purposes.
To make a diagnosis, the blood gas composition is examined. During treatment, oxygen is used with caution; the main efforts are aimed at eliminating the cause of the increase in carbon dioxide in the blood.