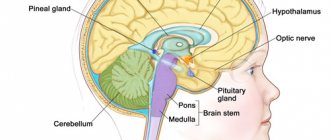
Features of neoplasms
A cyst in the head of a newborn can be diagnosed in the womb. Neoplasms can be localized in different parts of the brain and vary in size. Sometimes several compactions are observed. As a rule, cysts formed in utero go away on their own in nine out of ten cases and do not require treatment.
A certain danger is fraught with pathology diagnosed after the birth of the child. Such a neoplasm, for example, a ventricular cyst, is fraught with compression of certain parts of the brain in an infant and disruption of its functioning, which is often observed with a large size of the seal. The disease must be treated, and treatment begins from the first days of the baby’s life.
Symptoms of a cyst are:
- headache in an infant;
- impaired response to stimuli;
- numbness and short-term paralysis of the limbs;
- visual disturbances;
- anxiety, insomnia in an infant.
Symptoms largely depend on the location and size of the tumor.
As a rule, a cyst is detected using an ultrasound examination, which all newborns undergo in the first hours of life. If a neoplasm is detected, you must contact a neurologist. The specialist conducts a detailed examination, as a result of which the location and size of the compaction is determined, and then prescribes treatment. In the future, the child needs regular examinations (every 4 weeks), which will allow time to notice an increase in the size of the lump and adjust the treatment.
Treatment
The choice of therapeutic interventions depends on several factors. In this case, it is important to take into account the type of cystic formation, its size and location.
On this topic
- central nervous system
What threatens a cyst in the head?
- Olga Vladimirovna Khazova
- February 28, 2020
If the disease is diagnosed in utero, therapy is not required. In this case, observational tactics are chosen that allow constant monitoring of the state of the newborn’s brain. As a rule, in such situations, tumors undergo spontaneous resorption.
If there is a need to remove a tumor, then experts give preference to two methods of surgical intervention.
Radical
In this case, the skull is trepanned and the cyst is completely excised. The operation is one of the most traumatic and poses a serious threat to the health of the baby.
It is for this reason that it is used in extremely serious conditions, when no positive result is observed from the use of other treatment methods.
Palliative
Includes two methods of therapy.
Bypass surgery
The technique involves inserting a shunt into the cystic cavity and removing the contents from it. This procedure is not dangerous. However, it does not exclude the risk of infection entering the brain, against which inflammatory processes may begin to develop.
Endoscopy
Several small punctures are made in the skull. Extraction of the tumor formation is carried out using an endoscope. This type of surgery is less traumatic, and the recovery period does not take much time.
After surgery, it is rare for the baby’s condition to become complicated, but only if the procedure is carried out by a highly qualified specialist.
Symptoms and signs of benign neoplasm in infants
Symptoms of the disease largely depend on where the lump is located and its size. The nature of the cyst also plays an important role. Symptoms are determined by additional factors of complications due to the tumor, which include suppuration at the location of the compaction, the risk of transforming a benign tumor into a malignant one, as well as the presence of an inflammatory process.
It should be noted that small cysts are often asymptomatic. There is a high probability of complete resorption of a small cyst without treatment. However, it is imperative to conduct a detailed examination (ultrasound, MRI) and repeat it regularly, since the formation may increase in size.
In some cases, even a small cyst provokes the appearance of neurological symptoms, which include:
- infant sleep disorders;
- tremor of the limbs;
- increase in size of the fontanelle;
- muscle spasms;
- convulsions;
- mental development disorders;
- reflex disorders.
The situation is aggravated in the presence of an inflammatory process or suppuration. In this case, symptoms of intoxication of the body are added and an increase in body temperature is observed.
An increase in size of the cyst leads to a mechanical effect on the brain of a small patient, resulting in an increased risk of developing serious complications, including stroke.
Small cysts can be successfully treated with drug therapy. Complicated or multiple large cysts require surgical intervention. If the problem is detected in a timely manner and treatment is started on time, the disease is successfully cured and goes away without a trace.
NSG cyst - Protocol
The brain structures are formed correctly and asymmetrically. The furrows and convolutions are pronounced. In the projection of the lobe, an anechoic formation is visualized - mm, communicating with the cavity of the lateral ventricle.
The lateral ventricles are asymmetrically dilated. Anterior horns of the lateral ventricles: on the right - 3 mm; on the left - 3 mm (norm up to 5 mm). Body of the lateral ventricle – on the right – 3 mm; on the left - 3 mm (norm up to 5 mm). Temporal horns are not detectable (normal). Atrium - filled with choroid plexuses (normal up to 12-16 mm). Occipital horns are not detected (normal).
Periventricular tissues and areas of the basal ganglia have increased echogenicity.
CONCLUSION: cyst in projection
Causes of neoplasms
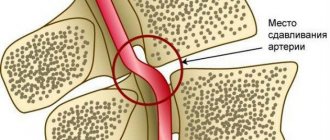
The cyst is formed against the background of degeneration of brain tissue and its subsequent death. It is in these areas that a dense spherical formation filled with liquid is formed. Among the causes of brain cysts in infants:
- trauma during passage through the birth canal or during complicated childbirth;
- pathologies of the central nervous system;
- inflammatory brain diseases (encephalitis or meningitis);
- action of the herpes virus;
- oxygen starvation of the brain;
- lack of nutrients, causing cerebrovascular accidents.
Under the influence of some negative factors, an existing cyst may enlarge or grow. As a rule, this occurs against the background of increased intracranial pressure in the infant. A concussion, head injury, or infection can also cause the tumor to increase in size.
Neurosonography is normal - Protocol
The interhemispheric gap is 1 mm (the norm is up to 4 mm).
Subarachnoid spaces - 2 mm (normal is up to 3 mm).
The cavity of the transparent septum: not expanded.
Anterior horns of the lateral ventricles: on the right - 3 mm; on the left - 3 mm (norm up to 5 mm). Body of the lateral ventricle – on the right – 3 mm; on the left - 3 mm (norm up to 5 mm). Temporal horns are not detectable (normal). Atrium - filled with choroid plexuses (normal up to 12-16 mm). Occipital horns are not detected (normal).
The third ventricle is 2 mm (normal is up to 4 mm).
The fourth ventricle is triangular in shape in the sagittal plane, not dilated (normal is up to 8 mm).
Choroid plexus - 10 mm, with smooth and clear contours.
The brain parenchyma is of medium echogenicity. The pattern of convolutions and grooves is distinct. The echogenicity of the subcortical zones is not changed. Caudothalamic notches are not changed. Periventricular areas have normal echogenicity.
The structures of the posterior cranial fossa are differentiated. Large tank 5 mm (norm up to 12 mm).
Stem structures are of normal echogenicity.
In the CD mode, the arteries of the circle of Willis are determined up to branches of the 4th-5th order, zones of hypo- and hypervascularization are not identified, the course of the vessels is not changed. Indicators of velocities and peripheral resistance in the arteries of the brain are not changed: ACA IR - 0.72 (normal up to 0.72). Venous blood flow is not changed, the maximum speed in the vein of Galen is 7 cm/s (the norm is up to 10 cm/s).
CONCLUSION: The brain parenchyma is not changed. The intrathecal spaces and ventricles are not dilated. Cerebral blood flow parameters are normal.
Types of neoplasms
In most cases, doctors have to deal with four types of benign tumors in the brain of newborns:
- choroid plexus cyst;
- intracerebral or subependymal cyst;
- arachnoid type cyst;
- benign neoplasm acquired as a result of trauma.
The first type develops due to the penetration of the herpes virus into the body in newborns. A subependymal or intracerebral cyst in a newborn develops due to lack of oxygen and subsequent death of brain tissue.
Arachnoid neoplasms arise between the cerebral spaces. If excessive pressure is applied to the baby while passing through the birth canal, there is a risk of developing a traumatic cyst. Also, this type of neoplasm may appear as a result of cerebral bleeding or, conversely, a lack of blood supply to the brain.
Relationship with other pathologies of intrauterine development. Does she really exist?
In medical literary sources, you can find information that there is some connection between the presence of choroid plexus cysts and some congenital pathology caused by a genetic mutation. Moreover, the localization of the cystic cavity on the right, left or both sides at the same time has absolutely no significance. But here it is very important to remember that it is NOT a cyst that provokes developmental anomalies, but on the contrary - a violation of intrauterine development contributes to the formation of vascular cysts , therefore the connection between them is limited only by the presence or increase in the number of choroid plexus cysts and that’s all. Nothing more. Such genetic defects, when a cystic cavity is diagnosed more often than usual, include trisomy 18, known as Edwards syndrome (non-disjunction of the 18th pair and the addition of another chromosome 18 to it, so instead of the normal two, there are 3 of them, and the entire genotype of such an embryo is represented by 47 chromosomes). By the way, it is believed that trisomy 21 (Down's disease) has a much smaller effect on the increase in the incidence of choroid plexus cysts than trisomy 18.
In addition, it is important to note that in the case of other pathology, the primary role does not belong to the cyst, but to the deviations that it accompanies, for example, the same Edwards syndrome, so its significance here is reduced to zero.
Thus, a choroid plexus cyst, no matter right or left, is single or represented by several small formations:
- Equally safe;
- Doesn't play any role;
- Does not participate in any important processes;
- Incapable of growing and being reborn.
Pregnant women should know about it so as not to be afraid and not to be confused with other cystic formations that have similar names, but a completely different genesis and location.
Bilateral choroid plexus cysts on MRI images
Cyst and viral diseases
The most common is a cyst or neoplasm of the choroid plexus in a newborn baby. This form appears due to the action of a virus, such as herpes. The disease can be caused by toxoplasmosis.
Often the disease develops during pregnancy, in the first trimester. There are no nerve endings in the choroid plexuses, but they are directly involved in the blood supply to the brain. As a rule, with the early development of a cyst, it completely resolves on its own before delivery.
This type of neoplasm is considered safe. Cysts do not affect the child’s mental abilities and do not cause neurological symptoms; children subsequently develop normally.
To determine the pathology, an intrauterine ultrasound examination of the fetus is performed. Most often, treatment is not required and, as the fetus’s nervous system develops, the tumors resolve.
Rarely, this type of cyst occurs in newborns. Despite the safety of the neoplasm itself, a detailed examination and constant monitoring of the size of the compaction are required. As the cyst enlarges, there is a high risk of developing diseases associated with mechanical compression of an area of the brain.
As a rule, the prognosis is favorable both for the intrauterine formation of compactions and for the diagnosis of cysts in newborn infants. Competent treatment allows you to completely get rid of the disease; it goes away without a trace during the first 6-10 months of life.
NSG norms and protocols
The article is under development.
Normally, the interhemispheric fissure has a strictly median position; the width in a newborn of 30-34 weeks of gestation is 2.8 ± 0.2 mm, in older infants it is 2.0 ± 0.1 mm. Separate assessment of the interhemispheric fissure and the falciform process is possible only in cases of fluid accumulation along the fissure and in cases of atrophy of the brain substance.
An arched deformity usually indicates a space-occupying process or fluid accumulation in the intrathecal space on one side. Displacement of the interhemispheric fissure and falciform process without deformation usually indicates hypoplasia of the cerebral hemisphere, which is often combined with changes in the facial skull.
Assessing the size of the various parts of the ventricular system is necessary to exclude ventricular enlargement (ventriculomegaly). The most stable dimensions are the body (depth no more than 4 mm) and its anterior horn (depth 1-2 mm); the occipital horn is often asymmetrical, variable in depth and size; the dimensions of the 3rd ventricle are 2-4 mm. Assessing the 4th ventricle is difficult, so attention is paid to its shape and structure, which can change significantly with abnormalities in brain development.
Using NSG, you can identify the level of occlusion (aqueduct - 60%, foramen of Monroe - 25%, foramina of Luschka and Magendie 10%, subarachnoid space - 5%).
- Initial signs of expansion of the ventricular system, manifested by an increase in the depth of the bodies of the lateral ventricles to 5-8 mm, the disappearance of lateral curvatures and the appearance of a rounded shape of the lateral ventricles; The 3rd and 4th ventricles are not dilated;
- Moderate ventriculomegaly - body depth up to 9 mm, slight uniform expansion of all parts of the lateral ventricles; The 3rd ventricle is enlarged to 4-6 mm, the 4th ventricle is usually normal;
- Severe ventriculomegaly - the depth of the bodies is more than 9 mm, the 3rd ventricle is dilated - interthalamic fusion in its cavity is visible, the 4th ventricle and the brain cisterns are dilated.
The average size of the cistern magna in a full-term newborn is 4-5 mm; In premature babies, the size of the cistern magna varies depending on the gestational age and can reach 10 mm or more.
The quadrigeminal cistern is usually represented by a hyperechoic line between the 3rd ventricle and the cerebellar vermis, its thickness is no more than 3 mm. It can increase with subarachnoid hemorrhages and with cysts of this cistern, which are difficult to differentiate from an arachnoid cyst in this area.
The dimensions of the cavity of the transparent septum can vary from 2 to 10 mm.
Intracerebral neoplasm
A subependymal cyst in a newborn develops as a result of oxygen starvation of brain tissue, which provokes the death of some areas and the development of a cyst in place of the dead tissue.
This form of the disease does not pose a threat to mental retardation or dementia in the child. However, the pathology causes a number of serious neurological disorders. In most cases, intracerebral formation resolves on its own. However, any changes in tumor size must be carefully monitored until it resolves.
Doctors often prescribe medication. If therapy is started in a timely manner, there is no risk to health or further life activity; the pathology is completely cured within a few months.
Arachnoid neoplasm
This type of disease occurs no more often than in 5% of cases of cyst formation in infants. This disease is divided into primary formation (congenital pathology) and secondary (due to inflammation of the brain).
The pathology causes neurological symptoms - migraines, sleep disorders, irritability. If the disease is provoked by an inflammatory process, signs of intoxication of the body are added to the symptoms - nausea and vomiting, and possibly an increase in body temperature. Treatment is usually surgical. If intervention is not carried out in time, there is a high risk of developing neurological disorders that leave an imprint on the entire future life of the baby.
NSG agenesis of the corpus callosum - Protocol
The structures are not formed correctly. The corpus callosum is absent. The interhemispheric fissure is not widened. The lateral ventricles are dilated: The grooves and convolutions extend fan-shaped from the bodies of the lateral ventricles.
The third ventricle is flask-shaped dilated (mm), pulled upward.
The fourth ventricle is elongated.
Periventricular tissues have normal echogenicity.
The choroid plexuses are deformed and not dilated.
CONCLUSION: agenesis of the corpus callosum. Dilatation of the lateral and 3rd ventricles.
Diagnosis of pathology
The examination is carried out by a neurologist. Ultrasound diagnostic methods are used for this. If the presence of a benign tumor is confirmed by examination, the child is referred for consultation to a neurosurgeon, who determines the location, size and type of tumor. To get an accurate picture, it is necessary to measure the baby's blood pressure, as well as check the condition of the blood vessels using Doppler ultrasound.
To determine the cause of the formation of the seal, the blood is also examined for infection, inflammation or an autoimmune response of the body.
Typically, the first brain examination is done in utero. Then an ultrasound examination is required upon reaching one month of age.
Brain examinations are mandatory for premature babies, as well as for complicated births or congenital pathologies.
Possible complications
The cyst can increase in size without causing discomfort to the baby. As a result, during puberty, due to hormonal changes, there is a high risk of rapid tumor growth and the development of dangerous complications, including stroke.
If the formation is not treated, the following complications are possible:
- loss of vision and hearing;
- problems of the vestibular apparatus;
- impaired coordination of movements;
- convulsive syndrome;
- progressive mental retardation.
Timely detection of pathology and further treatment allows you to avoid negative consequences. As a rule, in 99% of cases, removal of the cyst or drug therapy allows you to get rid of the formation without a trace.
Neurologist ⇒ Neurological problems in a baby
Post by Nozdrina Maria » Dec 15, 2008, 4:01 pm
Post by Ketevan Meshkov » December 15, 2008, 11:40 pm
Post by Granny » May 29, 2009, 01:16 pm
Post by Ketevan Meshkov » June 02, 2009, 18:49
Post by Guest » Jun 27, 2009, 6:08 pm
Post by Ketevan Meshkov » June 28, 2009, 10:43 pm
Post by Guest » 25 Aug 2009, 01:00
Hello! My 3-month-old child had an ultrasound scan of the brain: body of the lateral ventricles VLS=13.6 VLD=13.8 Anterior horns of the ventricles S=13.2 D=13.5 Temporal horns of the ventricles S=23.01.0 D =24.01.0 Third ventricle - width 1.5 ventricular index 0.27 and 0.26 Structure of the posterior cranial fossa - located symmetrically, pathological formations are not determined interhemispheric fissure - width - 2.5 depth - 10.6 echoarchitecture brain - disturbed - deformation of the choroid plexuses, hyperechogenicity of the contours of the lateral ventricles CONCLUSION: neurosonographic signs of moderate post-hypoxic changes in the brain, dilatation of the lateral ventricles
The neurologist prescribed Pantogam syrup 1 ml 2 times a day - course 2 months, magnesium b6 1 ml 2 times a day - course 1 month, as well as electrophoresis of aminophylline and lidase according to Bourguignon (forehead-occipital), general massage + gymnastics
Please tell me how serious these ultrasound results are and whether such treatment is justified, and I also don’t understand why magnesium b6 is prescribed here. Thanks in advance for your answer
Post by Ketevan Meshkov » August 25, 2009, 01:05