The course of some diseases is complicated by pathology such as hormonal tachycardia. Whether this condition is dangerous can be found out after a full examination of the patient, when changes in certain organs and systems of the body are determined.
Tachycardia most often characterizes a symptom that appears in various diseases, mainly associated with myocardial damage. Some pathological conditions develop against the background of hormonal disorders, and in such cases, a rapid heartbeat may also occur.
Hormonal tachycardia is a clinical definition that is not recorded in ICD-10, but often develops in middle-aged people, most often in women.
Diagnosis of the disease is carried out using electrocardiography and, if detected, appropriate treatment should be prescribed. If you take timely measures to treat hormonal tachycardia, then you will not need to worry about whether this condition is dangerous, which in some cases is quite difficult for patients to tolerate.
Video Tachycardia
Description of hormonal tachycardia
Hormonal levels are an important link in the chain of all life processes. Many of them ensure human growth, development, reproduction and withering. If there is a change in the hormonal (humoral) regulation of the body, then cardiac activity is primarily affected.
The effect of certain hormones on the heart muscle (myocardium):
- Catecholamines (norepinephrine, adrenaline, dopamine) are produced by the adrenal glands and by their action have a direct effect on the heart, promoting increased cardiac activity.
- Glucagon is produced by the pancreas and has an indirect effect on the heart by increasing the frequency of contractions.
- Iodine-containing hormones are produced by the thyroid gland and, like glucagon, have an indirect effect on the heart muscle, which begins to contract more frequently.
During hormonal tachycardia, a mechanism of increased automatism of the sinus node is most often observed, while organic heart damage is diagnosed in rare cases.
Having a direct connection with various kinds of hormonal imbalances, hormonal tachycardia is most often determined by an increase in the production of hormones by the thyroid gland. Other endocrine disorders can also cause hormonal imbalance and, as a result, cause tachycardia. In particular, this is a disorder of the menstrual cycle in women, which is often accompanied by rapid heartbeat. Also, dysfunctions of the genitourinary system in men have recently become more frequent, which consequently leads to the appearance of tachycardia.
Does the heart produce hormones?
The most studied endocrine functions of heart cells are the synthesis of atrial hormone (atriopeptide), atriopeptins and relaxil. In addition, substances such as growth hormones, stress hormones, and oxytocin were also found inside cardiomyocytes.
We recommend reading the article about arrhythmia. From it you will learn about what tests to take for arrhythmia, what the test results will show. And here is more information about thyrotoxicosis and the heart.
Atrial hormone
It is synthesized by myocytes and enters the blood when the atria are stretched with a large volume of blood. This process is also affected by: the concentration of sodium, vasopressin, angiotensin 2, and high activity of the sympathetic nervous system. In other words, any factors that increase blood pressure, and, consequently, the load on the heart, contribute to the formation and entry of atrial hormone into the vessels.
Under his influence:
- the walls of blood vessels relax;
- pressure decreases;
- water from the blood passes into tissue fluid;
- sodium excretion increases almost 90 times, which is why this hormone is called natriuretic, it is much stronger than any known diuretic;
- urine volume increases;
- the formation of renin and the conversion of angiotensin to angiotensin 2 (a powerful factor in vasoconstriction) are inhibited;
- the rate of filtration in the kidneys increases;
- Aldosterone synthesis slows down.
With normal secretion of this hormone, myocardial hypertrophy and amyloid deposition in the heart are prevented, intestinal walls are relaxed, fat breakdown is stimulated and body weight is reduced. It regulates pressure in intraocular and intracranial hypertension.
The level of atrial natriuretic hormone can be a diagnostic sign - it increases with heart failure in proportion to its severity. There is research data showing a slowdown in the progression of pancreatic cancer under the influence of injections of this protein.
Atriopeptins
These hormones increase blood pressure, regulate thirst, and the desire to eat salty foods. Some of these substances, also formed in the atria, inhibit the removal of water from the body and increase the release of vasopressin. The influence of atriopeptins on the sense of smell, sleep and duration of wakefulness, memory and general excitability of the nervous system has been discovered.
Relaxin
It is similar in structure to insulin - it has two chains connected by a disulfide bridge. It is synthesized and secreted by cells of the muscular layer of the right atrium. Under the influence of the hormone, the pulse rate and blood pressure increase, and during labor it helps to move the pelvic bones apart to facilitate the advancement of the fetus.
Stress hormones
The heart's own adrenergic cells are capable of producing catecholamines, which increase contraction frequency, coronary blood flow, and energy metabolism. The main compounds found in the myocardium are norepinephrine and dopamine. They activate cardiac activity and increase the heart’s readiness for high stress.
Oxytocin
The release of this hormone increases brain functions such as the desire for knowledge, adaptation to changes in the social environment, and tolerance towards people. Oxytocin increases the tone of the uterus, the level of sexual arousal, stimulates the excretion of sodium by the kidneys, but inhibits the release of water, and helps restore muscles during aging.
Symptoms of hormonal tachycardia
During an attack, patients experience a rapid heartbeat, which is often accompanied by symptoms of autonomic disorder. This may be a headache, dizziness, a feeling of lack of air, “the heart jumping out of the chest,” or painful sensations in the cardiac region.
The normal state is characterized by a heart rate of 60 to 90 beats per minute. This indicator applies to adults; in children, depending on age, heart rate can range from 100 to 170 beats per minute.
Tachycardia that develops as a sinus tachycardia is characterized by a gradual increase in heart rate and the same ending of the attack. In complex cases, tachycardia appears not only during physical exertion, but also in a calm state, so it is important to conduct a timely examination so as not to worry about how dangerous the disease is.
Paroxysmal or ventricular tachycardia, provoked by hormonal imbalance, develops less frequently and is perceived more difficult by patients. The condition may be complicated by fainting or fainting, which may serve as additional evidence of the presence of organic heart pathology.
Heart function and work
Contractile function – rapid contractility of the heart, controls the level of hypertension.
Endocrine function - the ability to produce natriuretic factor occurs.
Information function - information is transmitted in the form of blood flow speed in the tissue with a change in its metabolism.
Blood feeds the body with the help of the heart with useful elements and oxygen. Endocrine cells (distribute cardiodilantin - hormones that enhance the work of the heart - throughout many organs) are formed in the myocardium - the heart muscle and in the atria.
There is the following function that can remove carbon dioxide and used substances from the body.
Causes of hormonal tachycardia
The pathology is directly related to an imbalance in the humoral regulation of the heart, when certain diseases cause excessive production of hormones that cause tachycardia.
Endocrine diseases causing hormonal tachycardia:
- Pheochromocytoma is a tumor of the adrenal glands, most often benign, in which tachycardia is observed in 60% of cases. Changes in the body are associated with excessive synthesis of catecholamines by the tumor.
- Thyrotoxicosis is an overactive thyroid gland, which begins to intensively produce thyroid hormones.
- Hyperparathyroidism is excessive secretion of parathyroid hormone by the parathyroid gland. The hormone creates an imbalance in calcium metabolism, which indirectly affects the cardiovascular system.
- Itsenko-Cushing syndrome - with this pathology, cortisol is produced in significant quantities, which is associated with a pituitary tumor or adrenal tumor.
- Acromegaly - when a tumor occurs in the pituitary gland, growth hormone (somatotropin) begins to be produced in excess, which leads to gigantism or enlargement of various parts of the body (lower jaw, ears, palms, feet).
With all of the above pathologies, to varying degrees, from 30% to 60%, arterial hypertension and various cardiovascular diseases are observed, including the so-called hormonal tachycardia.
There are provoking factors that cause hormonal tachycardia:
- beginning of menarche;
- pregnancy or postpartum period;
- menopause (male and female);
- taking contraceptive medications;
- hyperfunction of the gonads.
Depending on the cause, appropriate treatment is prescribed, which necessarily takes into account the characteristics of the course of the underlying disease.
Hormonal regulation of heart activity
Factors of humoral regulation are divided into two groups:
1. substances of systemic action;
2. local substances.
Systemic substances include electrolytes and hormones.
Electrolytes ( Ca ions
) have a pronounced effect on the functioning of the heart (positive inotropic effect).
With an excess of Ca, cardiac arrest may occur during systole, since there is no complete relaxation. Na ions can have a moderate stimulating effect on the activity of the heart. With an increase in their concentration, a positive bathmotropic and dromotropic effect is observed. K ions
in high concentrations have an inhibitory effect on cardiac function due to hyperpolarization. However, a slight increase in K stimulates coronary blood flow. It has now been found that with an increase in the level of K compared to Ca, a decrease in heart function occurs, and vice versa.
Hormone adrenaline
increases the strength and frequency of heart contractions, improves coronary blood flow and increases metabolic processes in the myocardium.
Thyroxine
(thyroid hormone) enhances heart function, stimulates metabolic processes, and increases the sensitivity of the myocardium to adrenaline.
Mineralocorticoids
(aldosterone) stimulate Na reabsorption and K excretion from the body.
Glucagon
increases blood glucose levels due to the breakdown of glycogen, leading to a positive inotropic effect.
Sex hormones
in relation to the activity of the heart they are synergists and enhance the work of the heart.
Substances of local action act where they are produced. These include mediators. For example, acetylcholine
shows five types of negative effects on the activity of the heart, and norepinephrine - on the contrary
.
Tissue hormones (kinins) are substances with high biological activity, but they are quickly destroyed, and therefore have a local effect.
These include bradykinin, kalidin, moderately stimulating blood vessels. However, at high concentrations they can cause a decrease in heart function. Prostaglandins,
depending on the type and concentration, can have different effects. Metabolites formed during metabolic processes improve blood flow.
Thus, humoral regulation ensures a longer adaptation of the heart’s activity to the needs of the body.
Didn't find what you were looking for? Use the search:
source
Types / photos of hormonal tachycardia
Pathology can be expressed in various forms of arrhythmia: paroxysmal tachycardia, sinus tachycardia. Paroxysmal arrhythmia is considered the least favorable, since it can lead to ventricular fibrillation and sudden cardiac arrest.
Hormonal paroxysmal tachycardia
During disorders of humoral regulation, paroxysmal tachycardia can be observed, which manifests itself as sudden attacks of palpitations. The disease can be temporary; in severe cases, paroxysms occur once a month or more often.
Paroxysmal tachycardia due to hormonal imbalance most often affects the atria, although in some cases it disrupts the normal functioning of the ventricles. The danger of this form of hormonal tachycardia is that the heart cannot provide adequate blood supply to vital organs. This in turn affects their performance.
Hormonal sinus tachycardia
The disease manifests itself in hormonal disorders several times more often than paroxysmal tachycardia. This is due to the direct influence of a number of hormones on cardiac activity. In addition, the heart itself produces hormonal substances such as prostaglandins, adenosine and histamine, which also affect the activity of the sinus node.
With sinus tachycardia, which appears against the background of hormonal disorders, a heart rate of 100 to 150 beats per minute is observed, while the attack begins and ends smoothly, and the sinus rhythm remains the leader of cardiac activity. During hormonal disorders, tachycardia of an inadequate course is observed, that is, it can remain at rest, accompanied by symptoms such as a feeling of lack of air, strong heartbeat, weakness, and dizziness.
Hormones that increase heart rate
Women have a lower risk of developing cardiovascular disease than men. But during the postmenopausal period, the risks level out. In 65-70% of cases, acquired long QT syndrome and drug-induced torsade de pointes tachyarrhythmias occur in women. It is obvious that sex hormones influence the cardiovascular system - differences in male and female ECGs were identified back in 1920.
The specific mechanisms by which hormones affect the heart are described below:
Like any steroid hormones, sex hormones are able to bind to DNA, thereby influencing the processes of cell growth and maturation.
✔Estrogen has a protective effect on the cardiovascular system (reduces apoptosis and hypertrophy of cardiomyocytes, enhances the natural antioxidant defense of the cell, causes vasodilation and reduces the level of inflammation in the vascular wall)
✔Progestogen suppresses the proliferation of smooth muscle cells of the myocardium and blood vessels
✔Supraphysiological concentrations of testosterone cause myocardial hypertrophy.
Steroid hormones have been shown to bind to ion channels on heart cells and thus affect heart rate and rhythm.
✔Physiological fluctuations in sex hormones can cause changes in the length of the QT interval in pregnant women
✔Progestogen and testosterone reduce the QT interval on the ECG
✔Estrogen and aldosterone increase the length of the QT interval on the ECG
✔Hyperaldosteronism is associated with prolongation of the QT interval on the ECG. On therapy with mineralcorticoid receptor blockers, QT returns to normal values.
Cellular organelles - mitochondria, responsible for the synthesis of energy in the form of ATP - have estrogen receptors. Estrogens are thought to have a protective modulatory effect. This is associated with different sex ratios in the incidence structure of some mitochondrial pathologies—women suffer less often.
FSH (follicle stimulating hormone) receptors have been found to be present in the myocardium. FSH concentrations are positively correlated with the length of the QT interval. For this reason, women during the ovulatory peak are more susceptible to drug-induced long QT syndrome.
In conclusion, I would like to note that this is a large and still far from covered topic. The main avenues of research are: the genomic effects of steroids, the possibility of using hormonal therapy in the acute period of coronary heart disease, and the selection of optimal hormone replacement therapy.
If you have any questions, feel free to ask the author.
Have you been struggling with HYPERTENSION for many years without success?
Head of the Institute: “You will be amazed at how easy it is to cure hypertension by taking it every day.
There are orthostatic hypotension and hypertension. Orthostatic hypotension is a common disorder of the autonomic nervous system.
This disease most often occurs in elderly patients. This disease is also characterized as a syndrome that manifests itself in various neurological and somatic diseases.
Our readers successfully use ReCardio to treat hypertension. Seeing how popular this product is, we decided to bring it to your attention. Read more here...
Orthostatic hypertension is often a manifestation of nephroptosis, in which blood pressure increases when a person is in an upright position. This disease is observed in 85% of patients suffering from nephroptosis. This is a characteristic symptom of renovascular nephrogenic hypertension.
However, in comparison with renovascular hypertension, orthostatic hypertension develops with intense physical activity and changes in body position.
Therefore, when the patient is in an upright position, his condition is normal, because due to contraction, the diameter and length of the renal artery become the same, and the angle between the aorta and arteries increases.
In a healthy organism, when the body changes from a horizontal to a vertical position, compensatory reactions are triggered in the cardiovascular system, which is accompanied by gravitational movement of blood.
These processes are necessary to maintain normal blood circulation in the brain. Orthostatic disruptions in blood circulation occur due to insufficient compensatory reactions; they are a response to orthostasis.
It is noteworthy that some doctors believe that orthostatic hypotension and hypertension are not diseases, but conditions that occur when blood vessels cannot maintain a normal level of pressure. The reasons for this phenomenon are varied:
- poor nutrition;
- disruption of the endocrine system;
- stress;
- infectious diseases;
- intoxication, accompanied by hyperhidrosis, vomiting and stool disorder;
- blood loss;
- taking diuretics, antihypertensives, and vasodilators for a long time.
However, the main factor leading to loss of consciousness is ischemic anoxia. It develops when the myocardium cannot provide full cardiac output.
In this case, the heart rhythm is disturbed, due to which it cannot provide sufficient cerebral perfusion. There is also a decrease in pressure, the reasons for this lie in peripheral vasodilation, in which blood flow in the brain worsens.
In orthostatic hypertension, blood pressure often increases due to the presence of nephroptosis due to changes in body position or physical activity.
Hypotension of the orthostatic type is characterized by such manifestations as:
- sweating;
- malaise;
- darkening of the eyes;
- hearing impairment;
- blurred vision;
- dizziness.
But the leading sign of hypotension is fainting, which occurs when blood pressure decreases greatly, as a result of which blood flow also worsens and neuronal metabolism is disrupted.
This condition is also called postural hypotension. The clinic of loss of consciousness is stereotypical. That is, fainting occurs against the background of the same conditions. Often the patient’s eyes become dark in the morning and evening when he suddenly changes his horizontal position to a vertical one. But as soon as the patient assumes a horizontal position, his general condition and blood pressure levels normalize.
Postural hypotension with loss of consciousness and dizziness is often the only symptom of a disease such as orthostatic idiopathic hypotension.
It is characterized by constantly developing autonomic failure, when the preganglionic neurons of the lateral horns of the spinal cord are affected. In severe cases of the disease, patients are forced to remain in bed, since any change in body position leads to fainting.
Orthostatic hypertension is accompanied by symptoms such as lower back discomfort and headache. The disease is often accompanied by angiospastic retinopathy.
To confirm or refute the presence of orthostatic hypertension and hypotension, it is necessary to study the medical history and medications taken by patients, identify influencing factors and examine organs and systems using percussion, auscultation, palpation and other methods.
Active orthostatic load is also checked. To do this, the patient changes position (lying-sitting). During this, skeletal muscles take part in hemodynamic adaptation to orthostasis, which is strongly expressed even if the muscles voluntarily relax.
But most often the Shellong test is performed, which eliminates the participation of skeletal muscles in orthostatic adaptation.
The procedure takes place on a rotating table. Thus, the patient's body is passively transferred to a semi-vertical and vertical position.
An orthostatic test makes it possible to study the patient’s condition, measure blood pressure and heart rate. If the upper pressure decreases by 20 units, and the lower pressure by 10 or more, then this confirms the presence of orthostatic hypotension, in particular when this condition is accompanied by fainting. In addition, the progression of the disease is indicated by loss of muscle tone and collapse.
It is worth noting that if the patient’s age is over 60 years, then the pressure is measured not only in a sitting or lying position, but also when the patient stands for five minutes. The fact is that in older people, orthostatic hypertension often develops during treatment with hypertensive drugs.
Moreover, to establish an accurate diagnosis, it is necessary to conduct instrumental and laboratory studies.
It is equally important to distinguish the manifestations of hypotension and hypertension from ordinary fainting conditions. Thus, a simple loss of consciousness is different in that when it occurs in similar situations, over time it becomes not very pronounced, and then disappears altogether.
Signs of orthostatic hypertension and hypotension are almost always expressed equally. Consequently, people with blood pressure problems always know what conditions lead to fainting, and in other situations it is not always possible to determine when they will happen.
In addition, simple loss of consciousness often occurs when a person is in a trochanteric position, and with hypotension and hypertension it occurs when the position changes. Fainting also often develops against the background of physical activity.
Also, during normal loss of consciousness, the skin becomes warm and moist, and a warmth is felt throughout the body, which is not the case in the case of low or high blood pressure.
Often, treatment for orthostatic hypotension comes down to taking medications containing caffeine. The doctor may also prescribe medications containing hormones that affect the endocrine and nervous systems.
For orthostatic hypertension caused by nephropathosis against the background of functional stenosis of the renal artery, surgical intervention – nephropexy – is indicated. During such treatment, the kidney is fixed in a physiological position using laparoscopic or open access.
In addition, proper nutrition plays an important role in the treatment of orthostatic hypertension and hypotension. So, the diet should be nutritious, light, with limited salt intake, enriched with beneficial vitamins and microelements. The video in this article will continue the topic of hypotension.
Humoral influences on cardiac activity
The activity of the heart is influenced by hormones and salts in the blood.
Of the hormones, adrenaline and acetylcholine are of particular interest. If you add a few drops of adrenaline to the Ringer's solution passed through the heart, the activity of the heart becomes more frequent and intensifies.
Acetylcholine acts diametrically opposite to adrenaline, which causes a sharp slowdown and weakening of cardiac activity up to complete cardiac arrest. If the influence of hormones is compared with those changes in the activity of the heart that are observed when nerves are irritated, then it turns out that adrenaline acts like the sympathetic nervous system, and acetylcholine acts like the parasympathetic nervous system, in particular, like the vagus nerve?
Of great importance for understanding the mechanism of transmission of excitation from the nerve ending to the muscle were the studies of Otto Lewy, conducted in 1921 with the isolated heart of a frog. In these experiments, Ringer's solution was passed through an isolated frog heart and at the same time the cardiac fibers of the vagus nerve, prepared along with the heart, were irritated. Irritation of the vagus nerve caused a slowdown in heart activity.
Ringer's solution, taken from such a stopped or slowed heart, was passed through a second, isolated, normally functioning heart, all of whose nerves had been cut during dissection. At the same time, the activity of the second heart changed sharply, its work was inhibited, although the vagus nerves innervating it were cut and were not irritated.
It was quite natural to conclude that such a slowdown or cessation of heart activity could be caused by some substance in the solution. This substance could only get into Ringer's solution through irritation of the vagus nerves. Further analysis showed that the solution taken from the heart when irritating the vagus nerves contained acetylcholine, which acts like the vagus nerve. The same experiments were carried out to study the possibility of the formation of physiologically active substances in the endings of sympathetic nerves. In the experiment with an isolated heart, it was not the vagus nerves that were irritated, but the cardiac branches of the sympathetic nervous system.
At the same time, heart contractions became more frequent. The solution taken from the heart was passed through a second isolated heart. The contractions of this heart also became more frequent. Therefore, it could be assumed that when sympathetic nerves are irritated, substances are formed at their endings that act like sympathetic nerves. These substances turned out to be similar to adrenaline and were later named sympathin.
These and further studies have shown that the transfer of excitation from the vagus nerve to the heart occurs with the participation of acetylcholine, which is formed in the endings of the vagus nerve. The transfer of excitation from the sympathetic nerve occurs with the participation of an adrenaline-like substance - norepinephrine, which is formed in the endings of the sympathetic nerve. Substances formed at nerve endings (acetylcholine and norepinephrine) and involved in the transmission of excitation are called transmitters.
Ions of certain salts also affect the functioning of the heart. For example, an increase in the concentration of potassium ions causes inhibition of the heart, and an increase in the concentration of calcium ions, on the contrary, increases the frequency and intensification of cardiac activity. Thus, the effect of potassium to a certain extent resembles the influence of the vagus nerves, and calcium also to a certain extent resembles the influence of the sympathetic nerves.
For normal activity of an isolated heart, it is necessary that the solution passed through must contain potassium and calcium ions, and in a certain ratio. If you remove potassium or calcium ions from a solution, the heart stops and resumes its work again after adding the removed ions.
It should be emphasized that humoral influences are closely related to the activity of the nervous system and are ultimately determined by the activity of the nervous system, in particular the central nervous system, as was shown above.
Article on the topic Hormones affecting the heart
Diagnosis of hormonal tachycardia
It is carried out taking into account the underlying disease. First of all, a consultation with an endocrinologist is scheduled, who gives directions for specific tests that help determine the level of certain hormones. To determine the form of tachycardia, a standard ECG is used; Holter monitoring can be performed, which is more informative in the case of paroxysmal tachycardia.
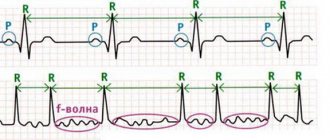
The ECG shows the following signs of tachycardia:
- The rhythm often remains sinus.
- The QRS, or ventricular complex, changes and this resembles a branch block or extrasystole with ventricular localization.
- In the presence of a deformed QRS complex, in rare cases the P wave is visible, most often it is not detected.
If the patient allegedly has a hereditary connection with hormonal imbalance, then magnetic resonance imaging is performed. This research method also helps in identifying tumor tumors in the brain and adrenal glands.
TESTING “ENDOCRINE GLANDS”
Basedow's disease, accompanied by an increase in heart rate, blood pressure, and excitability of the nervous system, occurs in humans due to dysfunction
3) pancreas
4) thyroid gland
With the help of chemicals carried by the blood to all cells of the body, regulation is carried out
Hormones are biologically active substances that are produced in the glands
1) salivary and sebaceous
3) internal secretion
4) tear and sweat
The pancreas produces not only pancreatic juice, but also hormones involved in metabolism
4) minerals
Diabetic patients are injected into the blood
2) thyroid hormone
4) sex hormones
Excess sugar in the blood and urine indicates disturbances in activity
1) thyroid gland
3) pancreas
The amount of sugar in a person’s blood and urine is regulated by the hormone insulin, which is produced
1) glands of the stomach
2) thyroid gland
4) pancreas
What role do hormones play in the human body?
1) accelerate chemical reactions in cells
2) protect the body from the penetration of pathogenic bacteria
3) participate in the formation of enzymes
4) regulate vital processes
The level of sugar in the blood necessary for normal life is maintained due to the action of1) pituitary hormones
2) thyroid hormone
3) adrenal hormones
4) adrenaline and insulin
When the cells of the pancreas, which produce hormones, are damaged, a person becomes ill
1) stomach ulcer
3) diabetes mellitus
4) cretinism A hormone containing iodine produces:
1) pancreas
4) thyroid gland
Treatment and prevention of hormonal tachycardia
In the presence of hypertension combined with hormonal tachycardia, standard antihypertensive drugs are prescribed - calcium antagonists, alpha-blockers, dopamine synthesis blockers. Some of them are able to reduce heart rate, which is still more effectively restored with the help of beta blockers.
In the presence of tumor processes, surgical treatment is used. Using laparoscopy, a pheochromocytoma can be removed or surgery can be performed to remove a tumor in the brain. In rare cases, radiation is used to slow the growth of tumor tissue.
Diseases of the thyroid gland can be treated with specific medications, including drugs that normalize cardiac activity in the prescription list. These can be selective or non-selective beta blockers, with the latter type of medicine being able to slightly reduce the level of thyroid hormones.
There is no specific prevention of hormonal therapy. To reduce the risk of arrhythmia due to an imbalance of hormonal activity, you need to follow general recommendations for strengthening the cardiovascular system.
4.55 Aug. rating ( 90 % score) – 11 votes – ratings
Hormonal regulation of heart activity.
Factors of humoral regulation are divided into two groups:
substances of systemic action;
local substances.
For systemic substances
include electrolytes and hormones.
Electrolytes ( Ca ions
) have a pronounced effect on the functioning of the heart (positive inotropic effect).
With an excess of Ca, cardiac arrest may occur during systole, since there is no complete relaxation. Na ions can have a moderate stimulating effect on the activity of the heart. With an increase in their concentration, a positive bathmotropic and dromotropic effect is observed. K ions
in high concentrations have an inhibitory effect on cardiac function due to hyperpolarization. However, a slight increase in K stimulates coronary blood flow. It has now been found that with an increase in the level of K compared to Ca, a decrease in heart function occurs, and vice versa.
Hormone adrenaline
increases the strength and frequency of heart contractions, improves coronary blood flow and increases metabolic processes in the myocardium.
Thyroxine
(thyroid hormone) enhances heart function, stimulates metabolic processes, and increases the sensitivity of the myocardium to adrenaline.
Mineralocorticoids
(aldosterone) stimulate Na reabsorption and K excretion from the body.
Glucagon
increases blood glucose levels due to the breakdown of glycogen, leading to a positive inotropic effect.
Sex hormones
in relation to the activity of the heart they are synergists and enhance the work of the heart.
Substances of local action
act where they are produced.
These include mediators. For example, acetylcholine
has five types of negative effects on the activity of the heart, and norepinephrine has the opposite effect
.
Tissue hormones (kinins) are substances with high biological activity, but they are quickly destroyed, and therefore have a local effect.
These include bradykinin, kalidin, moderately stimulating blood vessels. However, at high concentrations they can cause a decrease in heart function. Prostaglandins,
depending on the type and concentration, can have different effects. Metabolites formed during metabolic processes improve blood flow.
Thus, humoral regulation ensures a longer adaptation of the heart’s activity to the needs of the body.