Small Diameter of Vertebral Arteries: Normal, What It Is
The vertebral arteries perform the function of blood supply to the posterior parts of the brain. They carry nutrients to vital areas of the brain. However, the diameter of the vertebral arteries, the norm of which is 3.6 - 3.8 mm, may be underdeveloped and narrowed. As a rule, hypoplasia is a congenital disease. The consequences of the anomaly can be quite negative for brain activity. This is explained by a violation of hemodynamics, which entails a lack of nutrition in its individual areas, dysfunction of the vestibular apparatus, heart rhythm and circulatory system.
Ideally, the right and left vertebral arteries have the same development. They form the Circle of Willis in the brain, dividing into a number of small vessels in the area of the subclavian arteries. Hypoplasia is underdevelopment of body tissues. In this case, the pathology can be congenital or acquired.
In most cases in clinical practice, hypoplasia of the right vertebral artery of small diameter is observed, in rare cases - of the left vertebral artery. An anomaly on both sides at once is recorded very rarely in medical practice. The pathology can be congenital, much less often acquired.
Small diameter of both vertebral arteries
Dear doctor, I have been feeling dizzy for about 2 months, after being stressed at work and working with a computer, I feel a little wobbly, nauseous, my right arm is numb, and my vision has deteriorated.
And a week ago, in the morning, after sleep, everything swam before my eyes, I had difficulty getting up, my ears were blocked, I had difficulty thinking. The doctor ordered an examination. Duplex scanning of the brocephalic arteries. Here it is: linear blood flow velocity: common carotid artery on the right 68, left 70: internal carotid artery on the right 59, left 62: external carotid artery on the right 64, left 65: vertebral artery on the right 32, left 20.
The arteries under study—common carotid, external carotid, vertebral—are patent on both sides. The bifurcation is average. There are no pathological inclusions. Atherosclerotic plaques are vasulated. The IMC is not thickened: it is unevenly thickened along the CCA up to 0.9 mm.
There is no deformation of the course of the CCA, ECA, ICA, the entire color is 1.5 mm on the right, 1.1 mm on the left. Along the length, the blood flow is not changed, increased blood flow along the course is 1.1 mm on the left. PA: the diameter of the right PA is 3.6, the left PA is 2.3 mm, the PA is passable on both sides (right, left), the speed spectral characteristics along them are (not) symmetrical.
Presence of deformation of the course of the PA systems. the move is very PA in the cost. can. Conclusion: signs of initial astechondrotic changes in the vascular wall of the main artery. Small diameter of the left vertebral artery of the blood flow of the left VA. (moderate. Where italic font is written by hand and abbreviations are not clear.
For many years now I have been having attacks of shortness of breath, and then my face turns red. Tell me, doctor, how can my problem be solved or treated?
Small Diameter of Vertebral Arteries: Normal, What It Is
The vertebral arteries perform the function of blood supply to the posterior parts of the brain. They carry nutrients to vital areas of the brain. However, the diameter of the vertebral arteries, the norm of which is 3.6 - 3.8 mm, may be underdeveloped and narrowed.
As a rule, hypoplasia is a congenital disease. The consequences of the anomaly can be quite negative for brain activity.
This is explained by impaired hemodynamics, which entails a lack of nutrition in its individual areas, dysfunction of the vestibular apparatus, heart rhythm and circulatory system.
Ideally, the right and left vertebral arteries have the same development. They form the Circle of Willis in the brain, dividing into a number of small vessels in the area of the subclavian arteries. Hypoplasia is underdevelopment of body tissues. In this case, the pathology can be congenital or acquired.
In most cases in clinical practice, hypoplasia of the right vertebral artery of small diameter is observed, in rare cases - of the left vertebral artery. An anomaly on both sides at once is recorded very rarely in medical practice. The pathology can be congenital, much less often acquired.
Main causes and symptoms
The causes of the disease are related to the intrauterine development of the child:
- bruise and injuries to the expectant mother,
- excessive use of alcohol, drugs,
- nicotine addiction;
- irradiation with certain types of gamma rays, with prolonged overheating;
- infectious diseases: influenza, rubella, toxoplasmosis.
Hypoplasia of the left or right vertebral artery leads to the gradual onset of symptoms, making it very difficult to diagnose.
Among the main signs of the disease are:
- frequent dizziness;
- causeless pain in the head;
- decreased sensitivity of individual parts of the body;
- deterioration of movement coordination;
- decreased vision and hearing;
- deterioration of attention, memory and concentration.
All of these symptoms occur with varying frequency. They are characteristic of pathology of the left or right vertebral artery of prolonged development.
At the same time, patients often experience sudden changes in mood, depression, severe weakness and fatigue.
Weather dependence may also appear when a person begins to feel unwell due to temperature changes and changes in atmospheric pressure. In addition, sleep disturbance may occur.
With the development of this disease, a significant narrowing of the vascular lumen occurs in the area where it enters the bone canal leading into the cranial cavity. As a result, insufficient blood begins to flow into the brain. This factor explains hemodynamic abnormalities in VA underdevelopment.
Any symptoms that arise in the presence of pathology are caused by the fact that the vertebral arteries supply the brain with nutrients and nourishment, and even minor disturbances in their work are manifestations of deterioration in cerebral blood flow. Over the years, the symptoms intensify, and this is not surprising: the vessels begin to lose elasticity and become “clogged.” Therefore, the lumen narrows even more.
The small diameter of the PA can be on the right side or on the left. Hypoplasia of the right vertebral artery is observed in almost 10% of citizens. Diseases of the left VA are much less common.
Diagnostics
The disease can be identified during the first examination by a neurologist. The doctor listens to the patient’s complaints about his general condition, takes into account possible disorders in the cervical spine, and writes a referral for ultrasound diagnostics.
If during the examination a narrowing of the lumen in the diameter of the vertebral artery was revealed to 2 mm when the norm is 3.6 - 3.8 mm, this is considered a diagnostic symptom proving the presence of the disease.
If necessary, angiography is performed - x-ray diagnostics of blood vessels using a contrast agent, clearly demonstrating their current condition.
If a disease is suspected, the doctor must write a referral for a vascular ultrasound. This diagnosis allows you to determine the diameter of the artery. A narrowing of the internal diameter is considered an anomaly; the norm varies in the range of 3.6 - 3.8 mm. A pathological change is considered to be a diameter of less than 2 mm.
According to indications, tomography and angiography of the arteries are performed using a contrast agent. These studies help provide a complete picture of vascular abnormalities. Often, hypoplasia is aggravated by disorders of the vertebrae located in the cervical region. This can also be detected during diagnostics.
The following methods allow you to set a competent one:
- Ultrasound of the vessels of the neck and head. In particular, duplex angioscanning of the VA is recommended. During the examination, an image of the artery is displayed on the monitor, allowing you to determine the diameter and pattern of blood movement. This method is often used as screening, since it is completely safe and has no contraindications.
- Angiography is a graphic recording of the anatomical structure, features of the course and connections of all cerebral vessels. First of all, this method allows you to evaluate the vertebral artery. Diagnosis is carried out using a special X-ray machine. In this case, one of the largest arteries of the extremities is punctured, a conductor is laid to the branching site of the VA and a contrast agent is injected into it. Its structure is assessed by its external features, displayed on the monitor.
- Tomographic examination using contrast. The examination is performed on magnetic resonance or computed tomography scans using a contrast enhancer that fills the arteries.
Source: //ogomeopatii.ru/malyj-diametr-obeih-pozvonochnyh-arterij/
Main causes and symptoms
The causes of the disease are related to the intrauterine development of the child:
- bruise and injuries to the expectant mother,
- excessive use of alcohol, drugs,
- nicotine addiction;
- irradiation with certain types of gamma rays, with prolonged overheating;
- infectious diseases: influenza, rubella, toxoplasmosis.
Hypoplasia of the left or right vertebral artery leads to the gradual onset of symptoms, making it very difficult to diagnose.
Among the main signs of the disease are:
- frequent dizziness;
- causeless pain in the head;
- decreased sensitivity of individual parts of the body;
- deterioration of movement coordination;
- decreased vision and hearing;
- deterioration of attention, memory and concentration.
All of these symptoms occur with varying frequency. They are characteristic of pathology of the left or right vertebral artery of prolonged development. At the same time, patients often experience sudden changes in mood, depression, severe weakness and fatigue. Weather dependence may also appear when a person begins to feel unwell due to temperature changes and changes in atmospheric pressure. In addition, sleep disturbance may occur.
With the development of this disease, a significant narrowing of the vascular lumen occurs in the area where it enters the bone canal leading into the cranial cavity. As a result, insufficient blood begins to flow into the brain. This factor explains hemodynamic abnormalities in VA underdevelopment.
The small diameter of the PA can be on the right side or on the left. Hypoplasia of the right vertebral artery is observed in almost 10% of citizens. Diseases of the left VA are much less common.
Diagnostics
The disease can be identified during the first examination by a neurologist. The doctor listens to the patient’s complaints about his general condition, takes into account possible disorders in the cervical spine, and writes a referral for ultrasound diagnostics. If during the examination a narrowing of the lumen in the diameter of the vertebral artery was revealed to 2 mm when the norm is 3.6 - 3.8 mm, this is considered a diagnostic symptom proving the presence of the disease. If necessary, angiography is performed - x-ray diagnostics of blood vessels using a contrast agent, clearly demonstrating their current condition.
If a disease is suspected, the doctor must write a referral for a vascular ultrasound. This diagnosis allows you to determine the diameter of the artery. A narrowing of the internal diameter is considered an anomaly; the norm varies in the range of 3.6 - 3.8 mm. A pathological change is considered to be a diameter of less than 2 mm.
According to indications, tomography and angiography of the arteries are performed using a contrast agent. These studies help provide a complete picture of vascular abnormalities. Often, hypoplasia is aggravated by disorders of the vertebrae located in the cervical region. This can also be detected during diagnostics.
The following methods allow you to set a competent one:
- Ultrasound of the vessels of the neck and head. In particular, duplex angioscanning of the VA is recommended. During the examination, an image of the artery is displayed on the monitor, allowing you to determine the diameter and pattern of blood movement. This method is often used as screening, since it is completely safe and has no contraindications.
- Angiography is a graphic recording of the anatomical structure, features of the course and connections of all cerebral vessels. First of all, this method allows you to evaluate the vertebral artery. Diagnosis is carried out using a special X-ray machine. In this case, one of the largest arteries of the extremities is punctured, a conductor is laid to the branching site of the VA and a contrast agent is injected into it. Its structure is assessed by its external features, displayed on the monitor.
- Tomographic examination using contrast. The examination is performed on magnetic resonance or computed tomography scans using a contrast enhancer that fills the arteries.
What does an ultrasound scan of the neck vessels show?
Ultrasound of the vessels of the neck and head is the most accessible way to detect the cause of brain dysfunction. As a rule, such patients are often bothered by loss of consciousness (especially during exertion), attacks of dizziness, nausea, and spontaneous headaches. The most severe damage is ischemic stroke, which occurs when there is severe occlusion (“blockage”) of one of the arteries in the brain. In the presence of the above conditions, it is first recommended to do an ultrasound examination.
Treatment
Treatment is carried out using two methods:
- Conservative. It involves the introduction of drugs that improve blood properties, blood supply to the brain and metabolic processes in it. Such methods do not completely eliminate the disease, but only provide protection to the brain from ischemic abnormalities. For this purpose, various medications are used, in particular blood thinners.
- Surgical. Used in situations where it is impossible to compensate for cerebral circulation in other ways. Experienced surgeons perform endovascular surgery, the meaning of which is to insert a stent into the lumen of a narrowed vessel. This is a special dilator that increases the diameter of the artery, normalizing blood flow.
Prevention
Simple preventive measures will help prevent negative consequences for the body. If you regularly play sports, before training you should drink some water and perform a light back massage. This simple tactic helps to speed up the blood, improve metabolism and absorb the necessary amount of moisture into the intervertebral discs.
Try not to lift or hold heavy objects with outstretched arms. You need to learn how to carry weights correctly so as not to injure your back. With an even posture, you need to squat down, take the load and straighten your legs with it. At the same time, place your hands as close to your body as possible. Distribute the load evenly, so you don't have to carry it in one hand if you can carry two bags in both hands. Use bags, carts and rolling suitcases to transport heavy items.
When doing heavy physical work, which is inherently associated with lifting weights, wear a special support belt or corset. Do not lift loads weighing more than 10 kg. Use comfortable shoes in everyday life, giving preference to models made from natural raw materials that securely and securely support your foot.
Women, especially during pregnancy, should avoid wearing high-heeled shoes, as they are very harmful to the spine. After being in a bent position for a long time, you can hang on the bar or stretch up.
The vertebral arteries are designed to supply blood to the posterior parts of the brain. The supply of nutrients to this area depends on them, which can be blocked in case of underdevelopment of the arteries due to hypoplasia. To prevent pathology, you need to know what the small diameter of the right and left vertebral artery should be, understand the causes, symptoms and methods of diagnosing this disease in adults and children.
What should be the diameter of the vertebral artery
A normal diameter is considered to be within the range of 3.6-3.8 mm; with pathology, this range decreases due to underdevelopment or narrowing. Most often, hypoplasia is congenital, which negatively affects brain function. This occurs due to problems with hemodynamics, poor blood flow to certain parts of the brain, disturbances in the functioning of the vestibular apparatus, as well as heart rhythm.
Normally, the right and left arteries should be the same. They are responsible for the formation of the Circle of Willis in the brain and are divided into a number of numerous vessels in the arterial zone under the clavicles. Hypoplasia is tissue underdevelopment and can be either congenital or acquired. In clinical practice, pathology of the right artery with a small diameter most often occurs; occasionally it affects the vertebral artery on the left. Bilateral anomaly is recorded very rarely, as is acquired hypoplasia.
The Circle of Willis is the basis for the normal supply of blood to all body systems. It consists of large vertebral arteries with left and right branches, which develop evenly under normal conditions.
Anatomy
The right and left vertebral arteries emerge from a. subclavia (or its branches). They then enter the transverse process of C6 (sixth cervical vertebra) and go straight upward. At the level of C1, they continue from the transverse foramen into the posterior arch and through the suboccipital triangle merge into the common basilar artery, which enters the foramen magnum (see also How the human spine is structured).
This is interesting. Normally, the diameter of the right VA is 2.8-3.8 mm.
The photo shows the structure of the vertebral arteries
In topographic anatomy, each VA is divided into four parts.
Table: Parts a. vertebralis:
| Part | Topographic location |
| Running backward and upward between the cones of Longus and the anterior part of Skalenu | The veins (vertebral and internal jugular) are located anteriorly. Intersects with the inferior thyroid artery. |
| Passing strictly upward through the transverse processes of C6-C2 | Surrounded by a plexus of veins flowing into v. vertebralis, and branches of the inferior cervical sympathetic ganglion. |
| Emerging from the C2 process on the inner side of the rectus lateralis muscle | The anterior branch of the first cervical nerve is located more medially. The suboccipital nerve is located between this part of the artery and the posterior arch of the atlas. |
| Penetrating through the dura mater | It is located between the anterior root of the first cervical nerve and the hypoglossal nerve. |
Note! Most people have a right a. vertebralis is thinner than the left one and, accordingly, delivers less blood.
Features of blood supply
Several branches depart from the vertebral artery:
- rr. musculares – nourish the prevertebral muscles of the neck;
- rr. spinales - supply blood to the gray matter of the spinal cord and its membranes;
- a. spinalis posterior and anterior - also carry blood to the spinal cord and membranes;
- a. cerebelli inferior posterior – nourishes the infero-posterior parts of the cerebellar hemispheres, the medulla oblongata, etc.
The vessel mainly supplies the posterior parts of the brainstem
The structure and topography of the vessel are quite complex, so its pathologies are common in medical practice. In the sections below we will look at common vertebral artery disease syndromes.
Small diameter vertebral arteries
Pathology is divided into three types: left-sided, right-sided and bilateral. The problem with the right artery occurs due to improper development of the child in the womb. It is provoked by bruises or irradiation of a woman, nicotine, alcohol and prolonged overheating of the body. In adulthood, the patient begins to complain of dizziness, headaches, increased blood pressure, drowsiness, vestibular and emotional disorders. A congenital disease in humans does not require special treatment, since the body finds a way to compensate for the lack of blood supply on the right side on its own properly. In rare cases, malfunctions occur that require the intervention of specialists, and concomitant diseases develop, for example, atherosclerosis.
Problems with the artery located on the left depend on circulatory disorders and appear gradually. Hemodynamic dysfunction provokes vascular obstruction, blood stagnation and ischemia of various organs. The process develops gradually and can last for several years, leading to negative consequences.
An alarming sign is pain in the cervical spine and anastomosis - the connection between the branches of the great vessels. Hypoplasia of the left-sided type and linear process often leads to increased blood pressure and atherosclerosis. The disease includes many individual symptoms that may vary among patients. The list of basic features includes:
- headaches of varying degrees of intensity;
- dizziness for no specific reason;
- dysfunction of the nervous system and distortion of perception in space;
- frequent increase in blood pressure;
- disturbance of fine movements and problems with sensitivity, most often of the limbs;
- motor dysfunction, including paresis or paralysis affecting one or both hemispheres, damage to one side on the right or left;
- visual hallucinations, borderline disorders;
- problems with coordination of movements, decreased speed, unsteadiness while walking.
The pathology may not manifest itself as individual symptoms for a long time. Its danger lies in the fact that it is impossible to make an accurate diagnosis during the initial examination; doctors attribute the signs of hypoplasia to other diseases. If left untreated, the consequences will be the same as with hyperplasia; over time, changes will affect the area of the bone canal and the artery that flows into it.
If the normal diameter of a number of vertebral arteries is disrupted, patients begin to suffer from severe and recurring headaches, fatigue develops, hearing deteriorates and visual acuity decreases.
Common pathologies
Tortuosity
Pathological tortuosity of the right VA is a hereditary syndrome. The mechanism of its development lies in the atypical structure of blood vessels, in which collagen fibers predominate over elastic fibers.
Over time, this can lead to various deformations:
- S-like, smooth, which usually develops if the length of the artery is longer than normal;
- coiling – formation of a vascular loop;
- Kicking – bending a vessel at an acute angle.
Forms of crimp (see description above)
Clinically, the syndrome is manifested by the following symptoms:
- dizziness, aggravated by sudden movements of the head or lifting heavy objects;
- attacks of headache;
- noise, ringing in the ears;
- feeling of heaviness, pressure in the head;
- flashing “spots” before the eyes;
- short-term disturbances of consciousness, fainting;
- problems with coordination of movements;
- periodically occurring severe weakness in the arms.
Stenoses and occlusions
Stenosis of the right VA, a vessel that supplies the brain and spinal cord, is a dangerous condition. It is fraught with the development of hypoxia of nervous tissue and even stroke (ischemic stroke).
Critical narrowing of the vessel can lead to stroke
Important! Total aa. Vertebralis bring up to 25% of the total blood to the brain.
By its nature, stenosis of vertebral vessels can be:
- functional – occurs in a certain position of the neck in patients with osteochondrosis (see also treatment of osteochondrosis), spondylosis, ankylosing spondylitis and other degenerative processes in the spine;
- organic - formed with atherosclerosis, uncovertebral arthrosis, with hypertonicity of the scalene muscles.
Osteochondrosis is not as harmless as many people think
Symptoms of the pathology include:
- visual and oculomotor disorders (blurred vision, the appearance of dark spots or flashes of light before the eyes, “spots”);
- ataxia – difficulty maintaining body balance in space;
- vestibular disorders – dizziness, nystagmus;
- sometimes – pain in the cervical-occipital region.
If the cause of vessel stenosis is most often its compression in a certain area or the formation of an atherosclerotic plaque, then occlusion of the right vertebral artery is usually caused by blockage with a blood clot. Moreover, even a partial decrease in the lumen of the vessel can lead to vivid clinical symptoms.
If there are risk factors, an artery may become blocked by a blood clot.
The syndrome is characterized by:
- intense pain;
- pallor of the facial skin with subsequent development of cyanosis;
- paresthesia - a feeling of tingling, crawling;
- later – paralysis and paresis.
Important! When an artery is completely blocked, literally minutes count: without sufficient oxygen supply to the brain, ischemia and stroke quickly develop. In this case, the price of delay is human life.
Aplasia and hypoplasia
Hypoplasia and aplasia of the right vertebral artery are usually congenital defects. This syndrome leads to various hemodynamic disorders and numerous dysfunctions in the posterior regions of the brain, heart and circulatory system as a whole.
Underdevelopment of the artery can lead to serious problems
Talk about hypo- or aplasia a. vertebralis is possible if the following symptoms are present:
- frequent attacks of dizziness;
- headache;
- distorted perception of the position of one’s own body;
- reduction or complete disappearance of sensitivity;
- neurological and mental dysfunctions - insomnia, asthenia, decreased criticism, hypophobia of the right vertebral artery.
- arterial hypertension.
How to diagnose hypoplasia
You can find out about disruption of the left small-diameter vertebral artery of the body during an examination by a neurologist. After identifying the symptoms, the doctor writes a referral for an ultrasound or LSC. If during the diagnostic process a narrowing of the lumen of the vertebral artery to 1 or 2 mm is detected, this proves the presence of pathology. If necessary, angiography can be additionally performed - the introduction of a contrast component into the vessels to determine their condition.
First of all, the patient is prescribed an ultrasound examination of blood vessels to determine the diameter of the artery and MRI. For additional indications, tomography is performed to obtain a complete picture of vascular pathology. Exacerbation processes can also be identified during diagnosis. An accurate diagnosis can be made using ultrasound of the vessels of the head and neck; doctors often recommend performing a small duplex angioscan. During the study, the artery will be visible on the monitor, which allows you to clarify its diameter and the nature of blood flow.
An angiographic study is a graphically fixed picture of the anatomy, characteristics of the connections and course of the vessels of the brain and the intracranial canal. This technique allows you to assess the condition of healthy and diseased vertebral arteries in men and women, including even small deviations from the norm. Diagnosis in this way is carried out using an X-ray machine. The largest artery of the limb is punctured in the patient, a guide is applied to the branching area of the VA and a special substance is injected inside. The structure of the artery is assessed by its appearance, which is displayed on the monitor.
Another diagnostic method is examination using a tomograph using a contrast agent. It is carried out using computer or magnetic resonance machines, introducing an amplifier that fills the arteries. In this way, it is possible to determine the diameter of the vertebral arteries in children and adults, as well as early signs of pathology.
How is an ultrasound of the neck and head performed?
Ultrasound examination is done according to standard methods. The doctor applies a special gel to the neck area to facilitate signal transmission and consistently examines the necessary vessels. It is important for the patient to know several fundamental points before performing an ultrasound of the cerebral vessels:
- No preparation is required from the patient before the study;
- Position – For optimal diagnosis, the patient should be positioned on their back, with a thin pillow under their head. For people with short necks, it is better to place a thick cushion/pillow between the shoulder blades. In this position, a slight hyperextension of the cervical spine occurs, due to which almost all vessels become visible. To obtain a high-quality image of the vertebral arteries, the doctor may ask you to turn over to your side;
- The procedure can take up to 20 minutes.
It should be noted that in some patients, ultrasound of the head and neck vessels may give false results. This occurs due to compression of the vessel (usually the vertebral artery), as a result of which the speed of blood flow changes and “branching” may appear. This phenomenon can be observed in patients:
- Osteochondrosis stages II-IV;
- Osteophytosis;
- Vertebral instability;
- Herniated intervertebral discs in the cervical region (except for Schmorl's hernia);
- Bekhterev's disease (ankylosing spondyloarthritis).
Despite this, the method is highly informative, since it shows even small changes in the arteries of the neck. With correct decoding, you can promptly determine the cause of the disease (ischemic stroke, vertebral artery syndrome, etc.) or diagnose it at an early stage.
Methods of treatment and prevention
Hypoplasia and hyperplasia can be treated with various methods. Conservative methods involve the injection into a vein of drugs that improve the properties of the blood, the general blood supply to the brain and all metabolic processes in it. Such methods are not able to completely eliminate the disease; they only protect the brain from progressive ischemic processes. Additionally, medications are used, in particular blood thinners. Surgical methods of solving the problem are used when the blood circulation of the brain cannot be compensated in any other way.
During the operation, doctors perform an endovascular procedure, the essence of which is to insert a stent of the required thickness into the lumen, expanding the vessel. This dilator helps increase the diameter of the artery and normalize blood flow to the required level.
You can prevent problems and negative consequences for the entire body with the help of simple preventive measures. It is necessary to exercise regularly, drinking a small amount of water before exercise and performing a simple back massage. This method helps to disperse the blood, improve metabolism and give the intervertebral discs the opportunity to absorb the required volume of fluid.
If asymmetrical, transverse or standard hypoplasia is diagnosed, you should not do heavy physical work associated with lifting and holding heavy objects. If necessary, it is better to wear a special belt or corset. Patients should not lift loads weighing more than 10 kg; wheeled bags, trolleys and suitcases are used to transport large items.
In everyday life, you need to wear comfortable shoes of the right size, made from natural materials and that support your feet. Women should avoid wearing high-heeled shoes.
The article presents data on the prevalence and clinical significance of vertebral artery (VA) hypoplasia in civil aviation pilots of the older age group. An expert assessment of the professional prognosis of flight personnel with manifestations of
The article presents the data on the prevalence and clinical significance of vertebral artery hypoplasia in civil aviation pilots of older age group. Expert assessment of professional prognosis was done for airmen with manifestations of vertebral artery hypoplasia.
Special requirements are imposed on the health of pilots in order to maintain medical flight safety. The greatest attention is paid to the state of the cardiovascular system with an assessment of the blood supply to various pools, primarily the coronary and cerebral.
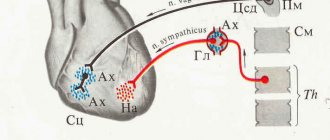
The blood flow of the central nervous system is 70–85% provided by the blood supply of the carotid arteries and 15–30% by the vertebral arteries (VA). The right vertebral artery (RVA) is the first branch of the right subclavian artery to arise from the brachiocephalic trunk; left (LPA) - the left subclavian artery, which originates from the aortic arch. Both VAs rise to the brain in the bony canal and merge in the cranial cavity, forming a large basilar artery. PAs vascularize the stem structures of the brain, the occipital and temporal lobes, the cerebellum, the inner ear, the posterior parts of the hypothalamic region, and segments of the spinal cord. Thus, PAs play an important role in maintaining cerebral blood flow. Cerebrovascular reserve associated with the reactivity of the arteries of the vertebrobasilar system currently remains poorly understood in comparison with the territory of the middle cerebral artery. Only a few works are devoted to this problem.
One of the most common anomalies of VA is its hypoplasia, which occurs in the population, according to various authors, from 2.34% to 26.5% [1–11] and is congenital in nature. With VA hypoplasia, the lumen of the vessel at the site of its entry into the bone canal in the cranial cavity is significantly narrowed, which creates the prerequisites for compression of the artery by the long colli muscle (extravasal compression of VA) and significant difficulty in the flow of blood to the posterior parts of the brain with the development of non-vertebrogenic VA syndrome. Manifestations of VA compression are paroxysmal states associated with turning the head. The development of reflex vasospastic reactions due to irritation of the sympathetic plexus of the VA is also of important pathogenetic significance. The powerful flow of afferent impulses that arise in this case has an irritating effect on the overlying centers of vascular-motor regulation. The consequence of this is diffuse and local reactions, affecting mainly the vessels of the vertebrobasilar system [12]. Hypoplasia of the vertebral artery can predispose to the development of cerebral stroke both due to impaired circulation in the vertebrobasilar system (posterior basilar and posterior communicating arteries), and due to damage to the vascular wall of the vertebral artery by the atherosclerotic process and even its dissection.
Clinical manifestations of VA hypoplasia syndrome consist of three groups of symptoms: vertebral (pain in the spine, back of the head, neck, most often cervicalgia); local (pain at the point of the vertebral artery with irradiation to the head or pain on palpation of the structures of the spinal motion segment with irradiation to the head); symptoms at a distance (due to dysgemic phenomena both in the area of vascularization of the VA and due to irritation of the sympathetic plexus of the artery - angiodystonic reactions, increased blood pressure, migraine pain, visual, vestibular and auditory disorders, gait instability when walking). Features of the clinical manifestations of VA lesions are largely determined by the nature, localization and prevalence of lesions of the cerebral arteries and the functional state of the vascular system of the brain (collaterals, anastomoses, state of the vascular wall).
For a long time, VA hypoplasia can be asymptomatic, which makes its early diagnosis difficult. The main screening method of examination is triplex or duplex scanning of the vertebral arteries. It should be noted that there are different approaches to ultrasound diagnosis of this pathology: the range of the conventional norm varies from 2.5–2.8 mm to 3.8–3.9 mm; Two criteria for hypoplasia are used: less than 2.0 (used more often) and 2.5 mm. In the older age group, when functional compensatory mechanisms are impaired, hemodynamic disturbances can be detected. Thus, clinical manifestations increase with age.
The purpose of this study was to evaluate the prevalence and clinical significance of vertebral artery hypoplasia in older civil aviation pilots.
The work was carried out at the Department of Aviation and Space Medicine of the Russian Medical Academy of Postgraduate Education, Ministry of Health of the Russian Federation, on the basis of the Department of Expertise and Rehabilitation Treatment of the Central Clinical Hospital and TsVLEK GA, Moscow. The study included 1,189 civil aviation pilots aged 54–68 years, consecutively admitted for inpatient examination to the department of examination and rehabilitation treatment of the Central Clinical Hospital of Civil Aviation upon reaching the age of 55 years and older, followed by examination at the Central Clinical Hospital of Civil Aviation in 2009–2010. The majority of those examined did not have any complaints at the time of examination - 87.3% (n = 1038). In 12.5% of cases (n = 149) there were complaints of hearing loss, poor speech intelligibility, tinnitus, and in 0.17% of cases (n = 2) there were manifestations of angina pectoris. None of the subjects had any neurological complaints.
By professional affiliation: 48.1% - PIC; co-pilots - 11.4%; pilot instructors - 6.5%; flight engineers - 10.6%; flight mechanics - 12.8%; navigators - 8.9%; flight directors and their deputies - 1.7%. Study design: cross-sectional. All subjects examined were male. The average age of the examinees was 56.8 ± 0.07 years. Work experience in civil aviation - from 1 to 45 years, on average - 33.2 ± 0.21 years; flight time - 14,841.94 ± 111.95 hours (from 1070 to 29,771).
Methodology for triplex scanning of the vertebral arteries
Statistical processing was carried out using the SPSS software package, version 11.5 for Windows. The mean value (M ± m) and standard deviation (SD) were determined. The significance of differences was assessed using the Mann–Whitney U test. Differences were considered statistically significant at p References
V. V. Book*, Doctor of Medical Sciences, Professor G. N. Biryukbaeva**, Candidate of Medical Sciences A. Yu. Kuzmina*, Candidate of Medical Sciences
* GBOU DPO RMAPO Ministry of Health of the Russian Federation, Moscow ** Federal Budgetary Institution Central Clinical Hospital of Civil Aviation, Moscow
Standard measurements of blood flow velocity in the carotid arteries
The pulsed wave Doppler angle during the study is maintained as sharp as possible, ideally in the range of 45–60 degrees. It is good practice for the clinician to try to maintain a specific angle, such as 55 or 60 degrees, to improve inter-exam reproducibility. For significant stenoses, it is better to reduce the size of the control volume as this allows a better determination of the peak area of the systolic flow signal. Color Doppler allows a more accurate assessment of the direction of flow in stenosis, since it may not always be parallel to the vessel walls. The exact final location of the blood flow sample volume is selected using a combination of audio Doppler signal and spectrum so as to obtain the purest, highest frequency audio signal and the best spectral trace. For stenoses, the control volume should be moved along the length of the stenotic segment to determine the location of the peak signal. The gain for the spectral display should be set to use the full gray scale without over- or under-saturation.
For scientific purposes, it is always necessary to measure a given parameter precisely, for example as part of a population survey. To do this, it can be measured on the image of the distal wall of the common carotid artery, where echoes from the intima-media complex are most easily distinguished. Machine settings should be adjusted to provide a clear, clutter-free image of the vessel wall, and the transducer position should be adjusted to display the characteristic double appearance of the vessel wall.
The image of the CCA should be maximized using the “zoom” on the ultrasound machine screen to make the measurement easier to perform. Intima-medial thickness (IMT) is best demonstrated in the superior portion of the common carotid artery on the posterior wall 1–2 cm below the bifurcation, where the vessel is usually at right angles to the ultrasound beam. The internal carotid artery is more difficult to evaluate because in many cases the vessel tilts away from the transducer surface. A minimum of three measurements are taken on a 1 cm segment at the top of the CCA. Automatic edge detection systems are available in some ultrasound systems, but with careful attention to detail it is possible to measure intima-media thickness manually with satisfactory reproducible accuracy. The exact upper limit of the normal range is the subject of some debate.
IMT is known to vary by age, sex and race, but values less than 0.8 mm correlate well with the absence of coronary artery disease, while increases in thickness above this level are associated with increasing severity of coronary artery disease, increased risk of heart attack myocardium, as well as stroke.
After both carotid arteries have been examined, the vertebral arteries are evaluated on ultrasound. The vertebral artery on each side is the first branch of the subclavian artery. It passes posteriorly and upward to the vertebral foramen in the transverse process of the sixth cervical vertebra (segment V1), and from there it passes upward along the spinal canal to the level of the axis (C2 - V2 segment). It then leaves the spinal canal at the C2 cervical vertebra, passes beyond the lateral region of the atlas (C1) and enters the skull through the foramen magnum (segment V3) and passes in front of the brain stem (segment V4), connecting with a vessel on the other side in front of the brain stem. to form the main artery.
The vertebral arteries are most easily located by placing the transducer longitudinally over the common carotid artery and angling it midway to identify the vertebral bodies. The transducer is then rotated laterally so that the transverse processes of the vertebrae and the spaces between them are visualized, in which the vertebral artery and vein can be seen. If the vertebral artery cannot be identified in the spinal canal, it can be looked for in the lower neck as it runs posteriorly from the subclavian artery to the top of C6; or in the upper part of the neck behind the mastoid process as it passes around the atlas (C1) and enters the foramen magnum.
There may be marked differences in the size of the vertebral arteries and their relative contribution to basilar artery blood flow. When there are differences in size on ultrasound, the left artery is usually larger than twice the size of the opposite right one, and in 7–10% of people there are significant segments of hypoplasia, resulting in the artery not being visible at all. Clear visualization of the vein, but not the artery, suggests that the artery may be either thrombosed or congenitally absent. Color Doppler makes a direct assessment of low resistance and underground direction in the vertebral arteries. They should have the same color as the common carotid artery in front of them. Caution must be exercised when diagnosing reversal flow, especially if the spectral Doppler waveform was inverted during the study. If subclavian steal syndrome is suspected, it is worth making sure that the machine is set up properly to avoid misdirection of blood flow.
When diagnosing many diseases, doctors resort to the use of ultrasound (ultrasound). This informative method of examination allows you to study the state of the circulatory system that supplies the head. This examination is both planned and unscheduled.
Vertebral artery diameter is normal in adults
To determine the degree of stenosis, you need to know the criteria for the normal condition of the carotid arteries:
- In case of occlusion (complete obstruction of the vessel), blood flow is not recorded.
- The first degree of stenosis above 50% is characterized by a maximum blood flow velocity in systole of 125-230 cm per second.
- Stenosis above 70% has a velocity of 230 cm per second and higher.
- The third degree of stenosis (90% and above) is characterized by a narrowing of the lumen of the vein and a reduced speed of blood flow through it.
- The norm is considered to be a systolic blood flow velocity of no more than 125 cm per second. In this case, there should be no plaques or seals from the inside of the vessel.
Additionally, the presence of vascular problems can be determined by calculating the ratio of the maximum systolic blood flow velocity in the common and internal arteries. In the presence of stenosis, this figure will exceed the norm by more than three times.
This diagnosis is especially important for patients with reduced left ventricular ejection fraction (weak or incomplete compression of the heart) or with heart failure. The same principle requires measuring the pressure in both arms before performing an ultrasound.
The common carotid artery is a major vessel that transports blood from the heart to the uppermost part of the human body.
It is this artery, along with its branches, that supplies the brain with 70% of the blood it needs. Eyes, back of the head, ear region, jaw and temporal glands, muscles of the face and tongue.
A wide network of branches of the carotid arteries extends through all tissues and organs concentrated in the head area.
The carotid glomus, located in the bifurcation area, is a small body. Its length is 2.5 and its width is 1.5 mm. Its second name is carotid paraganglion. This is an important element due to the fact that the glomus contains a developed network of capillaries and a mass of chemoreceptors (elements of human sensory systems).
Thanks to specific formations, the glomus reacts to fluctuations in the concentration of oxygen in the blood, as well as carbon dioxide and hydrogen ions. Using this data, he monitors blood composition, pressure stability and the intensity of the heart muscle.
The carotid sinus, an enlarged area at the bifurcation site, also has structural features. Its middle shell is poorly developed, but the outer shell is quite dense and thickened. A huge number of elastic fibers and nerves are concentrated here.
Such a simple procedure as an ultrasound examination of the neck vessels helps to find out how well the brain is supplied with blood. For its normal operation, a complete blood supply is necessary. This is how nutrients and oxygen are delivered to the brain, and the return flow of blood through the veins is also important.
To obtain a clear image of the vascular wall in B-mode, a high-frequency linear sensor of more than 7 MHz is required: sensor resolution of 7 MHz is 2.2 mm, 12 MHz is 1.28 mm. If the ultrasound beam is oriented perpendicular (90°) to the vessel wall, maximum reflection and echo intensity will be obtained in the image.
Atherosclerosis is expressed in the infiltration of vessel walls with lipids, with the subsequent development of connective tissue thickenings - atherosclerotic plaques (AP). Atherosclerosis often develops in the ostia and bifurcations, where laminar blood flow is divided and disrupted.
Photo. In the carotid sinus, at the outer wall, a zone of spiral flow is observed, which in the color flow mode is colored blue along with the red laminar flow along the main axis of the ICA. This is the so-called flow separation zone. ABs are most often formed in this zone. Sometimes large plaques without stenosis are found here.
In the early stages of atherosclerosis, thickening of the intima-media complex (IMC), heterogeneity of the echostructure, and undulation of the contour are determined.
Photo. To measure IMT in the distal part of the CCA, it is necessary to draw two clearly visible hyperechoic lines at the border between the lumen of the vessel and the intima, as well as the media layer and the adventitia (arrows). An example of automatic CMM thickness measurement is shown.
On longitudinal and transverse sections, the localization of plaques is determined: concentric or eccentric; anterior, posterior, medial or lateral.
All AB classifications are based on echogenicity and homogeneity of echostructure:
- Homogeneous with a smooth surface - considered stable and have a favorable prognosis.
- Calcified - have hyperechoic inclusions and acoustic shadowing behind.
- Heterogeneous with zones of different echogenicity, as well as hypoechoic with dense inclusions and “niche” type formations are considered unstable and can lead to vascular disasters due to vascular thrombosis and embolic complications.
Photo. In the CCA, the AB has a smooth and even contour, isoechoic, and heterogeneous. On a longitudinal section, a hyperechoic linear structure with an acoustic shadow behind is determined - calcification; on a transverse section, a focus of reduced echogenicity is determined in the center of the plaque - possibly hemorrhage.
Photo. In the CCA, AB with a smooth surface, heterogeneous: on the left - hypoechoic, on the right - isoechoic with a hyperechoic linear structure and an acoustic shadow behind (calcification).
Photo. Hypo- (C, D) and isoechoic (B) plaques, as well as hyperechoic plaques with an acoustic shadow (A) are difficult to distinguish in B-mode. Use color flow control to detect fill defects.
Pathological tortuosity of the great vessels of the neck is often a consequence of atherosclerotic damage to the vessel walls. There are C-shaped, S-shaped and loop-shaped forms of tortuosity. Tortuosity can be hemodynamically insignificant or significant. Hemodynamically significant tortuosity is characterized by the presence of turbulence of blood flow in places of an acute or right angle.
- NASCET (North American Symptomatic Carotid Endarterectomy Trial) - the degree of stenosis is calculated as the ratio of the difference in the diameter of the ICA distal to the site of stenosis to the value of the free (from intima to intima) lumen of the vessel in the area of stenosis, expressed as a percentage;
- ECST (European Carotid Surgery Method) - the degree of stenosis of the CCA bifurcation is calculated as the ratio of the difference in the maximum (from adventitia to adventitia) and free (from intima to intima) lumen of the vessel in the area of stenosis to the value of the maximum diameter of the vessel, expressed as a percentage;
- CC (Common Carotid) - the degree of stenosis is calculated as the ratio of the difference in the diameter of the CCA proximal to the site of stenosis and the size of the free (from intima to intima) lumen of the vessel in the area of stenosis to the diameter of the CCA, expressed as a percentage;
- The degree of stenosis is also determined as the ratio of the area of the passable section of the vessel (from intima to intima) to its total area (from adventitia to adventitia) on a cross section.
To determine the degree of stenosis, there must be increased velocity through the narrowed segment and poststenotic abnormalities distal to the stenosis. The highest speed is used to classify the degree of constriction. PSV are leading in the classification of ICA stenosis. If necessary, additional parameters are taken into account - the ratio PSV BCA/OCA, EDV.
Table. Doppler criteria for determining the degree of ICA stenosis. For the ICA/CCA PSV ratio, use the highest PSV from the origin of the ICA and the highest PSV from the CCA (2–3 cm proximal to the bifurcation).
Stenosis degree (%) PSV (cm/sec) EDV (cm/sec) VCA/OCA PSV ratio
| Norm | {amp}lt;125 | {amp}lt;40 | {amp}lt;2.0 |
| {amp}lt;50 | {amp}lt;125 | {amp}lt;40 | {amp}lt;2.0 |
| 50-69 | 125-230 | 40-100 | 2.0-4.0 |
| ≥70 | {amp}gt;230 | {amp}gt;100 | {amp}gt;4.0 |
| Close to occlusion | Variable | Variable | Variable |
| Complete occlusion | Absent | Absent | Not defined |
In the presence of contralateral ICA occlusion, the velocity on the ipsilateral ICA may be increased. To avoid overestimation of ICA stenosis, new rate criteria have been proposed. PSV greater than 140 cm/sec are used for {amp}gt;50% stenosis and EDV greater than 155 cm/sec for stenosis greater than 80%.
Photo. PSV in the left CCA is 86 cm/sec. On the left ICA, the maximum PSV is 462 cm/sec, EDV is 128 cm/sec. The PSV ratio of BCA/CCA is 5.4. Stenosis of the left ICA is 70-79%.
Photo. In the ICA, the maximum PSV is 356 cm/sec, EDV is 80 cm/sec. Stenosis of the left ICA is 50-69%.
Photo. In the ICA, the maximum PSV is 274 cm/sec, EDV is 64 cm/sec. Stenosis of the left ICA is 50-69%.
Photo. In the VCA, the maximum PSV is 480 cm/sec, EDV is 151 cm/sec. Stenosis of the left ICA is close to occlusion.
- High PSV (135 cm/sec) in both CCAs may be due to high cardiac output in hypertensive patients or young athletes.
- Low PSV (less than 45 cm/sec) in both coCAs is likely to be secondary to decreased cardiac output from cardiomyopathies, valvular disease, or large myocardial infarction.
- In patients with cardiac valve insufficiency and regurgitation, the proximal spectrum of OCA has a very low EDV.
- In arrhythmias, PSV will be low after premature ventricular contraction; after a compensatory pause, PSV will be high.
The distinction between occlusion and near-occlusion is important: severe narrowing may benefit from surgical treatment, but complete occlusion may not.
With almost or complete occlusion of the OCA, the direction of flow in the ECA changes. The apparatus must be configured to detect low flow rates. To achieve this, an appropriate Pulse Repetition Frequency (PRF) must be provided. In case of almost occlusion, a “string sign” or a “trickle flow” is determined on the color circulation.
- AB fills the gap;
- there is no pulsation;
- near the occlusion there is reverse blood flow;
- there is no diastolic wave in the ipsilateral OCA.
When the ICA is occluded, the ICA becomes a bypass for intracranial circulation and may exhibit low persistence and manifest as ICA (internalized ICA).
The only reliable parameter for differentiation is the presence of branches of the NCA in the neck. Also, tapping on the superficial parietal artery affects the ESA spectrum.
Although, reflected flow from the superficial temporal artery can also be found in the SCA and OCA.
Why is it necessary?
Why is an ultrasound of the carotid artery performed? Using an ultrasound examination of the cervical region, the doctor examines the condition:
- spinal arteries;
- carotid arterioles (left and right external);
- carotid arterioles (left and right internal);
- carotid arterial vessels (left and right common);
- arteries of the subclavian region (left from right);
- brachiocephalic trunk.
An experienced diagnostician identifies their diameter, size, blood flow speed and general condition. In addition to them, the mandatory examination area includes:
- arterioles of the eyes;
- arteries of the supratrochlear zone;
- vertebral plexus with its veins;
- jugular veins.
Ultrasound of the vessels of the neck allows you to carefully examine this area for the presence of:
Now it’s clear why an ultrasound scan of the neck is done, and how is the information received deciphered?
Interpretation of vascular ultrasound
In order to correctly interpret the results of ultrasound of the vessels of the brain, you should know the normal indicators. During the examination, several characteristics of the arteries are studied:
- Presence of tortuosity - if ultrasound shows an abnormal course of the vessel (the presence of kinks, tortuosity), most often this indicates the presence of an atherosclerotic lesion (plaque formation);
- Vessel diameter - this parameter reflects the adequacy of blood flow through the artery. A pronounced narrowing of the vessels of the cerebral apparatus on ultrasound can lead to insufficient oxygen supply to the tissues and the development of severe pathology (vertebral artery syndrome, ischemic stroke, transient attacks, and so on). Normal diameters of neck arteries:
- Vertebral (VA) – 3.5 mm;
- General carotid (CA) – 5.5 mm;
- Internal carotid (ICA) – 4.6 mm;
- External carotid (ECA) – 3.7 mm.
When deciphering, it should be remembered that a deviation within 0.5 mm is possible, since the size of the vessels may have individual characteristics.
- The presence of plaques is normal; the lumen of the artery should be completely patent. If it is narrowed/completely “clogged” by an atherosclerotic plaque or thrombus, symptoms of cerebral circulatory failure may occur. Therefore, when identifying these formations on ultrasound of the vessels of the head and neck, the degree of narrowing should be assessed:
| II | At 41-65 |
| III | At 66-95 |
| Occlusion (complete blockage) | At 100 |
- Blood flow speed - during an ultrasound of the vessels of the head, the speed of blood flow through the main arteries is necessarily measured. The assessment is carried out in two phases of heart activity: systole (when the ventricles contract, causing a pulse wave) and diastole (the moment the heart relaxes and the valves close). When deciphering an ultrasound of cerebral vessels, the following indicators should be considered normal:
| Artery | Vps – blood flow velocity in systole (cm/sec.) | Ved – blood flow velocity in diastole (cm/sec.) |
| Vertebral (PA) | 73 | 18 |
| General carotid (CAS) | 62 | 20.5 |
| Internal carotid (ICA) | 68 | 14 |
| External carotid (ECA) | 41.5 | 12 |
| Possible deviation | 15 cm/sec up or down | 5 cm/sec up or down |
Taking into account all these indicators, after decoding it is possible to draw an adequate conclusion about the condition of the vessel.
Ultrasound of the arteries of the head, which include the carotid and vertebral arteries, are of great diagnostic importance. Currently, this ultrasound examination is done to determine the cause of brain dysfunction and choose treatment tactics. If ultrasound does not show any abnormalities, additional examination of the overlying parts of the vascular system should be performed.
Source: uzigid.ru
What do the diagnostic results say?
Normally, interpretation of the ultrasound of this zone provides the following information:
- The narrowing of blood vessels in the cervical region is more than ninety percent. At the specified percentage of narrowing of the arteries in a person, various forms of stenosis are diagnosed. In the described state, a person’s blood flow rate decreases.
- The narrowing of the vascular lumen is more than seventy percent. In this state, a person’s blood flow speed is more than two hundred and thirty centimeters per second.
- Narrowing of the vascular lumen by half. Decoding such information comes down to a blood flow rate of no more than two hundred and thirty centimeters per second. Most often, this narrowing is formed due to the presence of characteristic plaques.
- No narrow zones on the vessels. In the absence of narrow areas on the vessels, doctors diagnose a normal, healthy result. In this case, the linear speed of blood flow through the internal carotid arteries is no more than one hundred and twenty-five centimeters per second. Thickenings with plaques are not visible on them.
If an occlusion is detected, blood flow is not formed. When examining this area of the body, the doctor pays attention to the ratio of the peak systolic blood velocity in the internal vessels to the common carotid arteriole.
What does an ultrasound of the neck show? This procedure allows you to determine the diameter of each vascular lumen.
If it is not blocked by foreign objects (plaques), then arterial blood flow will have an adequate speed. With vascular constriction, incomplete oxygen saturation of brain cells is diagnosed, against which many diseases can develop.
The following values are considered to be the normal sizes of the diameter of the cervical arterioles:
The normal value of the linear velocity of blood flow through the carotid arteries depends on the age characteristics of the patient and general health.
What does cervical vascular narrowing look like?
The size of the cervical vessels may deviate from the norm, which is the result of disruptions in metabolism or the appearance of disturbances in the structure of the body. Over a long period of time, such changes are imperceptible; the boiling point is the cerebral blood supply. As soon as the nutrition of the head cells ceases to be complete, a person experiences characteristic pain.
The development of degenerative-dystrophic diseases in the neck occurs with damage to the vertebral artery, which passes through the vertebral lumens at the transverse vertebral processes.
The formation of osteophytes leads to compression of the vessel, against which numerous autonomic disorders develop.
The diameter of the vertebral arteries with atherosclerosis decreases, as the vascular lumens are filled with plaques. They are formed as a result of disruption of metabolic processes in the body.
Plaques form lipoproteins that are slowly deposited on the vascular walls, creating congestion. In this case, the vascular wall begins to be damaged, and an accumulation forms in this place:
- platelets;
- leukocytes;
- red blood cells
The listed blood cells form a blood clot, which is capable of fibrotization over time.
Deviation from the norm in the diameter of the vertebral arteries may be accompanied by the following pain manifestations:
- feeling of stiffness;
- manifestations of crunching;
- feeling of discomfort.
The described signs indicate vertebral osteochondrosis. Sudden movements of a person are always accompanied by pain, radiating to the arms and shoulder girdle. Against this background, muscle spasms may occur, limiting the mobility of the vertebrae in the neck. With osteochondrosis, the linear speed of blood flow through the vessels will be increased.
What does the pain in the head indicate? Headaches caused by narrowing of the cervical arteries have different manifestations and can be:
- tightening (muscle tension);
- dull (arteriospastic disease);
- bursting (liquorodynamic pathology);
- pulsating (arteriodilatatory disease);
- aching (vein disease).