Aortic stenosis is a narrowing of the lumen of the largest artery, resulting in incomplete patency of the structure, reflux of blood into the left atrium and disruption of local and then general hemodynamics.
Recovery is carried out surgically. It is necessary to distinguish narrowing from blockage or occlusion. As is the case with common atherosclerosis.
In the first situation, aortic stenosis occurs, in the second, mechanical obstruction as a result of the deposition of cholesterol plaques. Both are dangerous.
Surgical treatment is required. The prognosis depends on its timeliness and effectiveness. The specialist on whose shoulders the therapy falls is a cardiac surgeon.
Aortic stenosis has its own ICD-10 code - I35 with various postfixes.
The mechanism of pathology development
The essence of the condition is the narrowing of the mouth of the artery and the impossibility of further blood flow into the systemic circle.
The pathogenic process is caused by one or a group of external and internal factors.
A common option is regular inflammation of the pericardial structures, for example, rheumatism. As an autoimmune pathology, it is destructive. It flows constantly.
If relapses are frequent, the probability increases even more significantly. Congenital malformations, vasculitis (damage to the vessel wall itself) and other options are also possible.
Regardless of the type of process, a narrowing of the aortic mouth is observed at the point where it flows into the left ventricle. Blood is ejected from the chamber, passes the valve, but is not able to overcome the resistance. Therefore, only part of the liquid connective tissue gets into the large circle.
The other gets stuck in the cavity of the cardiac structures and causes overload of the heart. As it progresses, the volume of regurgitation (return) increases, possibly stretching the ventricle, developing dilation and secondary cardiomyopathy.
The mechanism for the development of dangerous consequences is clear:
- On the one hand, the heart intensifies its activity to provide the body with sufficient nutrients and oxygen. This is fraught with artificial growth of the muscle layer, as a way of compensation. Blood pressure and its indicators in the aorta itself also increase.
- On the other hand, organs and systems do not receive enough necessary connections. This ends with hypoxia, tissue degeneration and multiple organ failure.
Aortic stenosis. Hemodynamics, symptoms, diagnosis.
Aortic stenosis is a narrowing of the LV outflow tract in the area of the aortic valve, leading to difficulty in the outflow of blood from the LV and a sharp increase in the pressure gradient between the LV and the aorta.
The causes of acquired aortic stenosis are:
Rheumatic disease of the valve leaflets (the most common cause)
atherosclerosis of the aorta
endocarditis
· degenerative changes in valves with subsequent calcification.
Syphilitic aortitis and subsequent calcification
Hemodynamic changes
Due to narrowing of the lumen, Clinic. Stenosis of the aortic mouth is asymptomatic for a long time.
With significant narrowing of the valve orifice, the most typical complaints are those caused by the presence of a fixed stroke volume, relative coronary insufficiency and left ventricular failure:
- dizziness, fainting during exertion or rapid changes in body position;
- fatigue, weakness during physical activity;
- attacks of typical angina pectoris;
- shortness of breath on exertion and then at rest;
- in severe cases - attacks of suffocation (cardiac asthma or pulmonary edema).
The first complaints usually appear when the aortic mouth narrows to approximately 50% of its lumen. The symptoms are explained by the inability to adequately increase cardiac output during exercise and transient cerebral circulatory failure.
Over time, against the background of the described clinical manifestations of a fixed stroke volume, rapid fatigue and weakness during physical activity appear (insufficient perfusion of skeletal muscles, including due to vasoconstrictor vascular reactions).
Pain in the heart area appears during the period of compensation of the defect as a result of relative coronary insufficiency, which appears or worsens during physical activity. The pain is usually localized behind the sternum, radiates to the left arm and shoulder, and is relieved with nitroglycerin.
Inspection
During a general examination, attention is drawn to the characteristic pallor of the skin (“aortic pallor”), caused by a decrease in cardiac output and the tendency of peripheral vessels to vasoconstrictor reactions that arises against this background.
In the stage of compensation, when pronounced concentric hypertrophy of the LV myocardium predominates without expansion of its cavity, a sharply enhanced concentrated and slightly displaced apical impulse is noted. It is usually located in the 5th intercostal space along the midclavicular line. The boundaries of relative dullness of the heart are practically unchanged. Sometimes a “double” apical impulse is detected, caused by increased contraction of the left atrium.
In the stage of decompensation, which is characterized not only by diastolic dysfunction, but also by a decrease in myocardial contractility, dilatation of the LV cavity is observed. Upon palpation, an enhanced apical impulse is determined, located in the V-VI intercostal space outward from the left midclavicular line. The left border of the relative dullness of the heart is shifted to the left.
In addition, with significant narrowing of the aortic valve orifice at the base of the heart, systolic tremors are often detected by palpation, caused by low-frequency vibrations formed when blood passes through the narrowed valve orifice. Systolic tremor can also be detected in the jugular notch and in the carotid arteries.
In typical cases, aortic stenosis is characterized by a rough, intense systolic murmur in the aortic auscultation zone and often a weakening of sounds 1 and 2.
Blood pressure. In the initial stages of the disease, arterial pulse and blood pressure are practically unchanged. With significant narrowing of the aortic valve, the pulse becomes small, low and rare (pulsus parvus, tardus et rarus). The slowing of the heart rate is a kind of compensatory mechanism that ensures more complete expulsion of blood through the narrowed opening of the aortic valve.
With severe aortic stenosis, a decrease in systolic and pulse blood pressure is observed, which reflects hemodynamic changes characteristic of the defect (decreased cardiac output).
Moist rales in the lungs indicate that the patient has left ventricular failure and blood stagnation in the pulmonary circulation.
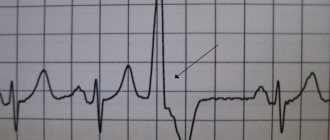
The ECG can remain constant for a long time. Later, deviations of the electrical axis of the heart to the left and other signs of left ventricular hypertrophy are detected: an increase in the R wave, a decrease in the ST segment, a change in the T wave in the left precordial leads.
Echocardiography reveals thickening of the aortic leaflets and a decrease in the systolic divergence of the valve leaflets during systole.
Ticket22
1. General palpation of the patient. Palpation is a research method using touch in order to study the physical properties, sensitivity, and topography of human organs.
To determine body temperature, hands are placed flat on the torso and limbs, on symmetrical joints. The pulse is examined by palpation, pressing fingers to the place where the artery runs, and the character and quality of the pulse are assessed. The lymph nodes are palpated and assessed. Palpation is used to determine vocal tremor. Palpation of the abdominal organs plays a huge role. Special palpation techniques are used in gynecological and urological practice.
There are superficial and deep palpations, palpation of painful points. There are also bimanual, balloting palpation, deep sliding palpation according to Obraztsov and Strazhesko.
2. Dry pleurisy. This is an inflammation of the pleura. Etiology: infectious, with lobar pneumonia, tuberculosis, allergic. Pathogenesis: fibrinous exudate covers the layers of the pleura, they become rough, desquamation of the mesothelium occurs, and exposure of nerve endings occurs. Clinic: pain, intensifies on inspiration (forcing the patient’s position on the sore side to reduce the excursion of the diseased lung), low-grade fever, dry painful cough. Inspection: limited mobility of the GR on the affected side. Percussion: decreased mobility of the lower edge. Clear lung sound. Ausk: Vesic breathing + pleural friction noise, intensifies when pressed with a stethoscope. The voice trembles and bronchophony does not change. Dry pleurisy can turn into exudative. 3. Aortic valve insufficiency. Hemodynamics, symptoms, diagnosis.
Aortic valve insufficiency is characterized by incomplete closure of the valve leaflets during diastole, which leads to reverse diastolic blood flow from the aorta to the LV.
The most common causes are: Rheumatism (about 70% of cases); Infective endocarditis; Atherosclerosis Syphilis Lupus endocarditis
Aortic valve insufficiency causes a significant portion of the blood ejected into the aorta to regurgitate back into the left ventricle during diastole. The volume of blood returning to the left ventricle can exceed half of the total cardiac output.
Thus, with aortic valve insufficiency, during diastole the left ventricle fills as a result of both blood flow from the left atrium and aortic reflux, which leads to an increase in end-diastolic volume and diastolic pressure in the left ventricular cavity.
As a result, the left ventricle enlarges and significantly hypertrophies.
Mitralization of the defect is the occurrence of relative mitral valve insufficiency with significant dilatation of the LV. “Mitralization” of aortic valve insufficiency leads to regurgitation of blood from the LV to the left atrium, expansion of the latter and a significant worsening of stagnation in the pulmonary circulation.
Hemodynamics: Compensatory eccentric hypertrophy of the LV (hypertrophy + dilatation), which occurs at the very beginning of the formation of the defect. Signs of left ventricular systolic failure, blood stagnation in the pulmonary circulation and pulmonary hypertension developing during decompensation of the defect.
Some features of blood supply to the arterial vascular system of the systemic circulation: - increased systolic blood pressure; - decreased diastolic blood pressure; -increased pulsation of the aorta, large arterial vessels, and in severe cases - arterioles; disruption of nutrition of peripheral organs and tissues due to a relative decrease in effective cardiac output and a tendency to peripheral vasoconstriction. Relative insufficiency of coronary blood flow (due to low diastolic pressure in the aorta, LV hypertrophy)
Clinic One of the first clinical manifestations of the disease is an unpleasant sensation of increased pulsation in the neck, in the head, as well as increased heart beats (patients “feel their heart”), especially in a lying position. These symptoms are associated with high cardiac output and pulse pressure in the arterial system. These sensations are often accompanied by a rapid heartbeat. With a significant defect in the aortic valve, the patient may experience dizziness, fainting, condition. impaired cerebral perfusion.
The pain is usually localized behind the sternum, but often differs in nature from typical angina. The pain often occurs at rest and is of a pressing or squeezing nature, usually lasts quite a long time and is not always well relieved with nitroglycerin.
The period of decompensation is characterized by the appearance of signs of left ventricular failure. Shortness of breath first appears during physical activity, and then at rest. With a progressive decline in LV systolic function, shortness of breath becomes orthopnea. Then it is joined by attacks of suffocation (cardiac asthma and pulmonary edema). Characteristic is the appearance of rapid fatigue during exercise and general weakness.
During a general examination of patients with aortic insufficiency, first of all, attention is drawn to the pallor of the skin, indicating insufficient perfusion of peripheral organs and tissues.
With a pronounced defect of the aortic valve, systolic-diastolic pressure drops in the arterial system can be detected:
· increased pulsation of the carotid arteries (“carotid dance”), as well as visible pulsation in the area of all superficially located large arteries (brachial, radial, temporal, femoral, artery of the dorsum of the foot, etc.);
· de Musset's symptom - rhythmic rocking of the head back and forth in accordance with the phases of the cardiac cycle (in systole and diastole);
· Quincke's symptom (“capillary pulse”, “precapillary pulse”) - alternating redness (in systole) and blanching (in diastole) of the nail bed at the base of the nail with sufficiently intense pressure on its tip. Quincke is detected by pressing on the lips with a glass slide;
Landolfi's symptom - pulsation of the pupils in the form of their narrowing and dilation;
Muller's sign - pulsation of the soft palate.
Typical auscultatory signs of aortic insufficiency are diastolic murmur on the aorta and at Botkin's point, weakening of the second and first heart sounds, as well as systolic murmur on the aorta of a functional nature. Flint's functional diastolic murmur is a presystolic murmur of functional stenosis of the left atrioventricular orifice, which is occasionally heard in patients with organic aortic valve insufficiency. Durosier's symptom Double Traube ECG tone: a rotation of the electrical axis of the heart to the left, an increase in the R wave in the left chest leads, and, subsequently, a downward displacement of the ST segment and inversion of the T wave in the standard and left chest leads are detected.
In cases of aortic valve insufficiency, clear radiological signs of LV dilatation are usually detected. On ECHO, the end-diastolic size of the left ventricle is increased
Ticket 23
1. Palpation, percussion and auscultation of a patient with pathology of the urinary system. Palpation - bimanual, left hand on the lower back, right hand pressing the kidney to the back of the chest. Normally, the lower pole of the right kidney is not palpable, but in asthenic patients the lower pole of the right kidney is palpable. Palpable when increasing or decreasing. Degrees of nephroptosis (omitted): 1) palpation of the lower pole of the kidney 2) palpation of the entire kidney 3) palpation of the entire kidney and is displaced. For ascites - ballistic palpation of the kidneys. Penetrating palpation - ureteral points, revealed pain. Effleurage (from Pasternatsky) - revealed pain. Percussion: Define the upper border of the bladder. When it overflows, a transition from tympanic to dull sound occurs. Ausk: Listening to a systolic murmur over the renal artery indicates its sclerosis.
2. Respiratory failure. DN is a condition in which there is insufficiency of the external respiration function to ensure complete gas exchange. Etiology: emphysema, asthma, pneumo and hydrothorax, etc. Classification: 1) pathogenetic: obstructive (BA, bronchitis, emphysema, foreign bodies), restrictive = reduced breathing volume (pneumonia, tuberculosis, tumor, hydro, pneumothorax), mixed. 2) By severity: 0 – no manifestations. 1 - manifested during physical activity; 2 - during minimal physical activity; 3 - at rest. The main manifestation is shortness of breath,
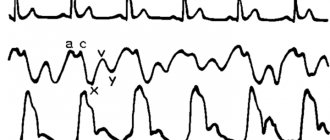
3. Mitral stenosis. Narrowing of the left AV foramen. Etiology: rheumatic endocarditis, sclerodegenerative changes, infective endocarditis. Hemodynamics: During atrial systole, the blood does not have time to completely move into the LV, some of the blood remains in the LA. At the same time, a new portion of blood enters the LA from the pulmonary veins -> dilatation and hypertrophy of the LA, pressure in the pulmonary circle increases (Kitaev reflex: part of the blood is discharged through arterioventriculus shunts), heat on the RV increases, and tricuspid insufficiency is formed. Complaints: shortness of breath during exercise, then at rest, interruptions in the heart (arrhythmia, pre-fibrillation), cough, hemoptysis, general complaints, with decompensation of the defect - edema (ascites, maybe anasarca) Inspection: Diffuse cyanosis of ashen color Facies mitralis (bogro-red butterfly – bridge of the nose + cheeks), pulsation of the jugular veins, swelling. Percussion: shift up, left, slightly right. Palp: arrhythmic pulse, on the left ray of the artery may be weaker or absent, frequent; Diastolic tremor (cat purring); Nesterov’s sign of “2 hammers” (alternating pulsation at the apex and base of the heart), cardiac impulse with decompensation Ausk: 1 sound at the top of the heart, loud clapping (calcinated cusps, thin LV wall, low hemodynamics), systolic pause, normal 2 tone, hz 0 .02 sec mitral click, diastolic rough murmur à quail rhythm. 3rd point (2nd m/r on the left) – emphasis of the 2nd tone on the pulmonary artery.
X-ray: mitral heart, waist smoothed. ECG: signs of HLP: 1 2 V1 V2 – double-humped P, increased 2nd phase. ECHO: ejection fraction reduced à loss of consciousness.
Ticket number 24.
1. Comparative percussion of the lungs. Characteristics of clear pulmonary sound, the mechanism of its formation. Mechanisms of change in percussion sound over the lungs.
The goal is to identify sound equivalents of lung tissue deformation (seals, voids). The study is carried out sequentially: the apexes, the anterior surface of the lungs - along the intercostal spaces, the lateral surfaces - along the middle axillary lines, the posterior surface - in the suprascapular areas, in the interscapular space and below the angle of the scapula along the scapular line.
Percussion produces 3 types of percussion tone:
- clear pulmonary - obtained by percussion directly behind the chest lies unchanged lung tissue, a clear pulmonary sound occurs with normal air content in the lungs, normal tension of the pulmonary tissue and with normal thickness of the integument, a clear pulmonary sound in its periodicity is oscillatory movements (this is due to the presence of elastic tension lung tissue), strength and height vary depending on a number of conditions: age, properties of the chest, muscle development, size of the subcutaneous fat layer;
- a dull or dull tone occurs during percussion wherever dense parenchymal organs are adjacent: liver, heart, spleen, in pathological conditions it is observed when the airiness of the lung decreases, as a result of filling the pleural cavity with fluid or complete tissue formations; airiness also decreases with its inflammation and filling of the alveoli with exudate, in case of collapse (atelectasis) of the lung due to blockage of the adductor bronchus or compression of the lung from the outside, in case of hemorrhage into it, in the presence of a large cavity filled with liquid contents in the lung, in case of a lung tumor; pleurisy, the formation of massive moorings, the development of a pleural tumor lead to the appearance of a dull percussion sound;
- tympanic tone is determined where cavities containing air are located directly close to the chest; under normal conditions, it is determined on the lower left (in the semilunar space of Traube); in pathology, it occurs when cavities containing air are formed in the lungs (cavity, abscess), and when air accumulates in the pleural cavity (pneumothorax).
Dull-tympanic tone - with a decrease in the airiness of the lung tissue, its normal elastic tension decreases - observed with inflammation of the lungs, when relaxation of the lung tissue occurs due to infiltration, with exudative pleurisy over exudate, with simultaneous filling of the alveoli with air, when other alveoli have not yet been completely freed from exudate , which is observed in stages 1 and 4 of lobar pneumonia, with pulmonary edema.
Box tone is a loud percussion tone with a tympanic tint, when the elastic tension of the lung tissue decreases and airiness increases (with emphysema, during an attack of bronchial asthma).
Based on the moment of development
- Congenital appearance. Relatively rare. Combined with a group of concomitant cardiac and other pathologies. The cause appears to be a developmental defect.
- Acquired form. It especially often affects young people under the age of 30. Then the disease progresses steadily, not making itself known until the anatomical defect stabilizes.
Note:
As practice shows, a complete cure never occurs. There are chances to significantly prolong the patient’s life by starting therapy in the early stages (1-2). But total recovery will not happen.
Treatment of aortic stenosis in children
The use of conservative therapy does not eliminate this heart defect. However, it can alleviate its symptoms by improving blood circulation in the heart and eliminating congestion in the lungs. Neonatal aortic stenosis is treated with prostaglandins, which prevent the aortic duct from closing; diuretics to relieve pulmonary edema. Diuretics remove excess fluid from the body, but at the same time contribute to disruption of the water-salt balance.
Aortic stenosis in newborns can also be eliminated surgically. For this purpose, methods of balloon valvuloplasty, prosthetics and plastic surgery of the aortic duct are used. In each specific case, the method of surgical treatment is determined by a pediatric cardiac surgeon.
Causes
Factors in the development of the condition are multiple. Some are controlled in nature, others do not depend on the patient at all and exhibit pathogenic activity spontaneously.
What are these moments?
- Long-term smoking. Persons with physiological nicotine addiction get sick in 80% of cases. If you take a closer look at tobacco users, you will find that the vast majority suffer from aortic valve stenosis in the initial or advanced phases. The problem will make itself known later.
- Cholesterolemia. It has an indirect connection with the described pathological process. Atherosclerosis appears and a plaque forms. The following are possible options. At the time of treatment, damage to the vascular walls and provocation of inflammation are likely. This is especially typical for surgical intervention for calcification of lipid formations. This results in gross scarring of tissue and narrowing of the lumen. The likelihood of such an outcome is minimal, but it is present.
- Being male. According to studies, women suffer from aortic stenosis 5-6 times less often. Apparently, this is due to the activity of estrogens, which make it possible to better combat various types of negative factors that can affect the heart and blood vessels.
- Age group 60+. There are two peaks of incidence. Youth up to 30 and old age after 55. Risk categories should be regularly monitored by a cardiologist and undergo ECHO-CG at least once a year.
- Renal failure in the decompensation phase. The provocation of the pathological process in this case is not fully understood. The same effect develops against the background of dangerous pathologies of the paired organ of a destructive nature. Jades, etc. Excess renin, angiotensin-II, and aldosterone are produced. They artificially narrow the lumen of the aorta. The pathological mechanism is fixed, becomes stereotypical and exists constantly, making normal blood flow impossible.
- Inflammatory lesions of cardiac structures. Primarily endocarditis. Destruction of the inner shell. It has an infectious (bacterial, less often viral or fungal origin). Accompanied by scarring and tissue fusion. When the aorta is destroyed, epithelization of the walls occurs. Connective cells narrow the lumen and prevent blood from moving normally.
- Systemic lupus erythematosus.
- Rheumatism. Inflammatory pathology. Like the previous reason, it ends with the destruction of vascular tissue, the inner layer, that is, the endothelium. Recovery has controversial prospects due to the persistence of the autoimmune process.
- Anomalies in the development of cardiac structures and blood vessels, including the aorta itself. They are of congenital origin. They are not necessarily related to heredity or genetic abnormalities, but this is also possible. In the second case, in addition to stenosis, gross defects of cardiac structures are observed. There are additional deviations from connective, bone tissue and others.
- Calcifications. Deposition of inorganic salts in the cavities of blood vessels and on the surface of valves. The disease is of metabolic origin and is not associated with the consumption of the named microelement or drugs based on it. Bedridden patients and calcium reabsorption processes are mainly affected.
Some factors can be eliminated by the person himself as part of prevention. Others are treated with special methods, depending on the initial diagnosis.
Procedures and operations
Depending on the clinical condition of the patient, his age and the form of the defect, the method of invasive correction is selected. Contraindications for surgical intervention are stage I and IV stenoses.
Possible methods of surgical treatment:
- Balloon percutaneous valvuloplasty of the aortic valve - the operation is performed in infants with critical stenoses.
- Aortic valve valvuloplasty is an open heart surgery performed in children. Aortic valve replacement - the operation is performed for congenital pathology (dysplastic bicuspid, unicuspid aortic valve) and for patients after valvotomy with progressive stenosis. The prosthesis can be a pulmonary valve autograft, an aortic allograft, a porcine bioprosthesis, or a mechanical prosthesis.
- Konneau's operation - dilatation of the aortic root with valve replacement. Surgical treatment is performed for tunnel-shaped obstruction and severe stenosis.
- The Ross operation is an autotransplantation of the pulmonary trunk from the valves to the aortic position. Additionally, reconstruction of the outflow tract of the right ventricle is performed using a homograft. Surgical treatment is performed for children in the first year of life.
Symptoms
Depends on the stage:
Grade 1 aortic stenosis is characterized by complete or predominantly absence of manifestations.
Stage 2 is determined by the minimal clinical picture:
- Shortness of breath during moderate physical activity. It is observed in most cases as a consequence of disruption of normal gas exchange.
- Tachycardia. Acceleration of cardiac activity, increased contraction frequency.
- Increase in blood pressure. Not always, but in most cases.
- Dizziness. As a result of damage to cerebral structures, the inability to supply nervous tissue with blood (by the way, they are very sensitive to a lack of oxygen and nutritional compounds).
Stage 3 is the most common point of diagnosis:
- Shortness of breath occurs with minimal physical activity.
- Intense chest pain. Paroxysmal, no longer than 30 minutes. Typical for angina pectoris.
- Fainting, syncope. Different frequency and intensity.
- Nausea, vomiting.
Other manifestations are also present.
Stage 4 is determined by the same signs, but of greater strength. The same applies to the fifth stage.
Regardless of the phase of the pathological process, the following moments are observed:
- Paleness of the skin.
- Cyanosis of the nasolabial triangle. Blue discoloration of the area around the mouth.
- Increased sweating.
- Physical activity intolerance. Also called decreased tolerance.
When cerebral structures are damaged, a persistent neurological focal deficit is formed. It may be manifested by impaired coordination in space, speech, vision, hearing, swallowing, motor function and others.
Aortic stenosis in children: causes
The disease can manifest itself in the first days of a child’s life if the mouth of his aorta is less than 5 mm. With this parameter, by six months of life the baby’s health condition sharply deteriorates.
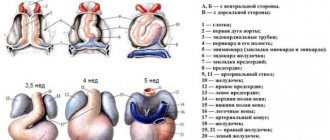
Congenital aortic stenosis occurs in the first trimester of the fetus’s gestation, and its development is facilitated by genetic predisposition, regular stress of the expectant mother, drinking alcohol or taking drugs prohibited during pregnancy. Williams syndrome in the fetus and the pregnant woman living in a dangerous environmental environment contribute to the development of this congenital pathology.
Diagnostics
Examination of patients with suspected aortic valve stenosis is carried out under the supervision of a cardiologist.
Approximate list of events:
- Oral questioning of the patient regarding complaints and their duration.
- Collection of anamnestic data. The main role is given to previously suffered pathologies of a cardiac, nephrogenic and endocrine nature. Lifestyle is also taken into account. The more bad habits, the greater the likelihood of deviation.
- Blood pressure measurement. Indicators may be elevated or normal. Also heart rate. At the time of an angina attack - acceleration of activity.
- Daily monitoring. As needed.
- ECG. To assess functional activity. Shows arrhythmias.
- ECHO-KG. Used to determine organic defects. The pressure in the chambers and the aorta itself is measured using the same method.
- Ultrasound of the kidneys. To identify nephrological conditions.
- MRI diagnostics.
As part of an extended examination, a blood test (general, biochemical, hormonal) may be required.
Activities are carried out in both inpatient and outpatient settings.
Treatment
Strictly surgical. The use of medications is practiced only in the early stages, as well as in preparing the patient for surgery.
List of drugs for aortic stenosis:
- Hypotensive. To correct blood pressure levels. There is a whole group of products with a similar effect.
- Antiplatelet agents. Aspirin-Cardio and others. To restore blood flow and make it easier to overcome stenotic areas.
- Medicines to normalize heart rate and rhythm in general. Amiodarone.
It is possible to prescribe other drugs as needed. The task of the preoperative period is to stabilize the patient’s condition and prevent complications at the time of intervention and immediately after it.
Radical treatment of aortic valve stenosis is carried out through prosthetics (replacement) or stenting of areas of narrowing at the initial stage.
- The first technique is indicated when it is impossible to restore the anatomical integrity and functional activity of the structure. The valve is replaced with a mechanical or biological one.
- The second concerns the installation of a special spring that prevents the lumen of the aorta from narrowing. Prescribed for supravalvular and subvalvular stenosis.
The choice of technique falls on the shoulders of the cardiac surgeon. In most cases there are no alternatives to replacing the valve or section.
Stages
Depending on the severity of hemodynamic disturbances, the following stages are distinguished during aortic valve stenosis:
- I (full compensation): symptoms of aortic stenosis can only be detected by listening to heart sounds or conducting instrumental studies for other diseases;
- II (latent heart failure): characterized by the appearance of complaints of increased fatigue and shortness of breath after physical activity and identification of signs of stenosis on ECG and Echo-CG (pressure gradient is 36-65 mm Hg), at this stage surgical intervention may be recommended interventions to eliminate stenosis;
- III (relative coronary insufficiency): accompanied by angina pectoris, increased frequency of fainting and worsening shortness of breath; at this stage, surgical intervention is recommended to eliminate the stenosis;
- IV (severe heart failure): shortness of breath and attacks of cardiac asthma also appear at rest, surgical correction at this stage is possible, but is accompanied by low effectiveness;
- V (terminal stage): complications may develop, a decrease in myocardial contractility rapidly increases and is accompanied by edema syndrome and cardiac asthma, at this stage only drug treatment can be undertaken, and surgery to eliminate stenosis is already contraindicated.
Forecast
A complete cure never occurs, as was said earlier. The outcome depends on the nature of the pathology, aggressiveness of the course, stage and other factors.
The possibility of radical intervention provides a good chance of success. According to statistics, survival among patients for 10 years is observed in 75-80% of cases.
Attention:
A longer lifespan is also possible. Clinical studies were not conducted, patients dropped out of the attention of doctors.
Progression, further development, correlates with the likelihood of death. The connection is proportional.
Emergency conditions worsen the overall prognosis, leading to a significant risk of fatal outcome.
Possible complications
Among the likely consequences of the pathological process:
- Heart attack. As a result of coronary insufficiency, which begins as early as stage 2 or a little later.
- Heart failure. Sudden death as a result.
- Cardiogenic shock. An absolutely lethal condition. Leads to death in 90-100% of cases. Recovery is hopeless.
- Vascular dementia. Similar in symptoms to Alzheimer's disease.
These conditions lead to death in most cases.