The main pump of our body - the heart - normally works unnoticed by us. We feel it only when it starts to fail. There are many heart diseases, and some of them (sick sinus syndrome, severe bradycardia, and others) may require a pacemaker. How to live after installation of an artificial pacemaker?
The heart is a muscular organ that pumps blood throughout the body. Any change in a person’s state (physical, emotional) is captured by the heart, and it changes the work (mainly in the form of an increase or decrease in heart rate) in accordance with the situation. This happens normally. If the heart is unhealthy, it cannot provide normal blood flow, and the person feels sick. For treatment, therapeutic and surgical treatment methods are used. The issue of installing a pacemaker to help a diseased heart deserves special attention.
A pacemaker (CS) is an electrical device whose main function is to “impose” the correct sinus rhythm on the heart. Diseases for which a pacemaker is installed:
- pronounced bradycardia - a decrease in the number of heart contractions (the norm is 60-80 contractions per minute);
- complete heart block, in which the atria and ventricles contract in an individual rhythm, independently of each other;
- severe heart failure;
— cardiomyopathies are diseases in which the contractile activity of the heart is disrupted due to structural changes.
Installation of a permanent pacemaker - a pacemaker - is a minor surgical intervention that is performed in the cath lab. The patient is given only local anesthesia in the surgical area. The purpose of the operation is to pass one or more electrodes through a vein into the chambers of the heart, followed by fixing the body of the pacemaker itself in the subcutaneous tissue of the chest. In Russia, right-handed people have stimulators implanted on their left side. Installation of the device on the right is carried out for left-handers in a number of other cases (for example, in the presence of skin scars on the left). However, the issue of placement of the device is decided in each case individually. The outer shell of the stimulator rarely causes rejection, since it is made of titanium or a special alloy that is inert to the body.
After installing a pacemaker, a person’s life, of course, changes: restrictions, new rules and requirements appear. But despite this, you can lead a full life with an artificial pacemaker. However, you need to understand that a pacemaker, even the most modern one, does not cure coronary artery disease, angina pectoris, or arrhythmia. This is not a new heart. The heart remains the same, so it must be spared.
Pacemaker - what is it?
A pacemaker is a device that takes on the role of a pacemaker. That is, it sets the heart to the correct rate when its sinus node is damaged, or the atria and ventricles work in an independent mode due to conduction blockade.
The pacemaker imposes the desired rhythm, and modern devices can also analyze the work of the heart. They stimulate it only when necessary - on demand. During installation, specialists perform individual configuration of the device.
We recommend reading about how to treat sinus bradycardia. You will learn about the causes of sinus bradycardia, symptoms, treatment and diagnosis of pathology. And here is more information about the drug treatment of ventricular tachycardia.
Contraindications
As with any procedure, pacemaker implantation must be done selectively depending on the condition of the individual patient. There are situations when the installation of a CS is not as useful as expected, or there are not enough indications for its use. They are sometimes also referred to as class III indications in ACC/AHA/HRS guidelines or European Society of Cardiology guidelines.
- Sinus bradycardia without significant symptoms; asymptomatic first degree AV block.
- AV block that is not expected to resolve or may recapitulate drug toxicity, Lyme disease, or transiently increased vagal tone.
- A pacemaker is not indicated for sinus node dysfunction in patients with symptoms suggestive of bradycardia that have been reported even in the absence of bradycardia.
- Asymptomatic Mobitz second degree, type I block.
- Asymptomatic prolonged RR interval with atrial fibrillation or other causes of transient ventricular pauses.
- Hypersensitive cardiac inhibitory response to carotid sinus stimulation in the absence of symptoms or in the presence of vague symptoms such as dizziness.
- Asymptomatic bradycardia during sleep.
- CRT is not indicated in patients whose functional status and life expectancy are limited primarily by noncardiac conditions.
- Right bundle branch block with left axis deviation without syncope or other symptoms consistent with intermittent AV block.
- Long QT syndrome or torsade de pointes due to reversible causes.
- The presence of an auxiliary pathway that has the ability for rapid anterograde conduction.
- Definition of class I or II symptoms and non-PVLP with QRS duration less than 150 ms.
Video: Pacemakers
4.67 Aug. rating ( 91 % score) – 3 votes – ratings
Purposes of pacemaker installation
Pacemakers are divided into temporary and permanent. The first ones are used when a short-term problem with the heart occurs, for example, arrhythmia appears against the background of acute myocardial infarction. If heart rhythm disturbances have become chronic, then a permanent CS is established. There are absolute and relative indications for long-term pacemaker implantation.
Absolute readings:
- • sick sinus syndrome;
- • symptomatic sinus bradycardia;
- • tachycardia-bradycardia syndrome;
- • atrial fibrillation with sinus node dysfunction;
Atrioventricular block - indication for installation of a pacemaker
- • complete atrioventricular block (third degree);
- • chronotropic incompetence (a condition in which the sinus node does not respond adequately to physical or emotional stress; even with maximum physical exertion, the heart rate does not exceed 100 beats per minute);
- • long QT syndrome;
- • cardiac resynchronization therapy with biventricular stimulation.
Relative readings:
- • cardiomyopathy (hypertrophic or dilated);
- • severe neurocardiogenic syncope.
Cardiomyopathy is one of the contraindications to the installation of a pacemaker.
Back in 1958, cardiac surgeon Ake Senning was the first to implant a cardiac pacemaker in a person.
Since then, the installation of a pacemaker has been considered the treatment of choice for the treatment of bradycardia and heart block. The number of operations performed is steadily growing. For example, the annual increase in implantation of conventional pacemakers in England is 4.7%, and cardiac defibrillator implantation - 15.1%.
Description of pacemakers
Since the invention of the first pacemaker, several significant improvements have been made. Additionally, a modern permanent pacemaker is a subcutaneously placed device. There are 3 types of artificial pacemakers:
- Implantable pulse generators with endocardial or myocardial electrodes.
- External, miniature, portable stationary, battery-powered, which are pulse generators with external electrodes for temporary transfusion endocardial or transthoracic myocardial stimulation.
- AC-powered cardioverters or monitors with high-current external transcutaneous or low-current endocardial or myocardial circuits for temporary pacing in asynchronous, manually or triggered pacing modes.
All pacemakers consist of two components: a pulse generator that provides the electrical impulse to stimulate the myocardium, and one or more electrodes/wires that deliver the electrical impulse from the generator to the myocardium.
The decision to introduce a pacemaker is usually based on symptoms of bradyarrhythmia or tachyarrhythmia. Symptomatic bradycardia is the most common indication.
Other symptoms that occur as a result of severe bradycardia include fatigue, decreased exercise capacity, and outright heart failure. Physiological sinus bradycardia, which is often detected in highly trained athletes, is not an indication for installation of an electrical pacemaker.
Heart pacemaker: pros and cons
The advantages of installing a pacemaker are reducing the risk of death from improper functioning of the heart, restoring normal heart rhythm, the ability to avoid disability, and restoring working capacity; disadvantages – slight restrictions in the usual way of life (it is necessary to avoid injuries, electromagnetic waves), rhythm disturbances, inflammatory reactions.
To evaluate the pros and cons of a pacemaker, you need to take into account that its implantation takes place according to health reasons. Therefore, refusing surgery can cost your life. The need is absolute for a slow heart rate that causes:
- dizziness;
- fainting conditions;
- attacks of shortness of breath;
- high blood pressure that cannot be relieved with medications;
- attacks of heart pain;
- swelling and enlargement of the liver;
- rapid fatigue during normal physical activity.
After installing a pacemaker, it is necessary to avoid exposure to high-frequency electric and magnetic waves and chest injuries. During operation of the device, rhythm disturbances and inflammatory reactions after implantation are possible.
Installation process
The pacemaker is implanted into the soft tissue under the skin in the area under the collarbone. Its wires are inserted into a large vein and advanced to the heart, where they are secured with prongs, hooks or small screws. Less commonly, the generator is placed under the skin of the abdomen.
The procedure is performed under local anesthesia, sedatives are used, and the patient is conscious. After the pacemaker is installed, its position is monitored using radiography. The duration of the procedure depends on the type of device and does not exceed 1 hour. The wound is sutured with absorbable sutures, so no stitches need to be removed. An immobilizing device is applied to the arm for 24 hours.
There are leadless pacemakers (without wires) that are inserted through the femoral vein and attached directly to the heart.
After implantation, the pacemaker is programmed - the base frequency, the maximum frequency at which the pacemaker can operate, and changes in the pacing rate during physical activity are determined. All this data is reflected in the device passport.
In what cases is a pacemaker placed on the heart?
A pacemaker should be placed on the heart if the heart rate is persistently slow. It is necessary when:
- bradycardia;
- weakness of the sinus node (the main pacemaker);
- blockade of impulses from the atrioventricular node.
All these conditions lead to the fact that the heart works with rare contractions, and the internal organs and brain do not receive the necessary nutrition. Patients may suffer from fainting conditions. If such episodes are frequent, then circulatory disorders of the brain and myocardium are possible. Surgery is usually recommended if medications do not have an effect, and the patient becomes unable to work or becomes disabled due to ineffective heart function.
How to live on after having a pacemaker installed. Recommendations
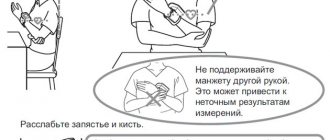
Despite the fact that the device is equipped with special built-in protection against the influence and interference of other electrical devices, you still need to avoid powerful electric fields. Do not be afraid of household appliances such as: microwave oven, tape recorder, vacuum cleaner, refrigerator, computer and the like.
It must be remembered that in order to prevent interference, the devices must be located at a distance of no closer than a decimeter from the area where the cardiac device is installed.
How to save your heart and the installed device
There are a number of rules that must be followed in everyday life:
- Do not touch the area where the cardiac device is installed to the operating TV.
- Do not lean against the front wall of the microwave oven.
- Do not stay near high-voltage power lines.
- Do not stand near welding equipment.
- Stay away from electric steel furnaces.
Remember not to go through security controls, both at airports and in stores. To avoid trouble, you should always have your cardiac device owner’s card and passport with you. The card can always be obtained at the hospital.
If an examination is prescribed such as: radiation therapy, diathermy, magnetic resonance diagnostics, external defibrillation, then first of all you need to inform the doctors that you have a pacemaker installed.
Fluorography and x-rays are not contraindicated. Sometimes radiography is prescribed if there is the slightest suspicion of electrode failure.
Doctors strongly recommend leading a healthy lifestyle after surgery. Watch your diet, engage in light sports, and spend more time outdoors.
Important! You should not sunbathe in the open rays of the sun. In hot weather, you should always wear cotton clothing on your body.
The battery in the device is designed to last for a decade. When the expiration date is approaching, the device will sound a signal. The signal will be recorded during a routine examination. The battery will be replaced immediately. Therefore, it is important to visit your doctor on time and regularly.
Emergency care for acute vascular insufficiency and treatment
Types of pacemakers
“Adaptation” to each type of heart rhythm disturbance prompted the development of various types of pacemakers and their modes of operation. All modern CS are capable of sensing the internal electrical activity of the heart and stimulating it only when the heart rate drops below a programmed level.
Essentially, they all have a built-in “sensor” that senses the need to change your heart rate in response to physiological needs.
For permanent cardiac pacing, three types of devices are used:
- ● single-chamber (PM-VVI) : the electrode is placed either in the right ventricle or in the right atrium;
- ● dual-chamber (PM-DDD) : two electrodes are installed (in the right ventricle and in the right atrium), this is the most common type of CS;
- ● three-chamber (PM-BiV) : used in so-called cardiac resynchronization therapy. As a rule, one electrode is implanted in the right atrium and in both ventricles. These pacemakers are usually installed in patients with chronic heart failure. They are able to “resynchronize” the work of the ventricles, which helps improve the pumping function of the heart.
- They are also called biventricular pacemakers. Cardiac resynchronization therapy may include implantation of a cardioverter-defibrillator.
Types of devices
Medical technology is constantly being improved, new models of pacemakers are being produced that are more reliable and effective. Now there are three types of such devices: one-, two- and three-chamber. Their choice depends on the severity of the patient’s heart rate problems and is determined individually by the doctor.
- Single-chamber devices are needed to stimulate the work of one chamber of the heart. They are usually installed for atrial fibrillation or sick sinus syndrome to improve the functioning of the right ventricle of the heart. Such devices can have a constant operating rhythm or regulate it depending on the patient’s physical activity.
- Dual-chamber pacemakers stimulate both the atrium and ventricle of the heart. They are needed for more serious pathologies of the sinus node. These devices help the heart work at a certain rhythm.
- Three-chamber pacemakers have a more complex structure and are installed mainly to relieve symptoms of severe heart failure. They synchronize the work of the ventricles of the heart and increase the force of its contractions.
- There are also special devices - cardioverters-defibrillators. They are needed to slow down the heart in case of severe tachycardia, which threatens the patient’s life. Such devices suppress an excessively rapid rhythm and normalize the condition of atrial fibrillation.
How does a pacemaker work?
The operating principle of new generation pacemakers is based on analysis of heart function. If the generated rhythm is lower than the set one (usually 60 beats per minute), there are pauses, then the device imposes a normal contraction frequency. There are also more advanced devices that change the activity of the heart when:
- physical activity;
- increased breathing;
- changing the duration of the intervals between contractions and relaxations of the ventricles (QT on the ECG);
- signs of fibrillation (chaotic contractions of muscle fibers) and other dangerous arrhythmias.
When working correctly, the pacemaker is capable of producing the desired rhythm for a long time, but testing is needed to check its functions. It is carried out at least once every six months in the department where the installation was carried out.
Pacemaker for atrial fibrillation
The need to install a pacemaker for atrial fibrillation occurs after cauterization. This procedure is called radiofrequency ablation. It allows radio waves to destroy the area of the myocardium that produces pathological signals. After it, there is a critical decrease in heart rate, which requires implantation of the device.
If after installation of a pacemaker there are rhythm disturbances, this means that its settings are not suitable for the patient. It is necessary to undergo testing and correction of the functions of the device in the department where the operation was performed.
How a pacemaker is installed: reviews
The effectiveness of such an operation is usually more than 80%. Most patients feel much better after it. This is a low-traumatic operation that rarely causes side effects and has almost no contraindications. But many patients have not very pleasant memories of the procedure itself, although it is performed under local anesthesia and no pain is felt. But there may be a feeling of pressure or even a slight burning sensation. Discomfort may also occur when connecting the electrodes. But usually the operation takes place without complications, the patient’s recovery does not last long, and after that he can lead a normal life.
Placement of a temporary pacemaker
To treat sudden blockade of impulse conduction or when contractions stop, temporary cardiac pacing is used. This may be necessary in case of acute circulatory disorders, myocardial infarction, poisoning with medications or toxic substances. Subsequently, the patient is fitted with a permanent device or prescribed medications to normalize the rhythm.
The essence of temporary stimulation is the introduction of an electrode through a vein to the right atrium and ventricle. Its outer end is connected to any stationary pacemaker. There is also the option of inserting a probe into the esophagus or using external electrodes.
Implantation technique
How is surgery to install a pacemaker performed? The procedure is performed in a specially equipped operating room under local anesthesia (general anesthesia is rarely used). It belongs to the category of minimally invasive surgical interventions.
Transvenous access to the chambers of the heart is used. That is, the wires (electrodes) coming from the pacemaker are placed intravenously.
To do this, the subclavian vein is most often catheterized. After which a small incision (3.8 - 5.1 cm) is made in the subclavian region, where a subcutaneous pocket is created where the pacemaker is implanted. Less commonly, the lateral saphenous vein of the arm is used for this purpose. Very rarely, access to the chambers of the heart is used through the axillary, internal jugular or femoral veins.
The guide catheter(s) are then inserted through a puncture in the vein into the right atrium. If necessary, a second catheter is sent along the same route and installed in another chamber. Or a puncture in another vein is used for this. After which the electrodes are directed through the conductors into the chambers of the heart.
Electrodes are attached to the endocardium (the inner lining of the heart) in two ways. Passive fixation - at the end of the electrode there is a hook that “clings” to the endocardium.
Active fixation - using a special fastening resembling a corkscrew, the electrode is screwed into the inner shell.
At the end of the procedure, specific tests are done to ensure the reliability of the installed pacemaker. Self-absorbing sutures are placed on the skin, and the arm is immobilized with a bandage for 24 hours.
How long the operation to install a pacemaker lasts will be influenced by its course and possible force majeure circumstances during the procedure. The CS implantation procedure itself, as a rule, does not exceed 3 hours. The duration of hospitalization is usually 24 hours.
Prevention of infectious complications with antibiotic therapy is mandatory. Cefazolin 1 g is usually prescribed. One hour before the procedure or alternatively 1 g of vancomycin in case of allergy to penicillin and/or cephalosporins.
The day after implantation, chest x-rays are performed to ensure that the electrodes and pacemaker are correctly positioned and that there are no possible complications (for example, pneumothorax).
To learn how to install a pacemaker, watch this video:
Pacemaker implantation in elderly people and its functioning.
How is a pacemaker placed in the elderly? The answer is obvious! Exactly the same as for young people. Installing a pacemaker at 80 years old is no different from installing a pacemaker at 20 years old. All the same stages that I have already described in more detail in one of the articles. Anesthesia with novocaine, incision and formation of a bed (pocket) of the pacemaker, installation of electrodes in the heart, connection of the pacemaker to the electrodes and suturing of the wound layer by layer (subcutaneous tissue, skin). But, of course, implanting a pacemaker in older people has its own peculiarities.
Reduced pain threshold.
Older people have a lower pain threshold. This means they feel pain more. This requires an increase in the dose of anesthetics, which, in old age, is more dangerous and undesirable. Older people are emotionally labile. They require more attention and communication. This is very important in the postoperative period, when it is important for the patient to understand what is happening and how to behave.
Flabbiness of tissues.
One of the main differences between the elderly and the young from a surgical point of view is tissue changes. What is called “flabbiness” of tissues. And this applies not only to the skin, but also to the subcutaneous tissue and muscles. This requires more careful work from the surgeon, since the skin is very easily “cut through” by the suture material. Due to the “flabby” heart muscle, when implanting electrodes, there is a higher risk of perforation of the heart wall by the electrode. This is a situation where the electrode can seem to pierce the wall of the heart. In addition, flabby tissue can contribute to the further development of the so-called Tweedler syndrome, or “twirler” syndrome. This is when the EX is too mobile in the bed and can rotate around its axis. The pacemaker “wraps” electrodes around itself. This can lead to dislocation - separation of the electrodes from the heart.
Medications.
Another difficulty is that older people tend to have several additional medical conditions. Often these diseases require the use of medications, which may affect the body during surgery. The main difficulty from this point of view is taking anticoagulants for atrial fibrillation, aspirin for ischemic heart disease, and antiplatelet agents after stenting. All these drugs inhibit blood clotting - coagulation, platelet aggregation. This increases the risk of bleeding during surgery and the risk of hematoma in the postoperative period. If the patient is taking warfarin (an indirect anticoagulant), then he is taken for surgery only if the INR (international normalized ratio) is 3 or less. If the patient's INR is higher, a reduction in the warfarin dose is required. For other anticoagulants and antiplatelet agents, there are no special criteria in terms of contraindications for surgery. However, their administration requires careful hemostasis during surgery.
Hardening and fatty degeneration of the heart muscle.
Another feature of tissues in old age is the replacement of muscles with fat and connective tissue. This process is called sclerosis, fatty degeneration. This plays a role in the implantation and attachment of electrodes to the heart wall. At this stage, the surgeon looks for an area of elastic contractile muscle. For some patients, this search may take a long time. If the heart muscle is sclerotic, this can increase the stimulation threshold. The pacing threshold is the minimum amount of electrical energy required to cause the heart to contract. Increasing the threshold, in turn, can reduce the service life of the pacemaker. Atrial fibrillation is an indication for a single-chamber pacemaker. Elderly patients are more likely to have atrial fibrillation, which dictates the need to implant a single-chamber pacemaker instead of a dual-chamber pacemaker.
Compliance with the postoperative regimen.
Well, in conclusion, I would like to draw the attention of our elderly patients to the need to carefully monitor compliance with all the doctor’s recommendations in the early postoperative period: do not raise the arm on the implantation side above shoulder level (for at least a month). Do not lie on your right side, sleep on your back or left side (3 months). When talking, place your mobile phone on the ear opposite the side of the implantation. Do not wet the wound for 2 weeks.
If the article was useful to you, rate it and share links on social networks! Leave your comments and questions!
Implantation of pacemaker
Pacemaker implantation is an operation, but it does not require general anesthesia. Local anesthesia of the skin is sufficient. First, one or two or three electrodes are inserted through a vein, depending on how many chambers of the heart need to be stimulated. They are attached to the heart under X-ray control.
Testing is then carried out using the device. Signals are sent to the heart and the reaction is monitored. After the desired effect is achieved, the pacemaker itself is placed under the skin of the chest in the subclavian region. The entire operation takes about 2 hours.
Recovery after installation of the device begins in the hospital - breathing and light therapeutic exercises are prescribed. After discharge, walks are recommended for the first month. Then, based on the results of an examination by a cardiologist, exercises for the arms, running and swimming are added to them. All exercises must be regular, overexertion is unacceptable.
Features of life with ECS
In most cases, the device does not lead to cardiac complications and is not felt by patients. Despite this, after the operation certain restrictions are introduced regarding the patient’s lifestyle.
The patient is not allowed:
- engage in sports in which there is a risk of chest injury (boxing, hockey, football, rugby, etc.),
- perform exercises using weights on the chest muscles,
- located near the transformer booths,
- fly on an airplane,
- drink alcohol in large quantities.
It is not prohibited to use household appliances. The basic rule in this case is to maintain a safe distance between the device and the pacemaker (from 20-61 cm depending on the type of household appliance).
If the pacemaker is installed due to severe heart failure, then the patient is assigned disability group 2 or 3.
Medical procedures for a patient with a pacemaker are prohibited:
- CT and MRI. CT scans are performed only with the consent of the doctor.
- Physiotherapeutic measures using magnetic or electrical radiation.
- Ultrasound with beams directed directly at the device.
Before conducting examinations, the patient warns the doctor about the device he has.
Complications
Naturally, many patients, worried about future intervention in the body, think about how dangerous the operation to install a pacemaker is. Although CS implantation is considered a minimally invasive procedure, there is still a possibility of complications occurring both during and after the operation.
In large clinics with extensive experience in performing implantations, the rate of early complications, as a rule, does not exceed 5%, and late complications - 2.7%. The mortality rate is in the range of 0.08 - 1.1%.
Fistula in the area of pacemaker implantation
Early complications:
- • bleeding (formation of hematomas in the pocket where the CS is installed);
- • thrombophlebitis and phlebitis;
- • displacement of electrodes;
- • infectious inflammation in the implantation area;
- • pneumothorax;
- • hemothorax;
- • infarction of the area of the heart wall where the electrode is fixed;
- • anaphylaxis;
- • air embolism;
- • device malfunction.
Late complications:
- pocket erosions (destructive changes in the tissues around the joint);
- electrode displacement;
- phlebitis or deep vein thrombosis;
- systemic infection;
- atrioventricular fistula;
- device failure;
- endocarditis;
- thrombus formation in the right atrium.
Technological advances and improvements in surgical procedures have led to a significant reduction in the incidence of complications. Recovery after the procedure is usually quick. However, during the first two to four weeks, there is pain and discomfort that limits mobility in the arm. Displacement of the electrodes, their separation from the place of fixation, is the most common problem that can arise after implantation.
Life after installing the device
Only 6% of people with installed pacemakers experience the following complications some time after surgery:
- inflammation of the heart chamber at the site of electrode attachment;
- swelling in the area where the generator is attached;
- instrument offset;
- load intolerance.
Restrictions in everyday life and profession
A person who has a pacemaker installed must always take into account the restrictions that have appeared in his life:
- Falls and blows to the chest area and pressure on it are unacceptable.
You should avoid being near power lines, transformer boxes, electrical panels - a powerful electromagnetic field disrupts the operation of the device.- In everyday life, it is necessary to dose physical activity on the chest area and arms.
- Electrical devices can only be touched with the hand opposite the stimulator.
- It is better to always keep your mobile phone at least 20 cm from the location of the pacemaker.
- All electrical appliances, including those in the office, must be in working order and grounded. In this case, you are allowed to work with them. It is prohibited to work with equipment that can lead to major electrical failures: welding machines, electric motors, steel-smelting furnaces, etc. Based on this, the following professions are prohibited:
- electrician;
- loader;
- electrician
welder;
One of the frequently asked questions before surgery from patients is whether it is possible to fly on an airplane and what to look for at the airport. Often the flight itself is not a contraindication. You should not stand near metal detectors for long periods of time. Be sure to have documents with you confirming the presence of ECS in the body.
Sports and physical education
For the first 1.5-3 months after surgery, you should limit sports activities until the body is completely restored. Then, gradually increasing the load, you can and should begin classes. It is worth giving up those sports that contribute to the breakdown or malfunction of the pacemaker, such as wrestling, football, skydiving, hockey.
It is recommended to avoid extreme sports, activities with a high load on the chest and possible blows to it.
Doctors recommend giving preference to running, race walking, swimming, and yoga. These sports, in addition to being non-traumatic, are great for training the heart.
Medical procedures
Many types of medical tests are contraindicated for a patient with an artificial pacemaker. Prohibited:
- MRI;
- some types of ultrasound;
- electrotherapy;
- lithotripsy;
- magnetotherapy.
Almost every prohibited procedure can be found with a permitted alternative. Some models of stimulants have no contraindications for medical examinations. When visiting any medical institution, you should definitely have with you documents confirming the presence of the device in the body, indicating the model.
Recovery period
Most people feel great, much better than before the procedure.
Usually, on the second day after implantation, they can return to their daily lives in full. How rehabilitation goes after surgery to install a pacemaker is also influenced by the patient’s behavior and compliance with the doctor’s recommendations, which include:
- • During the first 48 hours, it is necessary to avoid getting moisture into the postoperative wound.
- • If swelling, pain, or local warmth appears in the area of the sutures, you should consult a doctor.
- • During the first 4 weeks, you should limit movement in the arm on the side on which the pacemaker is installed.
- • It is recommended to avoid heavy lifting in excess of 20 kg during this period.
Duration of surgery to install a pacemaker
The operation is increasingly moving to the level of a minimally invasive procedure, as a result of which the time it takes is an inconspicuous 40-60 minutes. The fewer complications during implantation, the faster it goes. However, the operation time depends a lot on the type of pacemaker:
- single-chamber installation takes approximately 40-60 minutes;
- two-chamber - approximately 1.5 hours;
- three-chamber - up to 2.5 hours.
The most time from the entire operation is spent on antiseptic treatment and suturing, but in large-scale clinics, even these manipulations take a minimum of time.
After surgery, the patient usually spends several hours in the intensive care unit. If there are no places in it, they can be placed in the ward closest to it. In the absence of any complications, x-rays and electrocardiography are performed. A patient with a normal course of the postoperative period is sent to the general ward after approximately 2-3 hours. In the future, you need to strictly adhere to the doctor’s recommendations and undergo timely examinations, which will extend the life of the device, and therefore significantly improve the patient’s quality of life.
Further observation
People who have a permanent pacemaker should follow their doctor's recommendations and adhere to certain restrictions. The first examination is usually scheduled after 3 months, then after six months. The frequency of follow-up examinations is twice a year, provided there is no concern.
If you experience fainting, dizziness, or your heart rate drops below the programmed level, you should visit a doctor earlier than planned.
Sometimes a problem can occur when the lead loses contact with the heart. This situation requires its replacement. As a rule, it is not removed from the vein, but is disconnected from the pulse generator. A new electrode is attached, which is first moved along the vein along the old one and fixed to the heart.
Battery Replacement
The energy source used in a permanent pacemaker has a limited lifespan (5 to 10 years). The battery is located inside the metal case of the device and is its integral part. Therefore, when its charge is depleted, a procedure is required to replace the pulse generator.
Under local anesthesia, a skin incision is made in the pocket area, the old device is removed (the electrodes are first disconnected), and a new one is implanted in its place. The operation of the new pacemaker is checked, after which stitches are placed. The patient is sent home on the same day.
To see what signal a pacemaker gives when its battery runs out, watch this video:
What is a pacemaker?
A pacemaker is a special device, the main purpose of which is to stimulate the work of the heart muscle , to regulate the correct rhythm of work in people suffering from insufficient heartbeat. It is a small device, the dimensions of which vary from 3 to 5 centimeters , weight from 30 to 45 grams . The service life of a pacemaker depends on the battery and ranges from 5-15 years .
The principle of operation of this device is to apply electrical influences , which cause it to contract in a planned rhythm. Modern devices have additional sensors that measure breathing rate, body temperature and other necessary parameters, transmit the received information for analysis and begin their work only when necessary.
Pacemaker replacement time
The time to replace the pacemaker is determined by how long the battery lasts. On average, it functions normally for about 7 years. When its charge runs out, the device begins to send special signals. There are also reasons for an emergency change - breakdowns, displacements, purulent processes in neighboring tissues. If the implantation took place under a quota (free of charge), then the re-installation will be similar.
We recommend reading the article about complications of pacemaker. From it you will learn about the causes of complications after the installation of a pacemaker, the development of arrhythmia, and problems after implantation in children. And here you can read more about the rules of life after installing a pacemaker.
Cost of the procedure
The cost of installing modern pacemakers, not including their cost, can range from $3,500 to $5,000.
As a rule, the installation of a pacemaker significantly improves the patient’s quality of life if he suffers from arrhythmia, which is accompanied by severe symptoms of heart failure. These electrotherapeutic devices have proven themselves and have been used effectively for the past 60 years. Complications during their installation and further use are very rare.