Cerebral infarction, or ischemic stroke, is a serious disease that manifests itself in acute cerebrovascular accident and is a consequence of other pathologies.
Among all patients who are hospitalized with signs of cerebral blood flow disorders, the vast majority are diagnosed with this particular disease. At the same time, elderly people are at risk.
Considering the tragedy of the possible consequences of delaying seeking medical help at the first signs of the disease (death, severe limitation of physical capabilities), you should not take a wait-and-see attitude and waste precious minutes.
What can trigger
What are the causes of recurrent stroke?
For reference. A second stroke mainly occurs due to people’s negligence towards their health. According to statistics, half of patients after the first episode believe that since recovery occurred quickly, further treatment is not required.
People stop:
- visit a doctor for timely assessment of the condition and correction of medications;
- undergo examinations in order to timely diagnose a potential danger and correctly develop a set of preventive measures to prevent a relapse;
- measure A/D daily, changes in which are one of the main causes of recurrent stroke;
- take medications that prevent high cholesterol and blood clots;
- follow a diet;
- stick to the regime;
- visit a psychologist who will teach you methods of managing stressful situations.
For reference. Having successfully recovered in 2-3 weeks for the first time, people think that everything is behind them and return to the usual rhythm of life, unaware of the consequences. Without thinking that we had walked over the edge.
Risk factors
If the first attack has already been overcome, then you should understand exactly what can provoke a second stroke. You shouldn't rely on chance. By not taking any action, we are only deliberately increasing the risk of recurrence, but with a significantly worse result.
The likelihood of another stroke increases with:
- Over 45 years of age (the likelihood of recurrence increases 15 times).
- Lack of adequate treatment for concomitant diseases - arterial hypertension, atherosclerosis (blockage of the lumen of blood vessels with cholesterol plaques), atrial fibrillation (risk of thromboembolism), aneurysms (risk of hemorrhagic type).
- Endocrine pathologies, especially diabetes.
- Protracted infections that reduce immunity.
- Bad habits - smoking, alcohol, leading to increased blood pressure and blood clotting. The risk of developing hemorrhagic stroke in chronic alcoholics is 30-50%.
- Regular nervous and physical overload.
- Obesity.
- Long exhausting work in summer cottages under the sun, in one position.
- Lack of sleep, indiscriminate eating.
- In women – abuse of hormonal contraceptives.
- Micro-strokes (point hemorrhages), transient ischemic attacks (short-term reversible cerebrovascular accident). Patients do not notice them in time and do not treat them.
Attention. Yes. With some probability, the second attempt can be rescheduled. But after the 3rd stroke it is unlikely that you will be able to get out.
Causes
Not all causes of ischemic stroke can be classified. There are many clinical examples of unclear cardiovascular pathologies, especially in people under fifty years of age. According to various sources, up to 40% of all strokes at a young age do not have an established cause. Nevertheless, several classifications of causes have been proposed, one of which involves a conditional division of causes into two main components. Uncorrectable causes of ischemic stroke:
- age;
- floor;
- hereditary predisposition;
- stress factors;
Uncorrectable causes are given at birth or due to random factors.
Annual risk of developing ischemic stroke at the age of:
- 20 years is 1/3000 people.
- 84 years and above – 1/45 people.
A significant increase in the likelihood of stroke occurs after 45 years of age.
In women under 30 and after 80 years, the risk of developing ischemic stroke is significantly higher than in men of the same age, and from 30 to 80 years, men have more causes of stroke. This statement applies to different age and gender groups that do not have a history of chronic diseases that have been proven to affect cerebral blood flow. A number of researchers have proven a high familial predisposition to cerebral infarctions.
Correctable causes in descending order of importance:
- atherosclerosis;
- arterial hypertension;
- physical inactivity;
- osteochondrosis of the cervical skeleton;
- obesity;
- diabetes;
- alcohol abuse;
- smoking;
- use of oral contraceptives.
Correctable causes are the result of chronic diseases or bad habits.
The leading factors are atherosclerosis and arterial hypertension, caused by impaired lipid carbohydrate metabolism. The risk of developing atherosclerotic plaques begins at age twenty.
Maintaining a normal blood pressure level within the range (120/80), by approximately 40%, reduces the risk of developing ischemic stroke after forty years.
The use of oral contraceptives by young women significantly increases the risk of stroke, namely: the risk of stroke is 13/100,000 in the case of taking contraceptives, versus 3/100,000 in women not taking these drugs. One of the possible reasons for this phenomenon is hypercoagulation of blood cells under the influence of drugs.
Pathogenesis
In the development of secondary ischemic stroke, the main role is played by vascular lesions in the area:
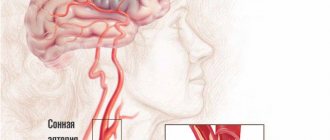
- extracranial – atherosclerosis of the main arteries (usually the carotid) before they enter the cranial cavity (40% of cases);
- brain – intracerebral small arteries (35%);
- cardiac - formation of an air or fat embolus in the left ventricle and subsequent blockage of the middle cerebral artery (15 - 20%).
Vascular lesions leading to cessation of blood flow are represented by:
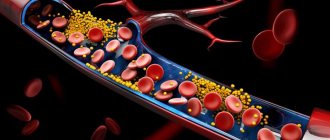
- blockage of the lumen of the vessel with an embolus;
- thickening of the wall due to the deposition of cholesterol plaques on it.
In the first minutes and hours, rapid necrotization of neurons occurs, caused by a pathological chain: -> blockage of the artery -> cessation of blood flow -> hypoxia and oxidation of brain tissue -> disturbance of the metabolism of fats and carbohydrates -> inhibition of the production of neurotransmitters and a decrease in their quantity in the synaptic cleft -> formation of infarction foci.
Foci form within 5-8 minutes. In the first hour and a half, the hypoxia zone covers 50%, in the next 6 hours – 80%. Secondary cerebral edema develops over 3 to 5 days, while the neurons of the affected area become necrotic and the process partially stops. After this period, neurological symptoms come to the fore.
The severity of a recurrent stroke, compared to the primary one, is determined by:
- the area of the previously existing affected area;
- possible transition from ischemic to hemorrhagic;
- late onset or lack of positive dynamics.
What can trigger a recurrent hemorrhagic stroke? Rupture of cerebral arteries and hemorrhage in the brain, leading to compression of the trunk, disruption of the outflow of cerebrospinal fluid and venous blood.
For reference. Ischemic foci are formed, neurons become necrotic. Over time, a cyst forms at the site of the hemorrhage.
What are the risk factors for stroke?
Anyone can suffer from a stroke, regardless of age, gender or race. The likelihood of getting the disease, however, increases when a person has certain risk factors. The good news is that almost 80 percent of strokes are preventable.
There are 2 types of risk factors for cerebral infarction - controlled and uncontrolled. Controllable risk factors generally fall into two categories - risk factors associated with life situations and diseases that can be changed, and situations associated with disease that can be cured.
Controllable risk factors:
- arterial hypertension,
- atrial fibrillation,
- high blood cholesterol levels,
- diabetes,
- atherosclerosis,
- smoking,
- alcohol consumption,
- decreased physical activity,
- obesity.
Uncontrollable risk factors include:
- elderly people (over 55 years old),
- male gender,
- history of stroke or transient ischemic attack in the family and others.
Arterial hypertension
High blood pressure according to WHO (World Health Organization) is defined as a sustained increase in blood pressure of more than 140 mm Hg. for systolic and more than 90 mm Hg. for diastolic.
Increased blood pressure causes the heart to pump blood to different parts of the body with greater effort. This can lead to weakened blood vessels and damage to vital organs such as the brain. If hypertension is not treated promptly, it may be a predisposing factor for stroke. IHD in older people is accompanied by more severe symptoms. It is distinguished by the difficulty of treatment due to concomitant chronic diseases. The same can be said about ischemic colitis in the elderly.
Patients with elevated blood pressure have a 1.5 times higher risk of stroke than patients with optimal blood pressure. Damage to the vascular wall in hypertension is due to unnecessary, excessive stress on the walls of blood vessels, which leads to thickening and damage. Controlling blood pressure and maintaining it within optimal limits is a preventive mechanism for reducing the incidence of cerebral infarction. Arterial hypertension can be treated with:
- diets,
- physical activity,
- medicines,
- combining all three methods.
Types of arterial hypertension:
- secondary hypertension,
- idiopathic (primary) hypertension.
Atrial fibrillation
About 15% of all stroke patients have atrial fibrillation. Patients diagnosed with atrial fibrillation have already taken the first step towards a stroke. Unfortunately, many people have atrial fibrillation without knowing it. Three out of four strokes associated with atrial fibrillation can be prevented if diagnosed.
Atrial fibrillation is a type of arrhythmia. This is reflected in very rapid (350-450 times per minute) cardiac atrial fibrillation. Atrial fibrillation increases the risk of developing a cerebral stroke because it creates conditions for blood to stagnate in the atrium (atrium). This, in turn, is a prerequisite for thrombosis, and the formed thrombus can easily pass through the bloodstream through the blood vessels and cause ischemic stroke in the brain. Treatment of coronary artery disease in the elderly should be gentle and take into account drug tolerability.
High blood cholesterol (dyslipidemia)
Cholesterol is a lipid (fat) that circulates in the bloodstream and is found in all cells of the body. Our body needs cholesterol to create cell membranes, certain hormones and vitamins. Cholesterol is also found in some foods such as eggs, meat and more. Since cholesterol cannot be degraded on its own in the bloodstream, it is carried from cell to cell by special particles called lipoproteins.
Lipoproteins come in several types, both of which have important diagnostic value—low-density lipoproteins (LDL) and high-density lipoproteins (HDL). LDL is also called “bad” cholesterol. This can cause plaque to form in the blood vessels, which can cause them to narrow.
Plaques may also increase the risk of transient ischemic attacks. The second major type of cholesterol, high-density cholesterol (HDL) is often called “good” cholesterol. High HDL levels may reduce the risk of stroke.
Diabetes
Patients with diabetes have a higher risk of developing stroke compared to people without the disease. Diabetes mellitus is a disease characterized by high levels of glucose in the blood due to the inability of the latter to be taken up by cells and used as a source of energy.
There are two main types of diabetes - type 1 (insulin dependent) and type 2 (non-insulin dependent). Type 1 diabetes usually begins in childhood and is characterized by the body's inability to produce enough insulin. Insulin is a hormone that the body uses to convert glucose into an energy source for cells.
Type 2 diabetes is more common. In this type of diabetes, the body can still produce insulin, but tissues develop insulin resistance and blood sugar levels rise above normal. The disease usually appears in adulthood, but diagnosing it can be difficult because the symptoms of the disease (frequent urination, thirst, excessive hunger, weight loss, fatigue, irritability) are harmless and patients do not seek medical help for a long time.
Atherosclerosis
Atherosclerosis puts patients at increased risk of cerebral infarction or transient cerebral blood flow disorders. Atherosclerosis is a disease that usually occurs without obvious symptoms. Conducting preventive examinations and studies can help in early detection of the disease and prevention of cerebral infarction.
Smoking
Smoking doubles the risk of stroke compared to non-smokers. This leads to a decrease in the amount of oxygen in the blood, which requires an increase in cardiac workload to ensure adequate oxygen supply to the tissues. In addition, smoking helps build up deposits on the walls of blood vessels, which reduces cerebral blood flow and can cause coronary artery disease in older citizens.
Alcohol intake
It is not yet clear what the relationship is between alcohol consumption and an increased risk of stroke. In some studies, excessive alcohol consumption showed no association with stroke. For example, drinking more than 2 glasses a day increases the risk of stroke by 50%.
At the same time, other studies have shown that drinking alcohol in small quantities can reduce the risk of stroke. Although moderate drinking is defined as drinking 1-2 glasses of alcoholic beverages per day, many medical experts believe that it increases the risk of stroke and leads to other medical problems such as liver disease, heart disease and possibly brain damage.
Obesity
Obesity leads to congestion of the entire blood flow. It also leads to high cholesterol levels, high blood pressure and diabetes, all of which increase the risk of stroke.
Increased physical activity may help reduce your risk of stroke. Recent research shows that people who exercise five or more times a week have a lower risk of stroke. Eating a low-calorie diet with minimal saturated trans fat and cholesterol helps control obesity and dyslipidemia, which in turn reduces the risk of stroke. A diet rich in salt leads to higher blood pressure values.
A healthy diet should include at least 5 servings of fruits and vegetables per day. Consuming this amount of vegetables and fruits leads to a 30% reduction in the risk of stroke. Citrus fruits and broccoli are especially useful among fruits and vegetables. As we age, the body's ability to absorb vitamin B12 decreases. This can cause a variety of health problems, including an increased risk of heart disease and stroke.
Fibromuscular dysplasia
This dysplasia is a disease characterized by the irregular formation of certain arteries in the body. The fibrous tissue in the wall of the arteries increases, which leads to their narrowing. As a result, blood flow through the arteries is reduced and a stroke may occur. In most cases (75% of patients), dysplasia affects the arteries that are present in the kidneys (renal arteries). In some cases, it may affect the carotid arteries, which supply blood to the brain, or arteries in the limbs, abdomen, and other areas.
Kinds
For reference. Repeated stroke is of two types: ischemic (4/5) and hemorrhagic (1/5), which is much more severe, ending in death in 80% of cases.
Often the primary stroke is ischemic, and the second time is hemorrhagic. Or vice versa. The same affected areas and brain structures are affected, but the pathogenesis is different.
Repeated ischemic stroke is divided into local and extensive.
Local often begins suddenly, the lesion is unilateral. The severity is determined by the location and area of the necrotic area, complications after the first attack. Neurological abnormalities of moderate severity.
With a major stroke, symptoms increase gradually. Consciousness is disabled, deep neurological disorders. Basically, this species ends in death.
Signs of a recurrent hemorrhagic stroke depend on the area of the lesion.
Cortical is the heaviest type. Consciousness is grossly impaired. Severe speech disorders, paralysis, and anesthesia are observed.
Prognosis for life in older people
About 20% of people who have an ischemic stroke die within the first hours or later in the hospital. Another 40-50% remain disabled, more or less capable of caring for themselves. The older the patient, the higher the likelihood of an unfavorable outcome. 10% of people who have a cerebral infarction recover completely. Another 25% have visible signs that they have had a serious illness but can lead normal lives.
The sooner the patient is taken to a medical facility, the more favorable the prognosis for him. Therefore, at the slightest suspicion of a stroke, immediately call an ambulance. Don't waste time! Don’t be afraid to bother doctors in vain or pay for a false emergency call. The risk of severe consequences of ischemic or hemorrhagic stroke is so high that it outweighs all these dangers.
The prognosis after an ischemic stroke depends on the patient’s desire and ability to engage in physical therapy, as well as work on restoring speech. Many people manage to make a full recovery, as if they never had a stroke. To do this, you need to diligently perform rehabilitation exercises. For patients who rely on quack remedies, the prognosis is rather poor.
The above is data from English-language sources. In Russian-speaking countries, the prognosis for patients is less favorable because ambulances are slow, intensive care units are poorly equipped, and their staff rarely receive training in stroke treatment. In Western countries, a lot of money is allocated for long-term rehabilitation of patients. In Russian-speaking countries, the injured person and his family receive little help from the state and surrounding people.
While a patient who has suffered a cerebral vascular accident is in the hospital, doctors are afraid to make prognoses in the first few days. Only later does it become clear how the situation is developing. People who are paralyzed on one side of their body can hope that exercise therapy will help them regain some of their lost function. This goal is achieved by 50% of patients - those who diligently exercise. Restoring the use of a paralyzed arm is usually more difficult than restoring the use of a paralyzed leg. Physical limitations that persist 12 months after the stroke are likely to remain permanent.
Prodromal period
A few weeks before another stroke, the following warning signs arise:
- headaches - occur when overworked, in weather-sensitive people when the weather changes;
- unilateral short-term blindness;
- tinnitus – temporary or continuous;
- dizziness - worsens when moving;
- lack of coordination;
- facial hyperemia;
- convulsions on the side of the stroke;
- fast fatiguability;
- amnesia for recent events;
- decreased concentration;
- short-term speech disorders;
- sleep problems - insomnia, shallow sleep, daytime sleepiness.
People who have experienced a first attack have an easier time recognizing the symptoms of an impending second stroke. If at least two signs are noticed, action must be taken immediately!
How to find out about a stroke?
The consequences of a stroke in women can be the most serious. It is important to correctly identify this condition, since symptoms can manifest themselves partially, in different combinations. You need to ask a person to take a simple test:
- Ask to smile. In a pathological condition, the face will be skewed and the smile will be asymmetrical.
- If the person is sitting or standing, ask him to raise his arms 90 degrees; if he is lying down, ask him to raise his arms 45 degrees. During a stroke, one of his arms will drop.
- Ask them to say a simple phrase. During a stroke, a person's speech is unintelligible.
Stages
The development of a recurrent stroke goes through the following stages, presented in the table:
| Stage name | Term |
| 1. Acute | First 24 hours |
| 2. Spicy | 24 hours – 3 weeks |
| 3. Subacute | 3 weeks – 3 months |
| 4. Early recovery | 3 – 6 months |
| 5. Late recovery | 6 months – year |
| 6. Stage of long-term consequences | One year after relapse |
Clinic by stages
For reference. On the first day of ischemic cerebral infarction, a person suddenly experiences dizziness and nausea, often turning into vomiting. The patient is stunned or, conversely, excited. He is temporarily derealized and does not understand where he is.
One side is partially (hemiparesis) or completely (paralysis) paralyzed. Movement is limited or completely impossible. Your temperature may rise. Facial asymmetry is observed (drooping of the corner of the mouth, inability to close the eye on the side opposite to the lesion). There is numbness in the limbs of the affected side and face. Convulsions are possible.
If the left side is affected, speech is impaired. The patient has poor hearing and vision deteriorates to the point of blindness.
If the stroke is hemorrhagic, the initial symptoms are as follows:
- sharp sudden cephalalgia;
- loss of consciousness, which often ends in coma;
- hyperemia of the skin;
- profuse sweating;
- a sharp increase in A/D to high numbers;
- tachycardia;
- anisocoria (pupils of different sizes), nystagmus (twitching of the eyeballs);
- facial asymmetry;
- lack of coordination;
- muscle hypotonia on one side;
- urinary incontinence;
- seizures of the epileptic type.
In almost all cases, swallowing is difficult. If the breathing and circulatory centers are affected, death occurs.
For reference. In the acute stage, the ischemic focus is localized and neurological symptoms increase. With the hemorrhagic variant, various types of impairment of consciousness are possible (from stunning to coma).
The degrees of post-stroke coma according to Glasgow are presented in the table:
| Severity | Symptoms | Forecast |
| First | The patient is drowsy, his reactions are inhibited, and he does not react acutely to pain. Contact is difficult to reach. The swallowing reflex is preserved. The patient can independently roll over in a lying position and perform simple movements. The pupils react to light. | Favorable, minimal complications. |
| Second | Does not make contact, state of stupor. Rare chaotic muscle contractions are observed. Involuntary physiological effects. Swallowing reflexes are preserved. The pupils are strongly constricted and almost do not react to light. Breathing is pathological, noisy, characteristic of cerebral hypoxia. | Survival is unlikely. |
| Third (atonic) | The patient is unconscious. There is no reaction to light or pain at all. Pharyngeal reflexes are very weak. Hypotension. Hyperthermia. The breathing rhythm is disturbed. | The probability of survival is close to zero. |
| Fourth | The patient shows no signs of life, breathing may stop every second. | No chance. |
| Fifth | Agony and death |
Mortality occurs on days 2–4 or on days 10–12 (if complications develop).
In the subacute stage, the process does not worsen. It is either stable, without changes, or is slowly improving. Then, with proper treatment and compliance with rehabilitation measures, an early and late rehabilitation period begins. After a year, long-term consequences are recorded.
First aid
Attention. The effectiveness of treatment primarily depends on the time of first aid and the professionalism of the team. The sooner others call an ambulance, the greater the chance of promptly localizing the lesion and stopping the rapidly developing hypoxia and neuronal necrosis.
When the first signs of secondary cerebral infarction occur, you must:
- Call an ambulance.
- Lay the patient down with the head elevated.
- Measure A/D and give an antihypertensive drug, if available.
- Carefully remove dentures, contact lenses, unfasten the collar, loosen the belt, remove watches and glasses.
- If a patient loses consciousness, you should not try to revive him. You need to turn your head to the side, open your mouth slightly so that the tongue does not fall in to avoid asphyxia.
- Place a cold compress or ice on your forehead.
Poor prognostic symptoms for stroke
There are symptoms that worsen the overall life prognosis of ischemic stroke:
- depression of consciousness;
- inability to move independently (the patient can only open and close his eyelids), lack of speech, although the patient’s understanding of what is happening may remain;
- pronounced cognitive and emotional-volitional disorders;
- dysphagia (difficulty swallowing);
- persistent hyperthermia - indicates damage to the thermoregulation center and aggravates ischemic damage to brain tissue. A decrease in body temperature by 1°C doubles the chances of a favorable outcome;
- muscle hypertonicity, throwing the head to one side, convulsive twitching or prolonged epileptic seizures, lack of coordination of movements, loss of control over the body;
- urinary incontinence;
- persistent gaze paralysis, eye movement disorder (pendulum-like oscillations or slow movements of the eyeballs, lack of synchrony of eye movements);
- violation of hemodynamic parameters (severe heart rhythm disturbances, high blood pressure);
- severe hemiparesis (weakening of the muscles on one side of the body);
- somatic diseases in the stage of decompensation, severe infectious and inflammatory diseases;
- pathological types of breathing: Kussmaul breathing (deep noisy inhalation and forced exhalation), Cheyne-Stokes breathing (alternating deep breaths and shallow respiratory movements, Biot breathing (long pauses between breaths);
- comatose state - the chances of recovery after four months of cerebral coma caused by ischemic brain damage remain only in 10% of patients.
Factors that aggravate the prognosis in acute cerebrovascular accidents include diseases of the cardiovascular system, the presence of concomitant diseases in the stage of decompensation, endocrine disorders, and a history of stroke.
Resuscitation measures
A specialized ambulance team carries out all necessary measures at home and on the way to the clinic. Transportation should be as gentle as possible. The patient is placed in the intensive care unit or intensive care unit.
Diagnostics are carried out to determine the area and level of the lesion, possible consequences and choice of treatment tactics. They do a blood test for cholesterol, sugar, prothrombin, and a general urine test. Neurological status is assessed using the US and Scandinavian stroke scales. Instrumental types of research are carried out - CT, MRI, EEG, EchoEG, ECG, EchoCG.
In the first hours of repeated ischemic stroke, try:
- restore the hemodynamics of damaged arteries - antispasmodics, nicotinic acid, saline solutions;
- reduce thrombosis by administering thrombolytics;
- protect neurons - neuroprotectors;
- prevent cerebral edema - dehydration.
Resuscitation measures for secondary hemorrhagic type include:
- stopping bleeding - hemostatic agents;
- prevention of compression of the brain stem by hematoma - removal of the tumor. Conservative treatment is indicated only for minor hemorrhages.
How to treat
A person is treated for a stroke in a hospital, where constant monitoring is provided. During therapy, the following activities are carried out:
- The cause that caused the stroke is eliminated. This could be a sharp increase in blood pressure due to hypertension, vascular atherosclerosis, ischemia, or kidney problems. The patient's condition is stabilized with the help of medications.
- Blood flow is restored. For this purpose, agents are used that thin the blood and eliminate vascular spasms. But if a hemorrhagic stroke occurs, in which there is severe bleeding and the walls of the vessels rupture, then it is necessary to reduce the blood pressure on the vessels.
- Medications are prescribed to improve the tone of the vascular walls.
- Blood pressure is normalized with the help of drugs injected into the blood.
- Diuretics are taken to lower blood pressure and prevent brain swelling.
Important information: What exercises can you use to restore speech impairment after a stroke (aphasia) and teach you to speak at home?
For stroke in older people, medications are prescribed to maintain heart function and reduce cholesterol in the blood. The treatment also includes a diet that must be strictly followed. The person’s lifestyle is also adjusted.
Further treatment
After successful resuscitation measures, the patient is transferred to the neurological department, where treatment is continued with the aim of:
- improve microcirculation of brain vessels;
- prevent neuronal hypoxia;
- reduce A/D;
- reduce cholesterol levels;
- reduce thrombosis;
- stabilize the nervous and mental state;
- prevent constipation.
For hemorrhagic stroke, medications are prescribed to stop bleeding. Vasodilators and anticoagulants (thrombolytics) are prohibited.
When the patient’s condition stabilizes, he is transferred to home treatment, where he continues to take medications and undergoes a course of long-term rehabilitation.
Two different forms of stroke
An ischemic stroke occurs when a blood clot in an artery in the brain becomes stenotic and deprives the area of oxygen and nutrients. This stroke accounts for 80% of stroke cases.
Hemorrhagic stroke is mentioned in more rare cases when an artery in the brain is damaged. This stroke accounts for 20% of cases. Blood passes through the brain and creates a hematoma. The part of the brain around the hematoma becomes compressed or even damaged. However, cerebral bleeding should not be confused with meningeal hemorrhage.
Rehabilitation
For reference. Rehabilitation measures begin from the second to third week from the onset of the secondary attack.
They include a set of special exercises to restore paralyzed limbs, physiotherapy, massage, and diet. They are carried out by a specialist in a hospital in the presence of relatives, who subsequently, after completing physiotherapeutic procedures, do the same at home.
If the patient is alone, or his relatives are unable to provide him with proper care, he undergoes a course in specialized centers.
For reference. 50% of self-care skills, motor and cognitive functions are restored during the first 2-3 months, the remaining half by the end of the year.
Physiotherapy helps improve metabolism, nutrition of cerebral vessels, reduce ischemia, and increase motor activity. The procedures reduce A/D, thrombus formation, and normalize blood composition. Physiotherapy is prescribed already in the acute period with the goal of reducing muscle hypertonicity; in hemorrhagic cases, 2 months after the onset of relapse.
Exercise therapy begins after the patient’s condition has stabilized. The limbs are fixed in a physiological position - the hand is opened, the fingers and foot are extended, the leg is bent at the knee. The patient is given special exercises to strengthen muscles and improve microcirculation in paralyzed limbs. Repeat them several times a day. Massages are provided daily.
Diet. The result of rehabilitation measures will be reduced if you do not adhere to a special diet aimed at reducing cholesterol, high-density lipids, and eliminating fatty, salty, fried, smoked, and baked goods. Food should be taken in small portions, 5-6 times a day.
Attention. Rehabilitation after a second stroke is long. Full recovery is unlikely. The result depends on the qualifications of the medical staff, the patient’s faith in improving his condition, and the enormous efforts of those around him.
What should people at risk do?
First of all, it is necessary to focus on the fact that the risk group includes not only individuals who have suffered a stroke, but also those who experience short-term transient attacks. To prevent the formation of a recurrent stroke, you must contact a neurologist, follow all his recommendations and undergo periodic preventive examinations.
Diagnostics
To prescribe adequate therapy and its correction, it is necessary to carry out diagnostics, namely:
- Ultrasound of the carotid arteries and large vessels of the brain;
- echocardiograms;
- electrocardiograms;
- determination of blood lipid profile;
- coagulograms.
Consequences
The prognosis of a recurrent stroke depends on the extent of the lesion, residual effects after the first event, timely medical intervention, competent support during the rehabilitation period, and the patient’s mood.
The consequences of a second stroke are much more significant than after the first attack:
- persistent hemiparesis or paralysis that confines the patient to bed;
- severe speech disorders;
- significant visual and hearing defects;
- violation of mnestic functions;
- emotional-volitional disorder;
- loss of self-care skills;
- inability to lead a normal lifestyle.
For reference. All this leads to disability, dependence on others, which causes depressive moods, often with suicidal thoughts.
What is dangerous for women?
A stroke occurs due to a sudden disruption of the blood supply to the brain . Depending on the type of disease, either blockage of the vessel by a detached blood clot (ischemic stroke) or hemorrhage due to rupture of the artery (hemorrhagic stroke) is noted.
In both cases, brain cells located in the affected area die. This threatens the patient with complete or partial loss of functions that a specific part of the brain provided:
- speech;
- hearing;
- vision;
- memory;
- coordination of movements;
- Often the disease leads to a loss of general clarity of consciousness.
The danger of a stroke lies in the fact that impaired functions sometimes cannot be restored even after a well-designed course of rehabilitation. The patient may permanently lose the ability to work, the ability to do favorite activities, become bedridden and need round-the-clock care. As for stroke mortality, about half of patients die within the first year after the illness.
An additional challenge is the prompt diagnosis of stroke. If the disease develops in men with classic symptoms, then in women atypical symptoms are often observed, which confuse the picture and complicate the diagnosis of the pathology.
Forecast
Life expectancy after a recurrent stroke does not exceed 5 years. How many strokes can a person have? According to statistics, 50% of patients who have had two strokes are at risk of having a third.
The risk of a third recurrent stroke increases in people who have suffered micro-strokes , which no one paid attention to in a timely manner.
Assessment of the condition for a third cerebral infarction includes:
- clinical outcome;
- duration of recovery;
- the likelihood of complications.
For reference. Prognosis of a third stroke is divided into early and late. Early shows whether the patient has a chance of surviving the first month after the 3rd stroke. Late - assessment of the level of dysfunction, loss of self-care skills, degree of disability.
Silent stroke
A silent stroke is a cerebral infarction common among older and middle-aged people in which no symptoms develop. Patients usually do not even realize that they have had a stroke.
Likewise, patients with severe stroke are also at risk for silent strokes. Silent variants of the disease usually cause damage that can be detected by magnetic resonance imaging. They are thought to occur approximately 5 times more often than symptomatic ones. The risk increases with age, but it may also affect younger people, especially those with severe anemia.
Prevention
How to avoid another stroke? Only with the help of prevention, which includes a review of lifestyle. It is worth considering your age and health status.
Prevention includes:
- Regular observation of a doctor after the first attack, taking the necessary medications.
- Regular examination in order to timely identify the risk of relapse.
- Compliance with a regimen that includes adequate sleep, feasible physical activity, and diet.
- Performing physical therapy exercises.
- Treatment of chronic diseases.
- Rejection of bad habits.
- Avoiding stressful situations.
Features of a stroke in an old person
Stroke is a disease that requires emergency medical intervention. At different ages, the consequences of pathology will differ markedly. Patients over 70–80 years of age have a very severe clinical picture of the disease and minimal chances of survival, especially if a major stroke occurs.
It is in old age that 45% of patients who have had an attack are susceptible to subsequent coma in the first few days. After a stroke, an old person's prognosis for restoring the body's functional capabilities will be much worse than that of people under 50 years of age. Even if the patient manages to survive, there is a high chance of remaining disabled, most often bedridden.
Elderly people, fearing to upset their loved ones, often ignore the symptoms of the disease themselves, thereby aggravating their situation during a stroke. When working with such patients, some characteristic features of the course of the disease should be taken into account:
- Stroke increases rapidly and is more severe, since the body of an old person is subject to age-related changes and is burdened by other chronic diseases.
- Elderly people put off visiting a medical facility, citing the fact that this is a common ailment at their age. Unfortunately, age plays a negative role, since at the time of a stroke, brain tissue is affected much faster in an older person.
- In older patients, major ischemic stroke is diagnosed more often than in 30–40 year olds.
- The most common cause of attacks after 60 years is the presence of atherosclerotic plaques.
We recommend
“High blood pressure in older people: treatment, prevention and traditional methods of combating the disease” Read more