Kaposi's sarcoma, what is it? First symptoms and methods of treatment Kaposi's sarcoma in HIV-infected patients is one of the “AIDS-indicating” diseases. The detection of a tumor of this type in young people without obvious disturbances in the functioning of the immune system provides grounds for diagnosing HIV infection in the AIDS stage, even without the use of laboratory research methods.
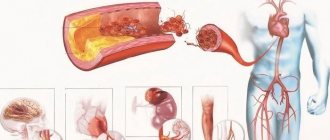
Kaposi's sarcoma accounts for 85% of all tumors developing in AIDS patients. This is a malignant multifocal tumor of vascular origin that affects the skin, mucous membranes and internal organs. It has several varieties, one of which is epidemic sarcoma associated with AIDS.
The tumor affects people under the age of 35 - 40 years, most often occurs in passive homosexuals, manifests itself as spots, nodules or plaques of a bright red or red-brown color, quickly spreads throughout all the skin, mucous membranes and internal organs. Elements of the tumor merge over time to form tumor-like formations, which eventually ulcerate. Kaposi's sarcoma is difficult to treat and quickly leads to death in patients. The correct diagnosis is easily established and confirmed by examining a piece of tissue under a microscope.
Causes
The reasons that cause the appearance of such neoplasms are not known for certain. But scientists with a high degree of probability suggest that the disease can develop against the background of human herpes virus type 8, which itself has not yet been sufficiently studied.
Kaposi's sarcoma also often accompanies other malignant processes, including:
- lymphosarcoma;
- multiple myeloma;
- mycosis fungoides;
- Hodgkin's lymphoma (lymphogranulomatosis);
- leukemia.
For pathology to occur, a significant decrease in human immunity due to various reasons is necessary. In addition, some groups of people have a much higher risk of developing Kaposi's sarcoma than others. For example, the disease is more often observed in men than in women.
At risk are:
- HIV-infected persons;
- persons with organ transplants from donors (especially kidneys);
- elderly men belonging to the Mediterranean race;
- persons whose homeland is equatorial Africa.
Medical scientists are unanimous on one thing: most often, especially in the initial stages of development, this disease is more likely to be a reactive process (that is, occurring in response to an infectious lesion) than a true sarcoma.
Preventive measures
The first preventive measures for Kaposi's sarcoma involve identifying people at risk.
Patients using immunosuppressive therapy should be among the first to be tested for the presence of patients with herpes virus type 8.
Further prevention involves monitoring patients in order to prevent premature relapse of the disease.
Preventive measures include:
- preventing sexual contact without condoms;
- annual medical examinations by a dentist, surgeon, examination of mucous membranes;
- eliminating tobacco products from everyday life;
- ban on the use of corticosteroids;
- strengthening the immune system;
- limiting sun exposure in the summer;
- prevention of HIV, AIDS.
The presence of angiosarcoma in a relative is a reason to think about it and undergo examination for the presence of pathology, since there is a high probability of transmitting the disease by inheritance.
Pathological anatomy
Usually the tumor is purple in color, but the color can have various shades: red, purple or brown. The tumor may be flat or slightly raised above the skin and appear as painless spots or nodules. Almost always located on the skin, less often on internal organs. Kaposi's sarcoma is often combined with damage to the mucous membrane of the palate and lymph nodes. The course of the disease is slow. The discovery of Kaposi's sarcoma in HIV infection provides grounds for the diagnosis of AIDS.
The histological structure of the tumor is characterized by many chaotically located thin-walled newly formed vessels and bundles of spindle cells. Tumor infiltration by lymphocytes and macrophages is characteristic. The vascular nature of the tumor sharply increases the risk of bleeding. However, a biopsy is not necessary if Kaposi's sarcoma is suspected. Kaposi's sarcoma is a special type of tumor that often does not require not only verification of the diagnosis, but also its treatment. This may seem strange at first glance. This situation is due to the fact that an accurate diagnosis can be made without a biopsy, and isolated treatment of Kaposi's sarcoma extremely rarely gives complete healing.
Moreover, treatment of Kaposi's sarcoma (due to its connection with the causative factors of the underlying disease) is usually palliative, that is, aimed only at reducing the symptoms of the disease.
Types of rashes
The disease in oncology is also divided into four types depending on the type of rash:
- Nodular sarcomatosis, in which purple nodules and plaques form on the lower extremities, which over time spread throughout the entire skin.
- Disseminated sarcomatosis is characterized by damage to internal organs and systems.
- Red sarcomatosis, in which formations appear that in appearance resemble polyps with legs, red in color.
- Infiltrative sarcomatosis is caused by the appearance of rashes on the skin with damage to bones and muscles.
Symptoms
The clinical picture of Kaposi's sarcoma is quite varied and depends on the duration of the disease.
In the initial stages, the symptoms of sarcoma appear as reddish-bluish spots of varying shapes and sizes, as well as pink nodule-like elements, which then acquire a bluish color. As Kaposi's sarcoma progresses, the rash takes on the appearance of nodular infiltrated elements of a reddish-bluish color of various sizes. These nodules tend to merge, which leads to the formation of large lumpy foci with sharply painful ulcers. In the area of the outbreak, the skin is thickened, swollen, and purple-bluish in color. The lesions are mainly localized on the skin of the distal extremities (in 94% on the lower extremities - the anterolateral surfaces of the legs and feet) and tend to be located near the superficial veins. Often there is symmetry of the damage to the extremities.
According to its course, the tumor can be subacute, acute and chronic. The acute course of Kaposi's sarcoma is characterized by rapidly progressive symptoms and is manifested by generalized skin lesions in the form of many nodular formations on the trunk, face and limbs, as well as fever. These symptoms are accompanied by damage to internal organs and/or lymph nodes. The duration of the acute form is from two months to two years.
In the subacute course of sarcoma, generalization of skin rashes is observed much less frequently. The chronic course is characterized by gradual progression of skin rashes in the form of plaques and macular-nodular elements. The duration of the chronic form is eight years or more. [adsen]
Forecast
The prognosis of Kaposi's sarcoma is determined by the form of the disease, the individual characteristics of the patient, and the state of the immune system, in particular. If the body’s defenses have potential, then with quality treatment a favorable outcome can be achieved.
Otherwise, even at the first stage, the prognosis is not in favor of the patient - about 40% of patients die in just a few months . In this case, therapeutic measures can only delay death. It is worth remembering that everything is determined by immunity status. Therefore, for people with AIDS, the occurrence of sarcoma is considered extremely dangerous.
We recommend watching a video in which a specialist talks about the course of Kaposi's sarcoma in people not infected with HIV:
If you find an error, please select a piece of text and press Ctrl+Enter.
Epidemic type
The appearance of this neoplasm is one of the main symptoms of HIV infection. This type of Kaposi's sarcoma is characterized by:
- onset at a young age (before 40 years);
- brightly colored neoplasms;
- characterized by the obligatory involvement of mucous membranes in the process;
- unusual location of sarcoma elements: on the tip of the nose, in the oral cavity on the hard palate, upper extremities.
This type of disease is characterized by a rapid and malignant course involving lymph nodes and internal organs.
Kinds
In the practice of studying Kaposi's sarcomotosis, four types of the disease are distinguished. The location, degree of damage, treatment and diagnostic features depend on the specific type. It becomes obvious that to fully understand this oncology, it is necessary to analyze each option separately.
Look at the photo to see how different types of skin cancer manifest themselves. In this article, symptoms of spleen lymphoma.
Follow the link https://stoprak.info/vidy/golovy-i-shei/mozg/na-kakie-simptomy-obratit-vnimanie.html symptoms and signs of head cancer.
So, Kaposi's sarcoma can manifest itself in the following types:
- Classic. Tumors form on the feet, hands and legs. In rare cases, tumors may appear in the ear, on the scalp, or on the mucous membrane and eyelids. The manifestations of the disease are symmetrical, usually do not cause any symptoms, but may be accompanied by sensations of itching and heat.
The variety under consideration involves the division into three more forms: spotted, papular and tumor. The first is characterized by spots up to 5 millimeters of bluish or brownish tints. They have an irregular border and a smooth surface.
The second form is distinguished by spots in the form of spheres up to 1 centimeter, which have a dense consistency. The surface can be smooth or rough. As for the tumor type, it appears in the form of nodes up to 5 centimeters in diameter with a reddish-brown color and soft consistency.
During the course of the disease, the nodes unite and ulcerate. In most cases, the classic type of sarcoma is benign and can be asymptomatic for more than 10 years.
- Endemic. First of all, oncology affects internal structures. In particular, damage to the lymph nodes occurs without any manifestations on the surface of the skin.
The rashes themselves take on an asymmetrical shape with a reddish tint. Patients are susceptible to pain, heat, and increased sweating. Endemic sarcoma develops very aggressively.
- Epidemic. This species is often associated with the human immunodeficiency virus, since the epidemic form is one of its symptoms. The rash is localized on the tip of the nose, oropharynx and head.
It appears in the form of small asymmetrical and reddish spots. As the disease progresses, the rash becomes ulcerated and the lymph nodes become enlarged. The disease is quite aggressive, which causes high mortality - about 80% of the total number of cases.
- Immunosuppressive. It is characterized by malignancy, develops and spreads in a short time. The main reason for the occurrence is a malfunction of the immune system, which is caused by the use of cytostatics and immunosuppressants.
This type manifests itself in a nodular form, subsequently rapid transformation into a tumor occurs. This sarcoma may regress if immunosuppressive therapy is stopped. This consequence is explained by the fact that the functionality of the immune system is restored and gradually returns to normal.
Photo: initial stage
Diagnostics
Diagnosis of Kaposi's sarcomatosis is carried out by an infectious disease specialist, dermatologist and oncologist. First, doctors listen to the patient and collect anamnesis, and then:
- Check for signs of disease.
- They do a biopsy.
- A histological examination is carried out to detect the proliferation of fibroblasts.
- Conduct immunological studies.
- Blood is taken for HIV testing.
The patient is also prescribed additional tests, for example, ultrasound, radiography, gastroscopy, CT scan of the kidneys, MRI of the adrenal glands and others to identify internal lesions.
The first symptoms are in the mouth, on the leg
Most often, a spotted rash or nodules appear on the skin, which have the following characteristic features:
- color – bluish, brown, violet, purple;
- shape – flat, papules in the form of a sphere or hemisphere;
- there is no pain at first, then large nodes are sensitive to palpation, ulcerations are accompanied by severe pain;
- after resorption, a stain with deep indentation remains.
Patients are concerned about burning and pain in the area of large nodes, which becomes stronger at night; most often the rash is localized on the legs.
When the mucous membranes of the mouth are affected, tumor elements may bleed, making eating and speaking difficult.
Complications
The occurrence of complications of Kaposi's sarcoma depends on the stage of development of the disease and the location of the tumors. The following complications may occur:
- lymphatic edema, elephantiasis due to compression of the lymph nodes;
- bacterial infection of damaged tumors;
- limitation of motor activity of the limbs and their deformation;
- bleeding from disintegrating tumors;
- intoxication of the body caused by the breakdown of tumors;
- disruption of the functioning of internal organs when tumors are localized on them.
Some complications lead to life-threatening conditions. [adsen2]
Alternative home treatments
Alternative treatments for Kaposi's angiosarcoma include:
- Nutrition and food additives.
- Herbal tinctures and balms.
The diet should be rich in vitamins to increase the stability of the immune system, and easily digestible proteins should be consumed to create antibodies.
Fiber in foods will help promote bowel movements and eliminate toxins.
To combat the disease, you can add lingonberries and apricots with pits to your daily menu.
Treatment of Kaposi's sarcoma
Treatment of single lesions is carried out surgically (excision of the lesion) followed by radiation therapy. Such treatment for classical Kaposi's sarcoma leads to a successful result (long-term remission) in 30-40% of patients.
If the patient has generalized Kaposi's sarcoma, and in particular, an HIV-infected person, then a complex of antiretroviral therapy, chemotherapy, interferon therapy, and radiation therapy is indicated (however, in the AIDS stage this often does not lead to the desired result).
1) Highly active antiretroviral therapy (HAART)
- the duration of such therapy should be at least a year;
- helps suppress the viral load and increase the immune status during HIV infection;
- Antiretroviral drugs can completely suppress the vital activity of one of the herpes viruses, which causes cancer - Kaposi's sarcoma.
2) Chemotherapy, for which prospidine (domestic drug), vincristine and vinblastine (rosevin), etoposide, taxol, doxirubicin, bleomycin and others are used. The drugs have pronounced side effects on the hematopoietic organs and others, which often requires the prescription of hormonal therapy (prednisolone, dexamethasone).
3) Interferon therapy.
- Purpose: interferon preparations are prescribed as an immunomodulatory effect, namely: recombinant alpha interferon 2a and 2b (intron, roferon, reaferon) or native (wellferon) in doses of 5-10 million IU/day intramuscularly, subcutaneously in long courses .
4) Local therapy includes: radiation therapy, cryotherapy, application of special gels (panretin), local chemotherapy.
Drugs that would be sufficiently effective in treating infection caused by HHV-8 have not yet been found.
How to treat
Kaposi's sarcoma requires adequate treatment. Therapy is based on increasing the performance of the body's autoimmune system. The isolated course of the disease rarely provides the opportunity for complete healing.
The attending physician prescribes a palliative course aimed at suppressing the main clinical signs of the disease.
Local treatment
Treatment of Kaposi's sarcoma includes a number of auxiliary techniques:
- cryotherapy;
- injection administration of chemotherapeutic drugs;
- introduction of interferon into the tumor;
- applying applications and ointments to problem areas of the dermis.
Indications for local irradiation are existing large lesions of damaged skin, the need to achieve a cosmetic effect.
Systemic therapy
Systemic treatment of Kaposi's sarcoma is carried out using surgical intervention - excision of problematic lesions, followed by the use of radiation therapy. The classic form of the pathology is cured in 40% of cases.
Generalized forms, especially in those affected by HIV infection, require the use of:
Highly active antiretroviral therapy:
- total duration is more than one year;
- suppression of the negative effects of viruses;
- increasing the performance of the autoimmune system.
Certain types of these medications can suppress the vital activity of herpes infection, which provokes the formation of Kaposi's sarcoma.
Chemotherapy is carried out with Prospidin, Vincristine, Rosevin, Taxol, Bleomycin, etc. In parallel with this treatment, patients are recommended to undergo hormonal therapy - against the background of pronounced side effects in the area of the hematopoietic organs.
Treatment with interferons - medications are used as immunomodulators. Therapy is carried out in long courses, with periodic replacement of medications.
Prognosis of Kaposi's sarcoma
The prognosis of the disease with Kaposi's sarcoma depends on the nature of its course and is closely related to the state of the patient's immune system.
With higher levels of immunity, the manifestations of the disease can be reversible; systemic treatment gives a good effect and allows one to achieve remission in 50-70% of patients. Thus, in patients with Kaposi's sarcoma with a CD4 lymphocyte count of more than 400 μl-1, the frequency of remissions against the background of immune therapy exceeds 45%, and with a CD4 count of less than 200 μl-1, only 7% of patients can achieve remission.
Pathomorphology and histology
The pathomorphological picture of Kaposi's sarcoma foci is as follows:
- chaotic and incomplete angiogenesis, that is, the formation of new blood vessels;
- proliferation of spindle-shaped cells characteristic of this tumor, having the nature and characteristics of endothelial cells;
- immunocellular accumulation (infiltration) in the blood and lymphatic vessels of mononuclear cells (blood cells with one nucleus).
The origin of tumor cells—from cells of lymphatic or blood vessels—remains not entirely clear. The results of histological examination are varied. Apparently, this depends on the type of elements and the stage of their development. In the early stages of development of rash elements in Kaposi's sarcoma, their cells look like endothelial cells of lymphatic vessels, and at later stages - both lymphatic vessels and blood vessels.
Prevention
The main measure to prevent the disease is timely and correct treatment of immunodeficiency conditions. Thus, the use of antiretroviral drugs in HIV-infected patients allows for a long time to maintain the normal function of the immune system, thereby preventing the appearance of Kaposi's sarcoma.
After treatment of Kaposi's sarcoma, a thorough examination of the skin and mucous membranes is necessary at least once every 3 months, assessment of the condition of the lungs and gastrointestinal tract - at least once every six months or a year. These measures will help to detect relapse of the disease in time.
Mechanism of origin and development
a herpes virus enters the body . It penetrates sexually, hematogenously or through saliva. The main factor in the development of the oncology in question is a violation of the optimal functioning of the immune system.
Often the process of spread of sarcoma is caused by the occurrence of other oncological lesions: mycosis, lymphosarcoma, Hodgkin's disease.
Atlas of skin diseases
SARCOMA MULTIPLE IDIOPATHIC HEMORRHAGIC KAPOSH (sarcoma idiopathicum haemorrhagicum multiplex Kaposi).Synonyms: Kaposi's angioreticulosis, Kaloshi's angiosarcoma, Kaloshi's sarcoma, skin angioendothelioma, etc. The disease was first described by Kaposi in 1872.
Etiology and pathogenesis
Most modern authors consider it as a disease of unknown etiology, having features of tumor diseases of perivascular reticulohistiocytic tissue.
Clinic
The disease occurs in representatives of all continents, but is unevenly distributed. In Asia it is a casuistic rarity.
The incidence is high in Africa, where it ranges from 0.04% in Tunisia to 9.1% in the Congo, in relation to all malignant tumors.
Quite often, Kaposi's sarcoma is observed in Europe - in Russia, Italy, Hungary, France, etc.
Based on duration and especially severity, three forms of the disease are distinguished.
- In the chronic form, progression is slow and patients live on average 6-8 years, sometimes longer (up to 15-20 years).
- In the subacute form, the disease progresses rapidly and leads to death within 2-3 years.
- The acute form is characterized by early generalization of the process, steady progression and death several months after the onset of the disease.
Men get sick more often than women, the ratio between them ranges from 3:1 to 32:1, averaging 8:1. In Europe, angioreticulosis most often affects people aged 40 to 70 years, in Africa - from 20 to 40 years.
Kaposi's sarcoma often begins with the appearance of reddish-bluish spots the size of a lentil to a 10-kopeck coin. Gradually increasing in size, they reach a diameter of 2-5 cm. The spots are well delimited, their surface is smooth. Another common early manifestation of angioreticulosis is a spherical, less often flat, nodule the size of a millet grain to a small pea, pinkish-bluish in color, and soft consistency. The nodules are located isolated, often grouped.
Subsequently, tumors and hemispherical nodes are formed, ranging in size from a large pea to a hazelnut, clearly rising above normal skin. The consistency of the tumors is densely elastic; their surface is shiny, uneven, with small depressions, like an orange peel, and less often smooth. They are located either isolated or merge into large lumpy formations. The color of the lesions at the beginning of the disease is reddish-bluish, later the color intensity intensifies to a bluish-brownish color. As a result of the disintegration of tumors and nodes, which is observed in approximately 15-20% of patients, deep, sharply painful (“shooting” pains) ulcers of irregular shape are formed, with slightly everted edges, painted in a rich bluish-purple color. The bottom of the ulcers is lumpy, covered with bloody-gangrenous discharge. Many patients experience vegetation of granulation tissue and verrucous growths.
Rarely, multiple bullous and vesicular rashes are observed, located on edematous legs and feet and clinically resembling lymphangioma. Multifocality, prevalence and symmetry of rashes are an important feature of Kaposi's angioreticulosis. Most often (in almost 80-90% of patients), the process is widespread with a predominant localization on the feet, legs and back of the hands. Among the rarer localizations of primary rashes, mention should be made of the ears, cheeks, nose, back, abdomen, and penis.
Damage to the oral mucosa occurs in 2-12% of patients with angioreticulosis. Most often, the rashes are located on the soft, hard palate, then on the cheeks, pharynx, larynx, tongue and arches. In patients with a significant spread of lesions, they are almost always accompanied by intense, excruciating pain. Approximately 25-40% of patients experience swelling of the affected areas, mainly the feet, legs and hands, and severe elephantiasis often develops with multiple papillomatous and hyperkeratotic growths.
Enlargement of peripheral lymph nodes is not the leading symptom of Kaposi's angioreticulosis; it occurs in approximately 20-25% of patients, more often in the subacute form of the disease.
The hemogram remains normal in most cases. Lymphocytosis and monocytosis are detected in 2/3 of patients.
Bone damage, characterized by osteoporosis (usually the feet) and periostosis, atrophy of the articular ends of the phalanges, is detected radiographically in approximately 1/3 of patients with Kaposi's angioreticulosis, mainly with widespread tumor-nodular rashes.
Histopathology
The dermis contains numerous vascular lumens surrounded by endothelial and perithelial cells; pronounced proliferation of spindle-shaped cells - young fibroblasts; some of them are atypical. There are areas of hemorrhage and hemosiderin deposits. Cell mitoses are detected.
Differential diagnosis
It should be carried out with malignant melanoma, fibromatosis, dermatofibrosarcoma, lichen planus, angioma, lymphangioma, Raynaud's disease, thrombophlebitis, cutaneous reticulosis, skin lymphomas, Kaposi's pseudosarcoma, etc.
Treatment
Penicillin in the initial stages of the disease up to 20-30 million per course; cytostatics (prospidin, phosphazine, methotrexate, 6-mercaptopurine) are recommended for patients with widespread nodular and tumor-nodular formations. X-ray therapy is indicated for limited tumor-like lesions. It is advisable to combine surgical removal of large tumors with pre- or postoperative chemotherapy.
KAPOSH SARCOMA as a manifestation of AIDS
At the end of the twentieth century, a connection between Kaposi's sarcoma and a disorder of the immune status was established. This was first noted in patients undergoing kidney transplantation and receiving immunosuppressive therapy.
The first report of such a combination comes from Siegel et al. (1969). It was followed by a large number of similar publications.
It is known that Kaposi's sarcoma can be combined with other diseases that require long courses of treatment with corticosteroids or cytostatics - with lupus erythematosus, pemphigus, dermatomyositis, bronchial asthma, chronic myeloid leukemia, etc. An important proof of the immunodependence of Kaposi's sarcoma in these patients is the fact of tumor remission with complete withdrawal or reduction of doses of immunosuppressants.
Thus, clinical observations make it possible to identify an independent immune-dependent form of Kaposi's sarcoma, which is characterized by an extremely malignant course, occurring against the background of massive therapy with immunosuppressants of pre-existing diseases.
Since 1981, the connection between a number of diseases, including Kaposi's sarcoma, in individuals with acquired immune deficiency syndrome (AIDS - Acquired Immune Deficiency Syndrome) has been widely discussed.
In addition to Kaposi's sarcoma, this syndrome includes various infectious diseases, such as Pneumocystis pneumonia, infectious mononucleosis, generalized herpes simplex, meningitis and encephalitis caused by aspergillus, systemic candidiasis, B-cell lymphomas and others.
The most common type of AIDS is Pneumocystis pneumonia - in 52%, less commonly Kaposi's sarcoma - in 28%, and their combination is observed in 9% (Gottlieb, Sonnichsen and Dorte Ruff, etc.).
Summarizing numerous studies available in the literature, it can be assumed that the decisive criterion for AIDS for changes in the immune system is the insufficiency of cellular immunity, with the following coming to the fore: clear lymphopenia in the peripheral blood, absence of skin reactions to tests with various antigens, a decrease in the ratio of T-helper cells to T-suppressograms (less than 1).
The main link in the pathogenesis of Kaposi's sarcoma in homosexuals is considered to be a disorder of immunity caused by various factors, including viruses.
Clinic
The immunosuppressive form is distinguished from ordinary Kaposi's sarcoma by:
- young age,
- sudden appearance of generalized forms of nodular and tumor-like formations,
- rare or absent patchy rashes,
- atypical arrangement of skin elements - head, neck, oral cavity, torso,
- rapid progression of the process,
- more frequent damage to visceral organs and lymph nodes,
- resistance to therapy,
- poor prognosis - 50%-60% of patients die within 3 months to 2 years.
Treatment
There are no effective treatments yet.