| Polycythemia | ||
| ICD-10 | 45. (ICD-O 9950/3), 75.1, 61.1 | |
| ICD-9 | 238.4, 289.0, 776.4 | |
Polycythemia vera
(Greek poly many + histological cytus cell + haima blood) (synonyms: primary polycythemia, polycythemia vera, erythremia, erythremia, Vaquez disease) is a benign disease of the hematopoietic system associated with myeloproliferation and hyperplasia of cellular elements of the bone marrow. This process affects the erythroblastic germ to a greater extent. An excess number of red blood cells appears in the blood, but the number of platelets and neutrophilic leukocytes also increases, but to a lesser extent. The cells have a normal morphological appearance. By increasing the number of red blood cells, blood viscosity increases and the mass of circulating blood increases. This leads to a slowdown in blood flow in the vessels and the formation of blood clots, which leads to impaired blood supply and organ hypoxia.
The disease was first described by Vaquez [1] in 1892. In 1903, Osler[2] suggested that the disease was caused by increased activity of the bone marrow. He also identified erythremia as a separate nosological form.
Polycythemia vera is a disease of adults, more often of older people, but also occurs in young people and children. [3] For many years the disease does not make itself felt and proceeds without symptoms. According to various studies, the average age of those affected ranges from 60 years to 70-79 years. [4][5] Young people get sick less often, but their illness is more severe. Men get sick somewhat more often than women, the ratio is approximately 1.5:1.0; women predominate among young and middle-aged patients. A family predisposition to this disease has been established, which indicates a genetic predisposition to it. Among chronic myeloproliferative diseases, erythremia is the most common. The prevalence is 29:100,000.
Content
- 1 Cause of polycythemia
- 2 Clinical picture
- 3 Laboratory indicators for polycythemia vera
- 4 Complications of polycythemia
- 5 Diagnostics
- 6 Diagnosis algorithm
- 7 Differential diagnosis
- 8 Treatment 8.1 Bleeding
- 8.2 Erythrocytopheresis
- 8.3 Cytoreductive therapy
Clinical picture[edit]
The clinical manifestations of the disease are dominated by manifestations of plethora and complications associated with vascular thrombosis. The main manifestations of the disease are as follows:
- Dilation of cutaneous veins and changes in skin color
On the skin of patients, especially in the neck area, protruding, dilated, swollen veins are clearly visible. With polycythemia, the skin has a red-cherry color, especially pronounced on exposed parts of the body—the face, neck, and hands. The tongue and lips are bluish-red, the eyes seem to be bloodshot (the conjunctiva of the eyes is hyperemic), the color of the soft palate is changed while the normal color of the hard palate is preserved (Cooperman's symptom). The peculiar shade of the skin and mucous membranes occurs due to the overflow of the superficial vessels with blood and the slowdown of its movement. As a result, most of the hemoglobin has time to transform into a reduced form.
- Itchy skin
Patients experience skin itching. Itchy skin is observed in 40% of patients. This is a specific diagnostic feature for Vaquez disease. This itching intensifies after swimming in warm water, which is associated with the release of histamine, serotonin and prostaglandin.
- Presence of erythromelalgia
These are short-term unbearable burning pains in the tips of the fingers and toes, accompanied by redness of the skin and the appearance of purple cyanotic spots. The appearance of pain is explained by an increased number of platelets and the appearance of microthrombi in the capillaries. A good effect for erythromelalgia is observed from taking aspirin
- Enlarged spleen (splenomegaly)
A common symptom of erythremia is an enlarged spleen of varying degrees, but the liver can also be enlarged. This is due to excessive blood supply and the participation of the hepato-lienal system in the myeloproliferative process.
- Development of ulcers in the duodenum and stomach
In 10-15% of cases, an ulcer of the duodenum develops, less often of the stomach; this is associated with thrombosis of small vessels and trophic disorders in the mucous membrane and a decrease in its resistance to Compylobacter [9].
- The occurrence of blood clots in blood vessels
Previously, vascular thrombosis and embolism were the main causes of death in polycythemia. Patients with polycythemia have a tendency to form blood clots. This leads to impaired blood circulation in the veins of the lower extremities, cerebral, coronary, and splenic vessels. The tendency to thrombosis is explained by increased blood viscosity, thrombocytosis and changes in the vascular wall.
- Presence of bleeding
Along with increased blood clotting and thrombus formation, bleeding from the gums and from dilated veins of the esophagus is observed in polycythemia
- Persistent joint pain and increased uric acid levels
Many patients (20%) complain of persistent pain in the joints of a gouty nature, as there is an increase in the level of uric acid
- Leg pain
Many patients complain of persistent pain in the legs, the cause of which is obliterating endarteritis, accompanying erythremia, and erythromelalgia.
- Flat bone pain
When flat bones are beaten and pressure is applied to them, they are painful, which is often observed with bone marrow hyperplasia.
- General complaints
Deterioration of blood circulation in the organs leads to patient complaints of fatigue, headache, dizziness, tinnitus, rush of blood to the head, fatigue, shortness of breath, flickering spots in the eyes, blurred vision. Blood pressure is increased, which is a compensatory reaction of the vascular bed to an increase in blood viscosity. Heart failure and myocardiosclerosis often develop.
Polycythemia treatment with folk remedies. Diet for polycythemia vera. Erythrocytosis - treatment
More about carbohydrates for erythremia All carbohydrates are a good source of energy for humans, and some of them also contain fiber, which is beneficial for digestion. Read more about water for erythremia Water is one of the important aspects of dietary nutrition when there is an increased content of red blood cells in blood tests.
The article was prepared by nutritionist Azarova Marina Andreevna Most often, blood viscosity is increased in residents of high mountains, where the oxygen content in the air is reduced, accordingly, more red blood cells are produced, and pathology develops. Reduced blood viscosity during erythrocytosis The danger of erythrocytosis is that the blood becomes much more viscous.
Nutrition for erythrocytosis: foods that reduce blood viscosity Compliance with a diet for erythrocytosis is one of the prerequisites for a speedy recovery. Try to limit your intake of foods rich in vitamin K, as they help blood clot and make it thicker. Chokeberries, spinach, lettuce and other leafy vegetables are especially rich in this vitamin.
Make sure your body regularly receives iodine: it reduces blood viscosity and increases vascular tone. Grind dry seaweed in a coffee grinder and season your dishes with it instead of salt at the rate of 1 tsp. Eat foods that reduce blood viscosity and contain taurine, which normalizes blood pressure: poultry, white fish, shellfish, walnuts and almonds, it is advisable to eat 1 tbsp daily.
Eat fish at least once a week, giving preference to fatty sea and ocean varieties: fish oil contains substances that help not only thin the blood, but also dissolve existing blood clots and sclerotic plaques. Remember that blood viscosity is reduced by garlic, tomatoes, sweet bell peppers, especially red ones, cherries, sweet cherries, melon, grapefruit, sweet clover herb, and gingko biloba.
Include chili peppers in your diet: they contain vitamins A and E, as well as potassium and folic acid, which are excellent blood thinners and prevent cardiovascular diseases. Drink 1 ml of freshly squeezed orange juice daily. Among other things, it is a rich source of vitamin C. However, it should be remembered that orange juice is contraindicated for stomach ulcers and gastritis with high acidity. An excellent blood thinner is 1 glass of dry red wine with lunch or dinner.
Physical education for erythrocytosis and treatment with folk remedies For erythrocytosis, not only the diet, but also the motor mode should be changed. Polycythemia erythremia, Vaquez's disease: causes, signs, course, therapy, prognosis Polycythemia is a disease that can be assumed just by looking at the patient's face. What kind of disease is polycythemia? Cancer or not cancer? Why do sprouts grow incorrectly? Complaints and clinical picture If there is nothing to say about the causes of polycythemia, then a lot can be said about the clinical manifestations.
The patient’s subjective sensations are of a general nature: Weakness and constant feeling of fatigue; Significant decrease in performance; Increased sweating; Headaches and dizziness; Noticeable memory loss; Visual and auditory disorders decreased.
Complaints characteristic of this disease and characterized by it: Acute burning pain in the fingers and toes; the vessels become clogged with platelets and red blood cells, which form small aggregates there; The pain, however, is not so burning, in the upper and lower extremities; Body itching is a consequence of thrombosis, the intensity of which noticeably increases after a shower and hot bath; Periodic appearance of a rash such as urticaria. Obviously, the cause of all these complaints is a violation of microcirculation.
In this case, red blood cells begin to behave like suppressors and suppress the immunological response to viruses and tumors. In addition, they are found in abnormally high quantities in the blood, which further aggravates the condition of the immune system; The kidneys and urinary tract suffer, so patients have a tendency to pyelonephritis and urolithiasis; The central nervous system does not remain aloof from the events occurring in the body; when it is involved in the pathological process, symptoms of cerebrovascular accidents, ischemic stroke due to thrombosis, hemorrhages, less often, insomnia, memory impairment, and mnestic disorders appear.
From the asymptomatic period to the terminal stage Due to the fact that polycythemia in the first stages is characterized by an asymptomatic course, the above manifestations do not occur in one day, but accumulate gradually and over a long period of time, it is customary to distinguish 3 stages in the development of the disease. Stage of advanced clinical manifestations.
It occurs in two stages: II A - occurs without myeloid metaplasia of the spleen, subjective and objective symptoms of erythremia are present, the duration of the period is years; II B - myeloid metaplasia of the spleen appears. ESR in polycythemia vera is always reduced and can reach zero. The degree of severity and prognosis of the disease with polycythemia in a general blood test is indicated by platelets; the more there are, the more severe the course of the disease; BAC biochemical blood test to determine the level of alkaline phosphatase and uric acid.
Erythremia is characterized by the accumulation of the latter, which indicates the development of gout as a consequence of Vaquez's disease; Radiological testing using radioactive chromium helps determine the increase in circulating red blood cells; Sternal puncture - collection of bone marrow from the sternum, followed by cytological diagnosis. The specimen shows hyperplasia of all three germs with a significant predominance of red and megakaryocytic; Trephine biopsy, a histological examination of material taken from the ilium, is the most informative method that allows one to most reliably identify the main symptom of the disease - trilinear hyperplasia.
So, the diagnosis has been made... What next? To do this, ml of blood is taken at intervals of a day until the number of red blood cells and Hb drops. Hematologists sometimes replace the bloodletting procedure with erythrocytopheresis, when, after collection by centrifugation or separation, red blood is separated and the plasma is returned to the patient; Cytostatic therapy myelosan, imifos, hydroxyurea, hydroxyurea; Antiplatelet agents aspirin, dipyridamole, which, however, require caution in use.
Nutrition, diet and folk remedies A significant role in the treatment of polycythemia is given to the work regime, reduction of physical activity, rest and nutrition. Prognosis for polycythemia vera Among blood diseases, there are many that cause a decrease in various elements - red blood cells, leukocytes, platelets. Features of the disease Primary polycythemia vera is a blood disease from the leukemia group that occurs idiopathically for no apparent reason, has a long-term chronic course and is characterized by an increase in the number of red blood cells, an increase in hematocrit and blood viscosity.
Causes of the pathology The primary form of the disease is considered hereditary and is transmitted in an autosomal recessive manner. Classification of polycythemia vera The disease is classified into the following stages: First, or initial stage.
It can last more than 5 years and represents the development of plethoric syndrome, that is, increased blood supply to organs. At this stage, symptoms may be moderate, and no complications arise. A general blood test reflects a slight increase in the number of red blood cells, a bone marrow puncture shows an increase in erythropoiesis or the production of all the main elements of blood, with the exception of lymphocytes.
Laboratory indicators for polycythemia vera[edit]
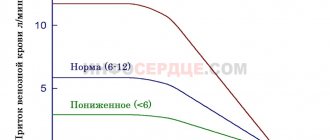
The number of red blood cells is increased and is usually 6×10¹²—8×10¹² per 1 liter or more. Hemoglobin increases to 180-220 g/l, the color index is less than one (0.7-0.6). The total volume of circulating blood is significantly increased - 1.5 -2.5 times, mainly due to an increase in the number of red blood cells. Hematocrit indicators (the ratio of red blood cells and plasma) change sharply due to an increase in red blood cells and reaches a value of 65% or more.
The number of reticulocytes in the blood is increased to 15-20 ppm, which indicates enhanced regeneration of red blood cells.
Polychromasia of erythrocytes is noted; individual erythroblasts can be detected in the smear.
The number of leukocytes increased 1.5–2 times to 10.0 × 10 9–12.0 × 10 9 per liter of blood. In some patients, leukocytosis reaches higher numbers. The increase occurs due to neutrophils, the content of which reaches 70-85%. A band or, less commonly, myelocytic shift is observed. The number of eosinophils increases, and less often basophils.
The number of platelets is increased to 400.0×109-600.0×109 per liter of blood, and sometimes more. Blood viscosity is significantly increased, ESR is slow (1-2 mm per hour).
Uric acid levels increase
What is erythremia
With erythremia, proliferation (growth) of red blood cells occurs and the number of other cells greatly increases (pancytosis).
There is also an increase in hemoglobin. Is erythremia an oncology, is it cancer or not? Most often, erythremia is benign in nature, with a long course, but degeneration of the benign form of the disease into a malignant one can occur, followed by death.
Erythremia is a fairly rare disease. It is diagnosed in approximately 4 out of 100 million people per year. The disease does not depend on the gender of the person, but usually develops in patients after 50. At a young age, cases of the disease are more often diagnosed in women. Erythremia (ICD 10 code - C 94.1) is characterized by a chronic form of the course.
For your information! Erythremia is considered one of the most benign blood diseases. Death often occurs due to the progression of various complications.
The disease is asymptomatic for a long time. Patients with this diagnosis tend to bleed heavily (although the level of platelets, which are responsible for stopping bleeding, is elevated).
There are two types of erythremia: acute form (erythroleukemia, erythromyelosis, erythroleukemia) and chronic. Depending on the progression, they are divided into true and false. The first form is characterized by a persistent increase in the number of blood cells and is extremely rare in children. The peculiarity of the second type is that the level of red blood cells is normal, but the plasma volume is slowly decreasing. Depending on the pathogenesis, the true form is divided into primary and secondary (erythrocytosis).
Complications of polycythemia[edit]
Complications of the disease arise due to thrombosis and embolism of arterial and venous vessels of the brain, spleen, liver, lower extremities, and, less commonly, other areas of the body. Splenic infarction, ischemic stroke, cardiac infarction, liver cirrhosis, and deep vein thrombosis of the thigh develop. Along with thrombosis, bleeding, erosion and ulcers of the stomach and duodenum, and anemia are noted. Very often, cholelithiasis and urolithiasis develop due to an increase in the concentration of uric acid. nephrosclerosis
Polycythemia symptoms
The classification of polycythemia is quite detailed. It is customary to distinguish not only the forms, but also the stages of the disease. This allows you to more accurately prescribe a course of therapy and rehabilitation. There are several forms of the disease:
- true polycythemia (primary, Vaquez disease). The erythroblastic germ in the bone marrow undergoes hyperplastic changes.
- relative polycythemia (secondary, Gaisbeck syndrome).
Additionally, polycythemia vera is divided into 3 stages:
- primary. Develops at the onset of the disease, the duration of the course can exceed a five-year period. The manifestation of symptoms is mild or there is no symptomatic picture at all;
- expanded. It can last about 20 years. It occurs with or without damage to the spleen.
- heavy. It is characterized by the formation of oncological tumors of any location, but more often not only the spleen, blood, but also the liver are affected.
Secondary polycythemia (Gaisbeck syndrome) can develop as a reaction to prolonged stress, poor working conditions and lack of proper rest. This course can go away with a minimal therapeutic course, but subject to the eradication of the root cause of the disease. Polycythemia vera may be false. It does not lead to a shift in the erythrocyte, leukocyte, or platelet balance.
The first signs (syndrome) of the disease usually do not cause suspicion. In the early stages, paroxysmal headaches, blurred vision, a person loses sleep, and complains of dizziness and nausea. The fingertips on both the upper and lower limbs are cold. Their temperature is practically independent of the ambient temperature.
Diagnostics[edit]
When diagnosing polycythemia vera, the assessment of clinical, hematological and biochemical parameters of the disease is of great importance. The characteristic appearance of the patient (specific coloring of the skin and mucous membranes). Enlarged spleen, liver, tendency to thrombosis. Changes in blood parameters: hematocrit, number of erythrocytes, leukocytes, platelets. An increase in the mass of circulating blood, an increase in its viscosity, a low ESR, an increase in the content of alkaline phosphatase, leukocytes, and serum vitamin B12. It is necessary to exclude diseases where there is hypoxia and inadequate treatment with vitamin B12. To clarify the diagnosis, a trephine biopsy and histological examination of the bone marrow are necessary.
The most commonly used indicators to confirm polycythemia vera are:
- Increase in the mass of circulating red blood cells:
- for men - 36 ml/kg,
- for women - more than 32 ml/kg
- Increase in hematocrit >52% in men and >47% in women, increase in hemoglobin > 185 g/l in men and > 165 g/l in women
- Arterial blood oxygen saturation (more than 92%)
- Enlarged spleen - splenomegaly.
- Weight loss
- Weakness
- Sweating
- Absence of secondary erythrocytosis
- The presence of genetic abnormalities in bone marrow cells, other than the presence of a chromosomal translocation of the Philadelphia chromosome or with a rearranged BCR ABL gene
- Colony formation by erythroid cells in vivo
- Leukocytosis more than 12.0×109 l (in the absence of temperature reaction, infections and intoxications).
- Thrombocytosis more than 400.0×109 per liter.
- An increase in the level of alkaline phosphatase in neutrophil granulocytes by more than 100 units. (in the absence of infections).
- Serum vitamin B12 level is more than 2200 ng
- Low erythropoietin levels
- Bone marrow puncture and histological examination of the punctate obtained by trepanobiopsy show an increase in megakaryocytes.
Diagnosis of the disease
As mentioned above, most often polycythemia vera is detected during a preventive blood test. Experts diagnose erythrocytosis if blood tests show levels above normal:
- hemoglobin level increased to 240 g/l;
- the level of red blood cells is increased to 7.5x10 12 /l;
- leukocyte level increased to 12x10 9 /l;
- platelet level increased to 400x10 9 /l.
To study the function of red bone marrow, a trephine biopsy procedure is used, because it is the disruption of the production of stem cells that provokes the development of polycythemia. To exclude other diseases, specialists can use studies such as ultrasound, urinalysis, FGDS, ultrasound, etc. The patient is also prescribed consultations with specialized specialists: neurologist, cardiologist, urologist, etc. If a patient is diagnosed with polycythemia, what is the treatment for this disease, consider the main methods.
Diagnosis algorithm[edit]
The diagnosis algorithm[10] is as follows:
- Determine whether the patient has:
- A. increase in hemoglobin or B. increase in hematocrit
- B. splenomegaly with or without increase in platelets or leukocytes
- G. portal vein thrombosis
- If so, secondary polycythemia should be excluded.
- If secondary polycythemia is excluded, continue the algorithm:
If the patient has three major criteria or the first two major ones in combination with two minor ones: then a consultation with a hematologist is necessary, since there is all the evidence for a diagnosis of polycythemia vera.
Large criteria
:
- increase in the mass of circulating red blood cells: for men - 36 ml/kg,
- for women - more than 32 ml/kg
Minor (additional) criteria
- increase in platelet count
- increase in white blood cell count
- increase in alkaline phosphatase
- increase in vitamin B12
then there is true polycythemia and observation by a hematologist is necessary.
Additionally, you can determine the presence of growth of erythroid colonies in a medium without erythropoietin, the level of erythropoietin (analysis sensitivity 70%, specificity 90%), conduct histology of bone marrow puncture,
Diagnosis of the disease
As mentioned above, most often polycythemia vera is detected during a preventive blood test. Experts diagnose erythrocytosis if blood tests show levels above normal:
- hemoglobin level increased to 240 g/l;
- the level of red blood cells is increased to 7.5x10 12 /l;
- leukocyte level increased to 12x10 9 /l;
- platelet level increased to 400x10 9 /l.
To study the function of red bone marrow, a trephine biopsy procedure is used, because it is the disruption of the production of stem cells that provokes the development of polycythemia. To exclude other diseases, specialists can use studies such as ultrasound, urinalysis, FGDS, ultrasound, etc. The patient is also prescribed consultations with specialized specialists: neurologist, cardiologist, urologist, etc. If a patient is diagnosed with polycythemia, what is the treatment for this disease, consider the main methods.
Treatment[edit]
The treatment is based on reducing blood viscosity and combating complications - blood clots and bleeding. Blood viscosity is directly related to the number of red blood cells, so phlebotomy and chemotherapy (cytoreductive therapy), which reduce the mass of red blood cells, have found use in the treatment of polycythemia vera. Phlebotomy remains the leading treatment for erythremia. Additionally, symptomatic agents are used. Treatment of the patient and his observation should be carried out by a hematologist.
Bleeding[edit]
Bloodletting (phlebotomy) is the leading method of treatment. Bloodletting reduces blood volume and normalizes hematocrit. Bloodletting is performed when plethora and hematocrit are above 55%. It is necessary to maintain the hematocrit level below 45%. 300–500 ml of blood are removed at intervals of 2–4 days until plethoric syndrome is eliminated. The hemoglobin level is adjusted to 140–150 g/l. Before bloodletting, in order to improve the rheological properties of blood and microcirculation, intravenous administration of 400 ml of rheopolyglucin a and 5000 units of heparin a is indicated. Bloodletting reduces skin itching. A contraindication to phlebotomy is an increase in platelets above 800,000. Phlebotomy is often combined with other treatment methods.
Erythrocytopheresis[edit]
Bloodletting can be successfully replaced with erythrocytopheresis.
Cytoreductive therapy[edit]
In persons with a high risk of thrombosis, cytoreductive therapy is carried out together with bloodletting or in case of ineffectiveness of maintaining hematocrit only with bloodletting.
To suppress the proliferation of platelets and erythrocytes, drugs from different pharmacological groups are used: antimetabolites, alkylating and biological substances [11]. Each drug has its own characteristics of use and contraindications.
Imiphos, myelosan (busulfan, mileran), myelobromol, chlorambucil (leukeran) are prescribed. In recent years, hydroxyurea (Hydrea, Litalir, Sirea), pipobroman (Verzite, Amedel) have been used. The use of hydroxyurea is indicated for people in older age groups. Among biological substances, recombinant interferon α-2b (intron) is used, which suppresses myeloproliferation. When using interferon, platelet levels decrease to a greater extent. Interferon prevents the development of thrombohemorrhagic complications and reduces skin itching.
In recent years, the use of radioactive phosphorus has been reduced. The treatment for erythremia is radioactive phosphorus (P32), first used by Lawrence in 1936. It inhibits myelopoiesis, including erythropoiesis. The use of radioactive phosphorus is associated with a high risk of developing leukemia.
To reduce the number of platelets, anagrelide is used at a dose of 0.5-3 mg per day.
The use of Imatinib in true police settings has not yet reached the research stage.
Useful foods for erythremia
To combat polycythemia, the patient should adhere to a plant-based and fermented milk diet. Recommended for use:
- raw, boiled, stewed vegetables (especially beans);
- kefir, yogurt, cottage cheese, milk, yogurt, sourdough, fermented baked milk, sour cream (necessarily without fillers, better homemade);
- eggs;
- greens (spinach, sorrel, dill, parsley);
- dried apricots and grapes;
- dishes made from whole grains (tofu, brown rice, whole grain bread);
- nuts (almonds and Brazil nuts);
- tea (especially green).
Traditional medicine for erythremia
For treatment, the use of leeches and bloodletting (phlebotomy) is indicated. These treatments help lower iron levels in the body, which helps normalize the number of red blood cells in the blood. The frequency and duration of such procedures depends on the stage of erythremia. These methods can only be used when prescribed by medical professionals and in their immediate presence.
To prevent blood clots from forming, you need to move more and spend time in the fresh air. Also, juice made from chestnut (horse) flowers will help get rid of thrombosis.
To normalize blood pressure, sleep, and for migraines, you should drink an infusion of medicinal clover. It should be noted that the course of treatment should not exceed 10-14 days.
To dilate blood vessels, improve blood flow, and increase the resistance of capillaries and blood vessels, you need to drink decoctions of periwinkle, nettle, hornbeam and burial ground.
In simple terms, erythremia is a thickening of the blood when free erythrocytes (red blood cells) increase, and with them hemoglobin. This condition threatens the development of thrombosis, and therefore requires an integrated approach to treatment, including dietary nutrition.
The main principle and goal of therapeutic nutrition for this disease is to thin the blood by drinking large amounts of purified water and reducing certain protein foods that enhance the production of red blood cells.
Treatment of complications of polycythemia[edit]
To prevent thrombosis and embolism, disaggregation therapy is used: acetylsalicylic acid in a dose (from 50 to 100 mg per day), dipyridamole, ticlopedine hydrochloride, trental. At the same time, heparin or fraxiparin is prescribed. The use of leeches is ineffective. To reduce skin itching, antihistamines have been used - blockers of antihistamine H1 systems - (Zyrtec) and paraxetine (Paxil).
For iron deficiency use:
- androgenic drugs: Winobanin (Danazol®)
- erythropoietin
- Thalidomide (alone or together with corticosteroid hormones)
- lenalidamide (Revlemid) in combination with corticosteroid hormones
With the development of autoimmune hemolytic anemia, the use of corticosteroid hormones is indicated.
To reduce uric acid levels - allopurinol, interferon α.
Bone marrow transplantation for polycythemia is rarely used because bone marrow transplantation itself can lead to poor outcomes.
For cytopenia, anemic and hemolytic crises, corticosteroid hormones (prednisolone), anabolic hormones, and B vitamins are indicated.
Splenectomy is possible only in cases of severe hypersplenism. If acute leukemia is suspected, surgery is contraindicated.
How does erythremia develop?
Erythremia develops as follows. Red blood cells (their function is to deliver oxygen to all cells of the human body) begin to be intensively produced so that they cannot fit into the bloodstream. When these red blood cells overwhelm the bloodstream, blood viscosity and blood clot formation increase. Hypoxia increases, cells do not receive enough nutrition, and the entire functioning of the body begins to malfunction.
Where are red blood cells formed in the human body? Red blood cells are formed in the red bone marrow, liver, and spleen. The distinctive ability of red blood cells is the ability to divide, transforming into another cell.
The normal level of hemoglobin in the blood is different and depends on age and gender (in children and older people its amount is lower). The normal content of red blood cells (normocytosis) in 1 liter of blood is:
- for men – 4.0 – 5.0 x 1012;
- for women – 3.5 – 4.7 x 1012.
The cytoplasm of an erythrocyte is almost 100% occupied by hemoglobin, which contains an iron atom. Hemoglobin gives the red color to red blood cells and is responsible for the delivery of oxygen to all organs and the removal of carbon dioxide.
The formation of red blood cells is constant and continuous, starting from intrauterine development (in the third week of embryo formation) and until the end of life.
As a result of mutations, a pathological clone of a cell is formed, which has similar capabilities for modification (can become an erythrocyte, platelet or leukocyte), but is not under the control of the body’s regulatory systems that maintain the cellular composition of the blood. The mutant cell begins to multiply, and the result of this is the appearance of absolutely normal red blood cells in the blood.
This is how 2 different types of cells arise - normal and mutant. As a result, the number of mutated cells in the blood increases, exceeding the body's needs. This inhibits the release of erythropoietin by the kidneys and leads to a decrease in its effect on the normal process of erythropoiesis, but does not affect the tumor cell. As the disease progresses, the number of mutant cells increases and they displace normal cells. There comes a moment when all the red blood cells in the body arise from the tumor cell.
With erythremia, a maximum of mutant cells turn into nuclear charged erythrocytes (erythrokaryocytes), but a certain part of them develops with the formation of platelets or leukocytes. This explains the increase in the number of not only red blood cells, but also other cells. Over time, the level of platelets and white blood cells obtained from the cancer cell increases. The process of sludge occurs—the blurring of the boundaries between red blood cells. But the erythrocyte membrane is preserved, and sludge is a pronounced aggregation - crowding of erythrocytes. Aggregation leads to a sharp increase in blood viscosity and a decrease in its fluidity.