Indications for surgery
Stenting of the coronary arteries can be carried out only after a complete diagnosis, including angiography - an X-ray and contrast examination of the cardiovascular system. This helps to determine the presence of narrowings in the vessels, their location, extent, and other nuances. Based on the data, the doctor decides whether it is permissible to perform a stent on the patient and selects the appropriate type of tube.
Surgery also takes place under X-ray control. Sometimes coronary angiography of the heart and stenting are performed on the same day. However, the second operation is not suitable for everyone, but only:
- patients with ischemia who are not helped by medications;
- those patients who, based on the test results, were allowed to install a stent in the heart (if atherosclerosis did not affect the main trunk of the artery);
- patients with angina pectoris whose professional activities are closely related to serious physical activity;
- having unstable angina or having recently experienced a myocardial infarction:
- if the institution where they were taken can perform such an operation;
- and if the patient’s condition allows it.
The essence
All surgery is performed through a puncture in the skin. A special catheter with a balloon is placed at the location of the problem, which expands there and pushes the vascular walls to normal sizes, restoring blood circulation.
X-rays constantly monitor the process, and the latest medical technology allows for the finest manipulations. A radiopaque solution helps determine the degree of dilation of the vessel.
Finally, a stent is installed. It is a metal mesh that does not allow the vessels to shrink.
How is stenting performed?
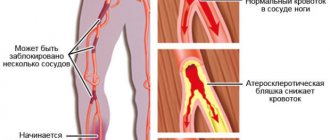
Vasoconstriction due to the development of atherosclerosis is very dangerous for humans. Depending on the location of the damage to the arteries, the disease can lead to a disruption of the blood supply to the brain - the carotid arteries supply it with blood, and with stenosis this function worsens. There are other equally serious pathologies. Frequent problems:
- cardiac ischemia;
- atherosclerosis of the lower extremities.
Modern medicine (the branch of endovascular surgery) has several common methods for restoring arterial patency:
- conservative drug therapy;
- stenosis of heart vessels;
- coronary artery bypass grafting;
- angioplasty (opening the affected artery using a catheter).
The stenting procedure can be performed in an emergency situation (in the presence of unstable angina or myocardial infarction). In other cases, the operation is performed as planned. Based on the results of laboratory tests, during which the condition of the patient’s blood vessels and heart is determined, the doctor approves or prohibits stenting of blood vessels. Before placing a stent:
- A general blood and urine test is taken from the patient;
- do an ECG, coagulogram;
- perform ultrasonic scanning.
Stenting takes place under sterile conditions in the operating room using local anesthetic. Stent placement is done under fluoroscopic control. To gain access to damaged vessels, the doctor punctures a large artery. A small tube (introducer) is inserted through the hole. It is needed to insert other instruments into the artery. A flexible catheter is placed through the introducer to the mouth of the affected artery. Through it, a stent is delivered directly to the site of narrowing of the vessel.
The specialist places the tube so that after deployment it is positioned as successfully as possible. Next, the stent balloon is filled with contrast, which causes it to inflate. Under the influence of pressure, the tube expands. If the stent is positioned correctly, the doctor takes out the instruments and applies a bandage to the puncture site. Stenting takes on average 30 to 60 minutes, but can be extended if multiple tubes need to be installed at once.
How they do it
Stenting of the iliac vein or artery is divided into stages:
- Anesthesia. Usually local to the intervention site.
- Puncture (or puncture) of a large vessel, usually the femoral artery.
- Inserting a catheter with a special balloon.
- Inserting a balloon into the site of narrowing of the vessel and inflating it to normal size.
- Using another catheter, a stent is installed into the resulting lumen for stabilization.
- Removal of both catheters.
- Press the puncture site for 15 minutes until the blood clots completely.
A special feature of stenting is that the catheter does not need to be placed far from the femoral artery. The operation lasts no more than 1.5 hours.
Life expectancy after stenting
A cardiologist is a doctor who often sees and observes his patients for years. Coronary heart disease is a chronic phenomenon, so this is not surprising. Sometimes you come across such stories: a person develops hypertension, angina, then suffers a heart attack and undergoes stenting.
Repeated heart attacks and heart failure are not rare phenomena even after repeated operations. As a result, a person feels much worse than he could, and his life expectancy is reduced.
Why does this happen? The reason is not only the insidiousness and danger of the disease, although, undoubtedly, both are fully inherent in coronary heart disease. Most often, an unfavorable outcome of the disease is determined by the fact that a person makes insufficient efforts to improve his condition and prolong his life.
If you have had stent surgery and you are not following all the lifestyle recommendations, it is time to consider changing your attitude towards treatment. All the tips listed above are clear, simple and doable; you just need to follow them, constantly and conscientiously.
To ensure that the results of stenting are the best and last as long as possible, it is also recommended to undergo a course of cardiac rehabilitation in a sanatorium. After stenting, hemodynamics change in the heart and throughout the body, so the body needs time to adapt to this.
The period of hospital treatment is not enough for the body to fully recover, so cardiac rehabilitation is recommended for patients after stenting. A set of health procedures will consolidate the results of therapy and improve a person’s condition.
Rehabilitation after cardiac stenting
Regular physical activity slows down the process of atherosclerotization and trains the cardiovascular system. Playing sports is one of the conditions for the speedy rehabilitation of the patient. Moderate physical activity increases the sensitivity of insulin receptors, accelerates lipolysis (fat burning) and stabilizes the level of total cholesterol in the blood.
It is worth establishing a clear daily routine - forming a dynamic stereotype. Try to do certain things at specific times: sleep, eat, exercise, work and rest. A stable daily routine will reduce the negative impact of stress factors on your life.
Aerobic workouts that will help make your heart stronger:
- fast walking (6-7 km/hour);
- Nordic walking (with poles);
- swimming;
- cycling (10-11 km/h);
- moderate running;
- morning work-out.
You should not engage in strength training, as this has a negative effect on the heart (risk of ventricular hypertrophy) and risks serious injury. Leading an active sex life is not prohibited, but in some cases it is not recommended.
Recommendations for healthy eating
After myocardial infarction, as well as after cardiac stenting, special attention is paid to diet. It is recommended to limit the intake of table salt (no more than 1 gram per day) and saturated fatty acids (pork, margarine and lard)
Saturated fats provoke atherosclerosis, and table salt increases blood pressure. A one-time increased intake of sodium chloride leads to an increase in the total volume of circulating fluid, and regular intake leads to hypertension.
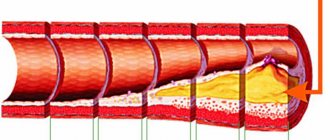
Cholesterol-rich foods and sweets are leading risk factors for atherosclerosis. Eggs, beef and lamb fat, chicken skin, pates, sausages, margarines and butter are the main sources of “bad” cholesterol (saturated fatty acids).
The body receives 15% of total cholesterol from food, and produces the remaining 85% itself. Atherosclerotic plaques are composed of cholesterol and calcium. The above products may be especially dangerous for those who have a hereditary predisposition to blood clots.
Life after stenting of cardiac vessels imposes certain restrictions on the intake of confectionery products. Sweets can stimulate blood clots in the blood vessels of the heart and cause a relapse of the disease. Sucrose (glucose and fructose) in large quantities can cause insulin resistance, another factor that has a detrimental effect on the heart.
Often, overeating can cause stabbing pain in the heart, especially in people suffering from angina pectoris. Severe pain in the chest after eating is a reason to consult your doctor.
It is important to avoid taking caffeine-containing medications because they stimulate the central nervous system. Caffeine is a mild stimulant of cardiac and bronchopulmonary activity
If you are a coffee lover, then you will have to live without it. It is dangerous because it can cause reperfusion arrhythmias. Large amounts of caffeine inhibit GABA and lead to overexcitation of the heart.
Coronary heart disease in diabetes mellitus
Almost all supporters of a healthy lifestyle and nutrition advocate a significant reduction in sugar and salt in the diet, rightly blaming an excess of these products for the aggravation of many diseases. Especially diabetes, hypertension and other obesity-related diseases. Are sugar and salt really that bad or are we just “not good at cooking them”?
In canned food and sausages, in juices and sweet drinks, in baked goods and fruits, not to mention such sweets as candies, cakes, baked goods, chocolate and others like them. That is, to eliminate the consumption of sugar and salt in the modern industrial world, you just need to stop eating altogether!
Expert opinion
Expert assessments in determining the strongest “pest” for our health vary greatly.
American scientists have identified the effect of sugar on the hypothalamus, which increases the number of heartbeats and blood pressure levels. They argue that a significant reduction in salt intake will lead to an overabundance of processed foods and sugars in the diet, and will also increase the content of certain types of fats in the blood, the level of which is restrained by the required amount of salt.
Experts from the University of New Zealand also came to the conclusion that sugar has a negative effect on heart function and hypertension. But recent research by Polish science has shown that sugar in small quantities, on the contrary, is beneficial and if a person is completely deprived of sugar, irreversible processes will begin in the body, which can end very badly.
The benefits of sugar
Sugar is a very energy-intensive product. And, of course, the ancient survival systems embedded in our brains cannot help but respond to such an amount of easily accessible energy. This explains our irresistible craving for everything sweet and sugar-containing.
And, if in underdeveloped countries and wild tribes this mechanism still serves to preserve life and health, then in developed countries, where food for the majority of the population is plentiful and easily accessible, the programming of the brain to consume foods such as sugars and fats has turned into its opposite and causes serious harm to the health of people who are unable to cope with the instincts inherent in nature.
However, sugar, consumed in limited quantities, is necessary and beneficial:
- Reduces the level of vascular sclerosis;
- Works as a prophylactic against thrombosis, slowing down the formation of atherosclerotic plaques;
- Sweet lovers are less likely to develop arthritis;
- Has a stimulating effect on the liver and spleen.
Sugar and blood pressure
Of course, sugar increases blood pressure. But this does not make him an enemy of all humanity. The effect of a rapid but short-term increase in pressure is widely used in cases of unexpected decrease in blood pressure in hypotensive patients.
Or when a donor donates a lot of blood, since it is vital at that moment. Then products with a high content of sugar and caffeine are not only not prohibited, but, on the contrary, are recommended for mandatory consumption.
A fatal “overdose” of sugar. It is precisely this formulation that can be applied to sugar, which, in its effect on humans, is comparable to hard drugs.
Of course, the human body, which is not engaged in heavy physical activity or intense brain activity at this time, is not able to expend so many calories and, like a zealous owner, it stores the rest for future use, synthesizing fat deposits from water and glucose.
This property of sugar is reflected in the saying: “A cake on the tongue for three minutes and a lifetime on the waist.” In addition, the feeling of fullness after sweets does not last very long and the body requires more and more portions of “sweet joy”, delivered to us by dopamine - the hormone of joy, which is produced by the adrenal glands, as a reward for the right choice of food, and we, falling into this vicious circle, gain “kilograms of happiness”, weighing heavily on our cardiovascular system and health.
DETAILS: What to do if it smudges. Why do my periods smear but not start?
Pressure surges caused by an excess of glucose raise blood pressure and force the pancreas to work in emergency mode, producing enough insulin to extract excess sugar from the blood, which inevitably leads to dysfunction of this important organ and to a number of diseases, including diabetes.
Sweets are also not good for tooth enamel. Combining with dental plaque containing bacteria, acids and food microparticles, sugar triggers an enhanced oxidative process, leading to enamel erosion with the development of caries and various periodontal lesions in the near future.
In a healthy person, the blood glucose level on an empty stomach corresponds to 3.2-5.5 mmol/l. After eating, the figure may increase to 7.7 mmol/l, which is also not a deviation from the norm. When blood for analysis is taken not from a finger, but from a vein, a level of 3.2-6.1 mmol/l is considered normal.
The norm varies depending on age:
- Up to 1 month - 2.8-4.4 mmol/l;
- From one month to 60 years - 3.2-5.5 mmol/l;
- From 61 to 90 years - 4.5-6.4 mmol/l;
- Over 91 years old - 4.2-6.7 mmol/l
During the examination, in order to make an accurate diagnosis, one should take into account only age, but also gender, current condition, history of diseases, as well as the emotional background of the patient.
2. To study the immediate and long-term results of coronary stenting in type 2 diabetes mellitus.
3. To compare the results of using bare stents and stents with antiproliferative coating “Cypher” in patients with diabetes mellitus.
4. Assess the role of clinical and morphological factors in the resumption of clinical angina in the long-term period after endoprosthetics of coronary arteries.
5. Determine treatment tactics for patients with coronary artery disease depending on the degree of coronary artery disease and the clinical course of diabetes mellitus.
This work is one of the first studies in the Russian Federation devoted to assessing the immediate and long-term results of coronary artery stenting in patients with diabetes mellitus. For the first time, using a fairly large material, a comparative assessment of the results of using Cypher drug-eluting stents and bare stents was given.
A decrease in the incidence of recurrent angina pectoris in the long term after implantation of sirolimus-eluting stents has been shown. An analysis of clinical and morphological factors influencing the rate of restenosis in the long-term period was carried out. Practical significance.
Indications for stenting in patients with type 2 diabetes have been developed, depending on the clinical features of diabetes and the morphology of coronary artery lesions. The data obtained will help optimize the criteria for selecting patients for arthroplasty. Basic provisions submitted for defense.
1. Stenting is an effective treatment method for patients with coronary artery disease with concomitant diabetes mellitus.
2. The high rate of resumption of angina in the long-term period in most cases is a consequence of restenosis due to the severity of diabetes mellitus and concomitant lipid metabolism disorders.
3. Morphological features of damage to the coronary arteries in diabetes mellitus (small reference diameter of the artery, diffuse lesions) are the leading factor influencing the rate of restenosis in the long-term period.
4. The use of stents with antiproliferative drug coating can significantly improve the long-term clinical effectiveness of endoprosthetics.
Implementation of research results.
The scientific principles and practical recommendations formulated in the dissertation were introduced into clinical practice and found application at the National Center for Cardiovascular Surgery named after. A.N. Bakulev RAMS. The results obtained can be recommended for implementation in clinical practice of cardiology and cardiac surgery centers in the country.
Publication of research results.
Nine scientific papers have been published on the topic of the dissertation, including one article and a chapter in a manual.
Approbation of dissertation material.
The main provisions were reported and discussed at the X, XI and XIII All-Russian Congresses of Cardiovascular Surgeons (Moscow, 2004, 2005, 2007), at the IX and X Annual Sessions of the Scientific Center for Cardiovascular Surgeons named after. A.N. Bakulev of the Russian Academy of Medical Sciences with the All-Russian Conference of Young Scientists (Moscow, 2005, 2006.
The dissertation is presented on 120 pages of typewritten text and consists of an introduction, five chapters, conclusions, practical recommendations, illustrations and a bibliography. The work is illustrated and provided with tables, diagrams, and drawings. The literature index includes 144 domestic and foreign sources.
Basic information about the presented work.
Inclusion criteria and clinical characteristics of patients.
— patients with coronary artery disease type 2 diabetes mellitus;
— angina pectoris and/or objective signs of myocardial ischemia;
- the presence of hemodynamically significant ({amp}gt; 50% in diameter) stenoses of the main epicardial coronary arteries;
- the primary nature of the narrowing of native coronary arteries;
- with acute myocardial infarction,
- severe congestive heart failure or pulmonary edema,
— with a previously performed coronary artery bypass surgery,
- with concomitant pathology of the cardiovascular system (valve-
significant heart defects, aortic aneurysm), requiring surgical treatment.
In accordance with these criteria, 100 of 178 patients with coronary artery disease with concomitant diabetes mellitus were included in the present study. The first group consisted of 40 patients who, during the period from January 1999 to June 2002, underwent stenting of the coronary arteries using stents without antiproliferative coating.
The second group consisted of 60 patients who, from June 2002 to September 2007, underwent endoprosthetics with implantation of stents with antiproliferative drug coating “Cypher” (“Cordis, Johnson{amp}amp;Johnson” USA).
Causes
With diabetes mellitus, especially if the second type, atherosclerosis develops. Moreover, the older the age, the more severe the narrowing of blood vessels. With stenosis, a sufficient amount of oxygen and nutrients is not delivered to the lower extremities, so pain occurs, which proportionally depends on the size of the lumen of the vessels
It is important to perform stenting in case of stenosis of 50%. This will not only help get rid of pain, but will also allow the vessel to maintain the necessary lumen for many years.
There are two courses of development of complications.
- Damage to the nerves of the legs due to constant high sugar. As a result, it is impossible to conduct a nerve impulse, which leads to loss of sensitivity, so nothing may hurt, but the process still progresses. This disease is called neuropathy.
- Progressive atherosclerosis, clogging blood vessels, contributes to the development of oxygen starvation. With this outcome, the pain syndrome is very pronounced. My legs hurt almost constantly.
The first course is dangerous because even the slightest microtrauma will go unnoticed, and weak immunity will lead to the development of an ulcer, the treatment of which will take a very long time.
Stenting technique
First of all, before surgery, the patient must undergo coronary angiography of the heart vessels - this is a diagnostic study using a contrast agent, which allows one to determine the exact location of the pathological process and narrowing of the artery lumen. After the location of the lesion has been established, the operation begins.
Instructions for stenting:
- before the intervention, the patient is administered intravenously a drug that reduces blood clotting;
- local anesthesia is administered to numb the area of skin where the incision will be made;
- a small incision or puncture is made in the right place, through which a catheter equipped with a special balloon is inserted into the lumen of the affected artery;
- the balloon reaches the exact location of the lesion, where it inflates on its own, thereby expanding the lumen of the artery;
- in place of the inflated balloon, under the control of an endoscope, the doctor installs a special filter, which will subsequently catch small blood clots and blood clots, preventing the development of a heart attack and stroke;
- another catheter equipped with an inflatable balloon is inserted into the puncture on the skin - as soon as the compressed balloon reaches the site of narrowing of the vessel, the structure expands, providing a powerful frame to the walls of the artery;
- all surgical instruments are removed, a sterile bandage or a small self-absorbing suture is applied to the intervention area (if a skin incision was made).
The duration of the procedure takes from 1 to 3 hours, all actions of the surgeon are controlled on the monitor screen. During the operation, the patient does not feel pain; it is unpleasant only at the moment when the balloon is inflated. The video in this article shows how the operation to install a stent is performed; the specialist talks in detail about this technique and types of stents.
Anesthesia for stenting
Most endovascular angioplasty procedures and lower extremity vascular stenting can be performed with mild intravenous sedation and local anesthesia at the access puncture site. Monitoring of blood pressure, electrocardiogram and blood oxygen saturation level (pulse oximetry) is mandatory. In case of unforeseen complications, the operating room is equipped with a breathing apparatus and a defibrillator. If the operation is performed for critical ischemia, then to make the patient comfortable, epidural anesthesia is performed (injection of an anesthetic drug through a catheter into the spinal area).
Treatment of coronary heart disease: balloon angioplasty, coronary stenting
Balloon angioplasty
This procedure, also called percutaneous transvascular coronary angioplasty (PTCA), uses a special balloon catheter to open a narrowed blood vessel. The balloon is inflated in the area of narrowing and, pressing the plaque into the wall of the vessel, opens the lumen of the coronary artery. This reduces the risk of myocardial infarction.
The procedure usually takes no more than an hour, and patients are discharged in the evening of the same day or the next morning.
Balloon angioplasty
- The first stages of angioplasty look the same as during the diagnostic procedure (preparation, insertion of a catheter and injection of a contrast agent).
- The doctor guides the guide through the catheter to the damaged area of the artery, watching it on the monitor(s)
- The balloon is inserted through the guidewire and placed at the site of blockage of the vessel (b).
- The balloon inflates, pushing plaque into the artery wall. The balloon may be inflated several times before it is removed (c).
- On the monitor, the doctor can see and evaluate the result. After the balloon is removed, the fat deposits remain pressed into the arterial wall, allowing blood supply to the heart to be restored (d).
According to statistics, repeated narrowing of the artery in the same place occurs in approximately half of patients. This phenomenon is called restenosis and occurs mainly 3 to 6 months after balloon angioplasty.
Implantation of a coronary stent
To reduce the risk of restenosis, your doctor may recommend a procedure called coronary stenting.
Implantation of a coronary stent
- In this procedure, a small balloon-expandable steel tube made of wire cells called a stent is placed in the affected area of the artery. The stent supports the walls of the artery, thereby improving blood supply to the heart.
- A stent attached to a balloon catheter is inserted into the artery and placed at the site of the blockage in the vessel (a).
- The balloon is then inflated. The stent expands and is pressed tightly into the arterial wall (b).
- Depending on the length of the narrowing, one or more stents may be needed. Using an x-ray, the doctor can make sure that the stent is placed correctly. To ensure that the stent has expanded correctly, the balloon may be inflated several times. Finally, the balloon is deflated and removed from the artery along with the guidewire and guiding catheter. The stent remains in the vessel permanently, keeping the artery open (c).
- After the procedure, the doctor will press with his hand the site where the catheter enters the artery.
If access was made through the arm, the doctor may apply a suture. Nurses will closely monitor your vital signs. If catheters were inserted in the groin area, you will be advised to rest in bed for several hours. Once you return to your room, you will be able to eat and drink as normal. Because the contrast agent used in the test is eliminated through the kidneys, you may urinate more frequently than usual.
The length of hospital stay depends mainly on the rate of healing of the arterial puncture site. Most patients are discharged the day after the procedure.
After returning home, you must strictly follow the doctor's recommendations. Take all medications prescribed to you and see your cardiologist regularly. Eat a low-fat diet
It is also very important to quit smoking and exercise regularly. The above lifestyle changes can help reduce the risk of heart disease
TBCA procedure
Preparation
After a preliminary examination (tests, ECG, ECHO, isotope diagnostics), you need to take a shower, shave the hair in the groin area (if accessed through the femoral artery). You should skip breakfast, or have a light breakfast. You need to have 1.5-2 liters of mineral water without gas and a new video cassette (or a blank CD with the ability to record).
Procedure
The duration of the procedure varies in each specific case, on average 1-2 hours.
The patient is taken to the angiography laboratory after preliminary premedication (im administration of sedatives). In the laboratory, the patient is placed on the surgical table and a cubital catheter is installed (in a vein in the arm).
The laboratory is kept sterile, so family and friends cannot be present during the procedure. Electrodes are placed on the arms and legs to continuously monitor the ECG. The puncture site is treated with an antiseptic, then an anesthetic (novocaine, lidocaine, etc.) is injected. The procedure is performed under local anesthesia. During anesthesia, the patient may feel a “tingling sensation of needles.” The necessary medications are administered through a cubital catheter. Remember - you can talk during the procedure, report any changes in your well-being to the doctor.
The entire procedure is carried out under X-ray control. A catheter with a balloon at the end is inserted through the puncture site and advanced towards the heart.
When the catheter reaches the site of stenosis, you may feel discomfort in the chest, this is normal. Pain may occur while inflating the balloon. The doctor may ask you to hold your breath for a few seconds.
After the procedure, the patient is transferred to the intensive care unit for dynamic monitoring of ECG, blood counts and puncture site. A small, flexible catheter (introducer) is placed in the artery for several hours, which is then removed by the doctor. A pressure bandage is applied to the puncture site. At this time, you are not allowed to bend your leg. The next day, the patient is transferred to the ward, the bandage is removed and allowed to walk.
You can eat and drink immediately after the procedure. It is recommended to drink 1-1.5 liters of mineral water for better removal of contrast.
The first few days after TBKA, you need to somewhat limit physical activity (load on the lower limbs).
This is what a stent looks like
Possible complications and risks.
If you follow your doctors' recommendations, the risk from the procedure is minimal. In case of complications, full assistance will be provided immediately (including emergency coronary bypass surgery).
Possible complications:
- Bleeding at the puncture site.
- Heart rhythm disturbances.
- Allergic reaction to contrast.
- Coronary artery thrombosis at the site of ballooning.
- Development of myocardial infarction.
After the procedure
The doctor may change the therapy (for example, cancel nitrates, beta blockers, prescribe drugs that affect blood clotting). Subsequently, we recommend periodic examinations - laboratory tests, ECG, stress test, isotope diagnostics, etc.
In some cases, coronary artery restenosis may occur. Therefore, if you feel chest pain, tell your doctor.
Remember that the TBKA procedure is the safest method of treating coronary heart disease and is increasingly used.
Rehabilitation after stenting of the coronary vessels of the heart
After undergoing arterial stenting, it is best for the patient to remain in bed for some time - this will reduce the likelihood of recurrent narrowing of the lumen of the vessels and reduce the risk of postoperative complications.
Life after stenting the coronary vessels of the heart involves undergoing cardiac rehabilitation, which is based on special dietary nutrition, a positive attitude and physical therapy.
Recovery after stenting of cardiac vessels, as a rule, occurs quickly, but for this the patient should strictly follow the recommendations of the attending physician, including:
- limit physical activity;
- refuse to take a bath for a while, only shower;
- do not lift weights weighing more than 3 kg;
- do not drive a car for 3-4 weeks after stenting;
- avoid stress and anxiety.
Exercise therapy after stenting of cardiac vessels
Physical therapy is prescribed to patients as early as 2 weeks after surgery. Exercises are prescribed for each individual individually by a cardiologist.
As a rule, these are not complex, moderate loads that help normalize blood pressure, weight, strengthen muscles and prevent heart attacks and strokes.
Diet
Since the main cause of the development of coronary heart disease and atherosclerosis is an unbalanced diet, and the absorption of food rich in fast carbohydrates and fats, a patient who has undergone coronary stenting should pay special attention to his diet. How to live after coronary stenting and what to eat? First of all, the following foods are completely excluded from the diet:
How to live after coronary stenting and what to eat? First of all, the following foods are completely excluded from the diet:
- margarine, lard, butter;
- baked goods;
- chocolate;
- pastries and cakes with rich cream;
- strong black coffee, tea;
- offal - brains, liver, kidneys;
- salo.
You should also limit your consumption of table salt and high-fat dairy products. Vegetable oils are used for cooking, and the dishes themselves are best prepared by stewing, boiling, or baking without a crust.
The basis of the diet is cereals, fresh vegetables and fruits, herbs, nuts, lean meats, fatty fish (mackerel, cod, salmon). It is fatty fish that are rich in polyunsaturated fatty acids, which prevent the formation of atherosclerotic plaques and blockage of arteries.
In order for the patient to feel well after stent installation, he must follow the doctor’s recommendations:
- take medications prescribed to prevent blood clots - usually Acetylsalicylic acid or Plavix;
- avoid surges in blood pressure - for arterial hypertension, medications that normalize blood pressure are prescribed;
- follow an anti-cholesterol diet and take medications that lower blood cholesterol levels;
- to live an active lifestyle.
As a conclusion, it should be noted that stenting of cardiac vessels is not a direct indication for the patient’s disability, however, if the condition is accompanied by other diseases that impair a person’s ability to work, then he may be given a referral to the VKK commission, where they will decide whether disability is necessary.
Possible complications
Complications after balloon angioplasty of the vessels of the lower extremities usually develop during the intervention and should be immediately eliminated. Methods for eliminating these complications are available to vascular surgeons. The most commonly observed complications are:
- Bleeding from the access site (hematoma or pseudoaneurysm) most often occurs when the patient violates bed rest. Sometimes requires open access to eliminate the source of bleeding.
- Puncture site infection is a very rare complication. It can develop with severe purulent-destructive processes on the lower limb. It is necessary to treat with antibiotics. If necessary, open the purulent focus.
- Contrast kidney injury is a rare complication from contrast media.
- Dissection (dissection) of the artery - sometimes observed with complex lesions and attempts at subintimal passage. Most often it can be eliminated by installing a stent.
- Blockage of the arterial bed with pieces of plaque can be determined during control angiography.
- Fracture of the stent in the places where it bends is a late complication associated with mechanical stress on the metal.
- Repeated narrowing at the site of stent installation (restenosis) is the process of overgrowth of the lumen of the stented segment.
- Arterial rupture is a complication that develops due to excessive balloon inflation in a severely calcified vessel. Detected during control angiography. It is often possible to stabilize the situation with prolonged exposure of the balloon; installation of a stent graft or open surgery may be required.
- Arterial spasm is a reaction to inflating a vessel with a balloon. Occurs in 10% of procedures. To eliminate spasms, medications (papaverine, nitroglycerin) can be administered.
The frequency of all complications is no more than 5% of all procedures performed and they are usually eliminated in a timely manner during the intervention.
Comparison of stenting and bypass surgery: their pros and cons
If you compare what is better – stenting or bypass surgery, you first need to decide how they differ.
Stenting, unlike bypass surgery, is an endovascular method and is performed without opening the chest and making large incisions. Bypass surgery is most often a cavity operation. On the other hand, installing a shunt is a more radical method that allows you to cope with stenosis with multiple blockages or complete occlusion. Stenting in such situations is often useless or impossible.
Principle of heart bypass
Stenting is most often used to treat young patients with minor vascular changes. Elderly patients with serious lesions are still advised to install a shunt.
During a stenting operation, local anesthesia is sufficient, but when installing a shunt, it is necessary not only to use general anesthesia, but also to connect the patient to a heart-lung machine.
The risk of blood clots after stenting forces patients to take special medications for a long time. In addition, restenosis is also possible. New generations of stents, of course, help solve these problems, but, nevertheless, this happens. Shunts are also not ideal - they, like any vessels, are subject to degenerative processes, atherosclerosis, etc., so after some time they can fail.
Recovery times also vary. After minimally invasive stenting, the patient can leave the clinic the very next day. Bypass surgery involves a longer period of recovery and rehabilitation.
Types of stents and their features
A stent is a cylindrical spring made of a special metal or plastic. It is introduced into the affected vessel in a compressed form and expanded into the desired location using a balloon into which pressure is applied. The balloon is then removed, and the spring remains in place, holding the vascular wall.
Types of stents differ in design, as well as in the material from which they are made.
The following designs are used in cardiac surgery:
- Made from thin wire, they are called wire;
- Consisting of individual links in the form of rings;
- Representing a solid tube - tubular;
- Made in the form of a grid.
In acute conditions (during a heart attack or an attack of unstable angina), bare metal stents are more often used. They are used when the narrowing of the coronary arteries does not reach a critical level and the likelihood of further stenosis is low.
Drug-eluting stents
There are several types of such stents. They are metal structures with a polymer coating, on which is applied a layer of medication that inhibits the growth of vascular tissue.
Gradually, this medicine enters the body, and the polymer dissolves. What remains is a metal frame that supports the walls of the artery. Biocompatible drug-eluting stents are widely used in European and Russian clinics.
Biosoluble coated stent
Stand resorption time
The atherosclerotic plaque, previously destroyed by a special balloon, must heal so that blood clots do not form on it. In the period from 3 to 6 months, the stent “works”, releasing a medicine that heals the endothelium of the vessel (inner lining) and prevents it from growing pathologically.
The scaffold is made of the finest metal mesh (almost 20 times thinner than a human hair) with a biosoluble polymer coating. After six months, the structure is completely covered with endothelium, and the polymer coating containing the drug dissolves. As a result, normal lumen is maintained in the artery, and its walls remain elastic.
Stenting for diabetes in Germany, Frankfurt
Russian Medical Server / German Clinic Sachsenhausen / Stenting for diabetes mellitus in the German Clinic Sachsenhausen
Treatment of diabetes mellitus in a specialized clinic in Germany, Frankfurt
Diabetes mellitus is one of the most common causes of early and severe vascular damage. Often their pathology appears long before other symptoms in patients who are unaware of their illness. Rapid progression of atherosclerosis of the arteries of the heart and lower extremities, especially against the background of hypertension, is a typical picture.
For example, diabetes mellitus of any type increases the risk of coronary heart disease (CHD) by 4-6 times, and every second of the patients newly diagnosed with diabetes mellitus already suffers from CHD, and dangerous asymptomatic and painless forms.
Atherosclerotic stenosis of the arteries of the lower extremities is the cause of severe ischemic complications of diabetes, leading to amputations.
Therefore, restoring the patency of the arterial bed in diabetes is an urgent need. Arterial stenting is one of the components of complex comprehensive treatment for these patients. It has undoubted advantages for them. After all, the majority have absolute or relative contraindications to “major” operations with general anesthesia and extensive opening of tissues and body cavities.
Arterial stenting is a minimally invasive intervention. It is performed through a puncture of the artery, under local anesthesia. All other stages of the operation take place inside the vessels, under the control of X-ray angiography, and are completely painless.
First, radiography of the vessels is performed with a contrast agent, and after their visualization, a stent is carried out and installed using a catheter in the area of narrowing. This is a special mesh metal structure that expands the area of stenosis and fixes it in this position, ensuring normal blood flow.
Such operations, being very effective, are much easier for patients to tolerate than traditional open interventions.
Therefore, they are always indicated when there are technical possibilities for restoring blood circulation in this way, and there is no effect from conservative treatment.
They are the method of choice in cases of critical ischemia of the myocardium or limbs, as they ensure rapid disappearance of clinical manifestations of vascular complications.
Another advantage is that stenting operations can be performed repeatedly, and in patients with diabetes this need arises quite often.
This is due to specific, so-called proliferative processes in the vascular wall, characteristic of this group of patients.
Due to the proliferation of the inner linings of the vascular wall, their risk of restenosis (re-narrowing of the vessel) is increased.
Stenting in patients with diabetes mellitus has its own characteristics:
- in more than 70% we see multiple arterial lesions;
- more than 80% are structurally unfavorable lesions;
- in the long-term period, the frequency of relapse of angina pectoris and ischemia of the lower extremities due to repeated stenosis is high;
- the risk of restenosis is increased by increased cholesterol levels, a large length of the primary stenotic segment and small diameter of the arteries, therefore, after stenting, strict control of the lipid spectrum and glycemia is necessary;
- after coronary stenting, control angiography to detect restenosis is performed no later than a year later, and in case of relapse of angina - earlier;
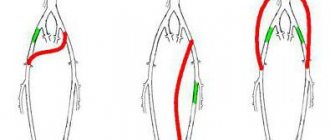
- Most patients with damage to the peripheral arteries of the lower extremities have critical ischemia: they cannot walk more than 25 meters without pain and have trophic disorders of the feet. They have extended, more than 10 cm, and multiple stenoses and occlusions (areas of complete obstruction) of the leg arteries;
- Stenting of the arteries of the lower extremities is performed if several segments of the popliteal artery and at least one artery of the leg are patent;
- for successful stenting, the distance between occlusion and stenosis must be at least 3 cm;
- preoperative antiplatelet therapy for several months is required;
- more effective treatment of short areas of stenosis;
- eliminating occlusions is problematic, but if they can be passed with a catheter, long-term results do not differ from the results of treating stenosis (partial narrowing).
The use of new generation stents that release the drug over a long period of time has made it possible to reduce the frequency of restenosis by almost 2 times.
CYPHER drug-eluting stents release sirolimus. This drug suppresses proliferative processes in the arteries, which are so characteristic of patients with diabetes.
As a result, the need for repeated operations due to developed restenosis is significantly reduced.
At the Sachsenhausen Clinic in Frankfurt, diabetic patients requiring stenting are supervised by doctors from the Diabetology Center and the Clinic's Center for Angiology, Interventional Cardiology and Radiology.
Therefore, even in the most difficult cases, they receive high-tech, effective, comprehensive assistance.
Thus, the clinical effectiveness of stenting of coronary arteries in such patients is 97%, and of peripheral arteries – 95% in the first year after surgery.
+7 – treatment at the German clinic Sachsenhausen
REQUEST TO THE CLINIC
Source: https://www.rusmedserv.com/zaksenhauzen/StentingDiabetes/
Rehabilitation period
Rehabilitation after stenting includes a set of measures that will help a person recover faster and reduce the risk of relapse of the disease. Immediately after the operation, the patient must observe strict bed rest in a hospital setting (1-2 days). During this time, the attending physician constantly monitors the person’s condition. When the patient is discharged, he should provide himself with maximum peace at home. Physical activity is prohibited at first. In addition, after stenting, you should not take a hot shower/bath.
Rehabilitation after stenting involves taking medications prescribed by your doctor. With the help of medications, the risk of developing myocardial infarction is significantly reduced, and indicators such as life expectancy and quality of life with coronary heart disease increase. The duration of the course is on average up to six months. The list of prescribed drugs after vascular stenting includes:
- reducing the amount of cholesterol in the blood;
- antiargents;
- anticoagulants.
During the rehabilitation period, it is important to follow a diet. Fatty foods should be limited in a person's diet
If you have hypertension, you should avoid salt. If the patient suffers from diabetes, his diet should contain exclusively products of the ninth table according to Pevzner. Obese people should reduce their calorie intake as much as possible.
A person who has undergone stenting of the heart vessels should regularly perform exercise therapy (physical therapy) 1-2 weeks after the operation. Rules:
- The ideal option is walking. Light homework shown.
- The duration of exercise should be limited to 30-40 minutes and carried out daily.
- A health path is considered an excellent rehabilitation tool - climbing limited in time, angle of inclination and distance along specially organized routes.
- Exercises promote gentle training of the heart and gradually restore its function.
What diseases cause the device to deteriorate quickly?
Rapid deterioration of stents occurs under the influence of three main factors:
- Violation of the vascular wall is generally nonspecific for any diseases and develops when the vascular endothelium covers the stent too intensively, leading to a narrowing of the lumen of the vessel.
- Blood clotting disorders can occur due to external factors (overheating, dehydration) or against the background of chronic diseases (atherosclerosis, fermentopathy, parasitic infestations, chronic liver diseases).
- Slowing of blood flow is mainly accompanied by an attack of angina pectoris and is explained by spasm of small vessels that provide blood flow to the heart muscle.
Diabetes mellitus is regarded by doctors as a disease that can lead to accelerated stent deterioration, but the presence of diabetes is not a contraindication to intervention.
Patients with uncompensated diabetes mellitus are in most cases denied stenting, as the risk of complications is high.